You might also like
- Anaphylaxis: A Practical GuideFrom EverandAnaphylaxis: A Practical GuideAnne K. EllisNo ratings yet
- Upper Respiratory Tract Infections Group 1 BSN 2.3Document57 pagesUpper Respiratory Tract Infections Group 1 BSN 2.3Joedelynne Diane Endaya GarciaNo ratings yet
- Anatomy and Physiology of The Respiratory System: Basco, Kimberly BSN-2Document5 pagesAnatomy and Physiology of The Respiratory System: Basco, Kimberly BSN-2Cxazandra Kaith CasasNo ratings yet
- 6.upper Airway DiseaseDocument7 pages6.upper Airway Disease2BGrp3Plaza, Anna MaeNo ratings yet
- Common Disorde Rs in ChildrenDocument172 pagesCommon Disorde Rs in Childrenblacklilha100% (1)
- Respiratory Disorders: Parainfluenza, RSV, RhinovirusDocument5 pagesRespiratory Disorders: Parainfluenza, RSV, RhinovirusSoojung Nam100% (1)
- Finals LecDocument14 pagesFinals LecSheena Patricia ArasulaNo ratings yet
- Childhood Respiratory Infections GuideDocument6 pagesChildhood Respiratory Infections GuideBg NatzzNo ratings yet
- Case - Study (PCAP)Document27 pagesCase - Study (PCAP)Cherry Ann BalagotNo ratings yet
- NCM109 - Reviewer-Lp-1-To-Lp-4Document54 pagesNCM109 - Reviewer-Lp-1-To-Lp-4princessNo ratings yet
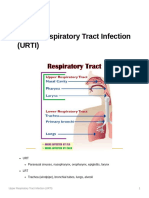
- 8 - Upper Respiratory Tract Infection (URTI)Document21 pages8 - Upper Respiratory Tract Infection (URTI)Kaela Beatrice Sy LatoNo ratings yet
- Respiratory EmergenciesDocument30 pagesRespiratory EmergenciesNovriefta NugrahaNo ratings yet
- Respiratory Tract InfectionsDocument17 pagesRespiratory Tract InfectionsPriya bhattiNo ratings yet
- Acute Tracheobronchitis Causes, Symptoms, TreatmentDocument2 pagesAcute Tracheobronchitis Causes, Symptoms, TreatmentNicole Shannon CariñoNo ratings yet
- URTIDocument41 pagesURTIGetaneh LiknawNo ratings yet
- NCM 109Document18 pagesNCM 109Grace Jane HannaNo ratings yet
- Ewag - PHMP ReviewerDocument12 pagesEwag - PHMP ReviewerKyla Charlotte EwagNo ratings yet
- Upper Respiratory Infections: Symptoms and TreatmentsDocument45 pagesUpper Respiratory Infections: Symptoms and TreatmentsNatasha Abdulla100% (2)
- Pulmonary and Respiratory Nursing Assessment GuideDocument48 pagesPulmonary and Respiratory Nursing Assessment GuideEmjay JapitanaNo ratings yet
- Adenovirus, Influenza, RSV, CMV, Parainfluenza, EBV: Most CommonDocument2 pagesAdenovirus, Influenza, RSV, CMV, Parainfluenza, EBV: Most CommonSoojung NamNo ratings yet
- Lesson Notes On UrtiDocument9 pagesLesson Notes On UrtiNeethupaulNo ratings yet
- 1.acute Respiratory Disease: DDX: Kawasaki, Strep. InfectionDocument5 pages1.acute Respiratory Disease: DDX: Kawasaki, Strep. InfectionSheryl Layne Lao-SebrioNo ratings yet
- Common Cold - : Etiologic Agent-Most Commonly Rhinovirus. 50 % of Infections. Persistence of Nasal CongestionDocument2 pagesCommon Cold - : Etiologic Agent-Most Commonly Rhinovirus. 50 % of Infections. Persistence of Nasal CongestionStewart Garneth Reston RancesNo ratings yet
- MEDSURGDocument7 pagesMEDSURGVal FielNo ratings yet
- NCM 112 Study Guide MidtermDocument42 pagesNCM 112 Study Guide MidtermMark Nathaniel ValerioNo ratings yet
- Nursing Care of A Child With Respiratory DisorderDocument69 pagesNursing Care of A Child With Respiratory DisorderTamil Villardo100% (1)
- Ch 150 Management of Cough in Office PracticeDocument8 pagesCh 150 Management of Cough in Office Practiceroshen02No ratings yet
