The permit is automatically suspended on activation of the General Alarm or Instruction via Notification Alarm.
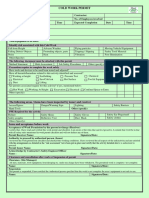
COLD WORK PERMIT
WORK PERMIT NUMBER CWP - PERMIT ISSUED TO SUBCONTRACTOR Yes □ No □
DIVISION / SUBCONTRACTOR NAME MANPOWER
1 A TASK DESCRIPTION
Task/Work Description
Location/Area
Validity Period
Work Shift □ Day Shift □ Night Shift
Days Date From To From To
(Working Duration)
Time From To From To
B HAZARD IDENTIFICATION & RISK ASSESSMENT
Description of Possible Hazards □ Work at Height □ Adjacent Work □ Lifting Operations □ Unauthorized Entry □ Moving Parts □ Rotating Machinery
□ Flying Particles □ Slippery Surface □ Isolations □ Cables / Hoses □ Chemical Handling □ Lifting/Manual Handling
□ Vehicle Movement □ High Noise □ Equipment Hazard □ Spillage □ High Pressure □ High Temperature
□ Others
Attachment required □ HEMP □ Risk Assessment □ Method Statement(MS) □ Drawings □others ______________
CONTROLS
ORIGINATOR / PERFORMING AUTHORITY
C
Required Control measures: Yes No N/A Other Control Measures: Yes No N/A
Safe Access / Work Platform available □ □ □ Cables / Hoses without damage and Safe End Connection □ □ □
Fall Protection System □ □ □ Trolley, Equipment in place for minimizing Manual Handling □ □ □
Hard / Soft Barrier □ □ □ Banksman Assigned to Control Vehicle Movement & Reverse Operation □ □ □
Certified Equipment, Tools and Operator for Lifting Operations □ □ □ Spill Kits Available □ □ □
No Work under suspended load □ □ □ Pipe, Hose and other connections secured for High Pressure □ □ □
Rotating Machinery Guards In Place □ □ □ Heat Stress Control Measure □ □ □
Guards / Shield in place for Preventing Flying Particles □ □ □ Gas Test (if "Yes" go to D) □ □ □
Barrication and Signs for Slippery/Wet Surface □ □ □ Confined Space Entry (if "Yes" go to )F □ □ □
LOTO (Logout/Tagout), if 'Yes' check Isolation work permit □ □ □ Override of HSE Critical devices (if "Yes" go to ) F □ □ □
PPE Required (Check the box if required) ;
Safety Helmet □ □ □ Face shields □ □ □
Safety Goggles □ □ □ Cartridge Respirator □ □ □
Safety Shoe / Boots □ □ □ Hood (□ Welding, □ Blasting, □ Others) □ □ □
Glove s(□ Cotton, □ Leather, □ Nitrile,□ IR) □ □ □ Chemical/Fire Resistant Clothing □ □ □
Full Body Safety Harness and Double lanyard □ □ □ Ear Plug / Ear Muff □ □ □
Actions & Other Precautions:
D GAS TEST ( If additional gas tests are required, use the Additional Gas Tests Form )
Toxic
Gas Test Parameter Flammable Oxygen
Date Time Gas Tester Name H2S CO Ammonia SO2 Others Remarks
Safe Limits < 1% LEL 23.5%<O2> 19.5% < 10 ppm < 35 ppm < 25 ppm < 2 ppm
Test Results
Test Results
Test Results
2
E CROSS REFERENCES & ACKNOWLEDGMENT F PERMITS & CERTIFICATES REQUIRED
ORIGINATOR/AREA
SUPERVISOR
Other permits in area that Yes □ No □ Details: Other Permits or Certificates Required Yes □ No □
could interfere: [SIMOPS] Confined Space Work Permit Number
Acknowledgement from Electrical Work Permit Number
Affected Parties [SIMOPS] Isolation Certificate Number
3 DESCRIPTION PERFORMING AUTHORITY AREA SUPERVISOR ISSUING AUTHORITY HSE TEAM (AOTC)
I understand and accept the above conditions and precautions and accept I declare that all hazards have been identified and all specified control The Permit and any supplementary certificates have been completed. The For check, Compliance and Record
Acknowledgement responsibility for the work and ensure the persons under my control measures are in place and it safe to carry out the work defined control measures defined are in place.
understand and comply with these conditions and precautions
ISSUE
Name
Sign
Date/Time
CHECK
PERFORMING AUTHORITY AREA SUPERVISOR ISSUING AUTHORITY HSE TEAM (AOTC)
CANCELATION
EXTENSION
4
DATE TIME
D NAME SIGN NAME SIGN Name SIGN NAME SIGN
□ □
EXTENSION OR CANCELLATION
□ □
□ □
□ □
□ □
□ □
5 DESCRIPTION PERFORMING AUTHORITY AREA SUPERVISOR ISSUING AUTHORITY HSE TEAM (AOTC)
I declare that the work has been properly performed and that the I have inspected the equipment/work area and declare that the work All copies of Permit & any supplementary certificates collected. The control For check, Compliance and Record
Acknowledgement equipment, plant and apparatus affected by the work have been left in a defined in this permit is complete and that the area is clean and safe. measures put in place for this permit have been removed.
safe, clean condition
COMPLETION
Name
Sign
Date/Time
Document Tag: AOTC-IMS-L4-301-F-001 | Rev:01 | Date: 10-01-2021