- App To CHR CoughDocument6 pagesApp To CHR Coughbrajendra singhNo ratings yet
- CcroupDocument53 pagesCcroupOlivia BernadiNo ratings yet
- q3 HealthDocument54 pagesq3 HealthGenelyn Lucena Hurtada LabindaoNo ratings yet
- Common Health Problems of Infancy PowptDocument78 pagesCommon Health Problems of Infancy PowptCiella Dela CruzNo ratings yet
- Pedia Rotation CroupDocument2 pagesPedia Rotation CroupKaren ArandiaNo ratings yet
- Respiratory DisordersDocument15 pagesRespiratory DisordersStephanie LeeNo ratings yet
- Disorder of ThroatDocument21 pagesDisorder of ThroatSumit YadavNo ratings yet
- Acute Respiratory Infection: Darmawan B SetyantoDocument84 pagesAcute Respiratory Infection: Darmawan B SetyantonurhasanahNo ratings yet
- AsthmaDocument15 pagesAsthmaDiana HuañecNo ratings yet
- Chapter 17Document19 pagesChapter 17Patricia VasquezNo ratings yet
- ENT LESSON 4 (1)Document64 pagesENT LESSON 4 (1)favourednancie9No ratings yet
- Bronchial AsthmaDocument20 pagesBronchial AsthmaJuliet De GuzmanNo ratings yet
- Bronchopneumonia Nursing CareDocument24 pagesBronchopneumonia Nursing CareRickyNo ratings yet
- Nursing Management of Children With Respiratory System DysfunctionsDocument27 pagesNursing Management of Children With Respiratory System DysfunctionsDody ZainNo ratings yet
- Avian Flu and H1N1Document14 pagesAvian Flu and H1N1Fleurellei SantosNo ratings yet
- Bronchitis: Presented By:-Himanshi B. B. Sc. (N) 3 Year Gcon (Tehri)Document29 pagesBronchitis: Presented By:-Himanshi B. B. Sc. (N) 3 Year Gcon (Tehri)HimanshiNo ratings yet
- Upper RespiratoryDocument51 pagesUpper RespiratoryMelanie D'artistNo ratings yet
- Pediatrics - Lower AirwayDocument3 pagesPediatrics - Lower AirwayJasmine KangNo ratings yet
- Leaflet IspaDocument2 pagesLeaflet IspareviyanaNo ratings yet
- Requirement in NCM 312: Submitted By: Jaylee C. Andaya Submitted To: Dr. Ma. Lynne C. ParambitaDocument8 pagesRequirement in NCM 312: Submitted By: Jaylee C. Andaya Submitted To: Dr. Ma. Lynne C. ParambitaChloie Marie RosalejosNo ratings yet
- Anatomy and Infections of the Respiratory TractDocument5 pagesAnatomy and Infections of the Respiratory TractNinaNo ratings yet
- Upper Respiratory Tract InfectionDocument43 pagesUpper Respiratory Tract InfectionNaresh JoshiNo ratings yet
- URI-ppt 03Document111 pagesURI-ppt 03tinsjohnNo ratings yet
- Urti 1 14Document14 pagesUrti 1 14Ahsan kamalNo ratings yet
- Oxygenation ReviewerDocument8 pagesOxygenation ReviewerDamie FernandezNo ratings yet
- Child Health Nursing Teaching Staff Respiratory DisordersDocument47 pagesChild Health Nursing Teaching Staff Respiratory DisordersSimaNo ratings yet
- Common ColdDocument1 pageCommon ColdLalisaM ActivityNo ratings yet
- Upper Respiratory Tract InfectionsDocument26 pagesUpper Respiratory Tract InfectionsZyrene RiveraNo ratings yet
- Respiratory Emergency and DiseasesDocument5 pagesRespiratory Emergency and DiseaseshanhananicasNo ratings yet
- Croup Syndrome Nursing Care Planning and Management - Study Guide PDFDocument18 pagesCroup Syndrome Nursing Care Planning and Management - Study Guide PDFSanket TelangNo ratings yet
- StridorDocument48 pagesStridorMahindra Kumar100% (1)
- Opd) Ba) CSDocument7 pagesOpd) Ba) CSFerreze AnnNo ratings yet
- Flash CardDocument2 pagesFlash CardRoy CabuenasNo ratings yet
- The Potential of Organometallic Complexes in Medicinal Chemistry PDFDocument8 pagesThe Potential of Organometallic Complexes in Medicinal Chemistry PDFArijit dasguptaNo ratings yet
- Overrating or Dismissing The Value of Evidence-Based Practice+++Document7 pagesOverrating or Dismissing The Value of Evidence-Based Practice+++pig5evans30No ratings yet
- Pharmacology Questions MGR Medical UniversityDocument40 pagesPharmacology Questions MGR Medical UniversityPONNUSAMY PNo ratings yet
- Dexmedetomidine FAQDocument16 pagesDexmedetomidine FAQRoxana SurliuNo ratings yet
- Puerperal InfectionDocument28 pagesPuerperal InfectionAgus PratiwaNo ratings yet
- Ten Days in A Mad-House by Nellie BlyDocument122 pagesTen Days in A Mad-House by Nellie BlyCharmaineTanti100% (1)
- Pharmacy Policy and ProceduresDocument15 pagesPharmacy Policy and ProcedureswilliamNo ratings yet
- Yimi Catalogue2014Document60 pagesYimi Catalogue2014ariovaldofjNo ratings yet
- Charges and Optical Voucher ValuesDocument12 pagesCharges and Optical Voucher ValuesAnonymous hnk5L17No ratings yet
- Active Aging - A Policy FrameworkDocument60 pagesActive Aging - A Policy FrameworkJulie HenriNo ratings yet
- The Pittston Dispatch 08-05-2012Document62 pagesThe Pittston Dispatch 08-05-2012The Times LeaderNo ratings yet
- MometasoneDocument2 pagesMometasoneGilang infNo ratings yet
- Hospital Statistics Report On 8.5.2020Document4 pagesHospital Statistics Report On 8.5.2020vaideeswari kumarNo ratings yet
- The Concept of Plants As TeachersDocument18 pagesThe Concept of Plants As TeachersAya Greengo100% (1)
- ThegreatgatsbyDocument6 pagesThegreatgatsbyapi-287109554No ratings yet
- Blue Book 2023Document193 pagesBlue Book 2023YS NateNo ratings yet
- A Study To Assess The Patient's Satisfaction On Nursing Care in Emergency DepartmentDocument3 pagesA Study To Assess The Patient's Satisfaction On Nursing Care in Emergency DepartmentIOSRjournalNo ratings yet
- Amikacin Drug StudyDocument4 pagesAmikacin Drug StudyMark Angelo LorzanoNo ratings yet
- Ketamine Presentation - PPT RevisedDocument31 pagesKetamine Presentation - PPT RevisedJack TanNo ratings yet
- Anatomy StomachDocument43 pagesAnatomy StomachBijo K BennyNo ratings yet
- Phaco Chop: Roger F. Steinert, MDDocument9 pagesPhaco Chop: Roger F. Steinert, MDMichael CraneNo ratings yet
- Power Up Your Primary Care Coding by Nikki TaylorDocument21 pagesPower Up Your Primary Care Coding by Nikki TaylorsupercoderNo ratings yet
- Dec 2010Document94 pagesDec 2010Faiz DhmNo ratings yet
- Ticagrelor Vs Aspirin in Acute Stroke or Transient Ischemic AttackDocument28 pagesTicagrelor Vs Aspirin in Acute Stroke or Transient Ischemic AttacklucasNo ratings yet
- Informed Consent - Filler - RadiesseDocument7 pagesInformed Consent - Filler - RadiesseAshraf AboNo ratings yet
- Managing The Red EyeDocument92 pagesManaging The Red EyeisabelleNo ratings yet
- Yoga Healthy Heart GuideDocument100 pagesYoga Healthy Heart GuidePralesh12No ratings yet
- Babies Die From Lack of TouchDocument3 pagesBabies Die From Lack of Touchkbarn389No ratings yet
- Hagerman - Training The Energy SystemsDocument8 pagesHagerman - Training The Energy Systemsmkn1214100% (1)
- Care Plan - Ineffective MobilityDocument10 pagesCare Plan - Ineffective MobilityAshley ToppNo ratings yet