You might also like
- O Que É TareDocument1 pageO Que É Tarejacyellen pereira da silvaNo ratings yet
- Tridimensional DGDocument9 pagesTridimensional DGDalilaNo ratings yet
- Arfid Tea Eval y ManejoDocument7 pagesArfid Tea Eval y ManejoDalilaNo ratings yet
- Prevalence and Characteristics of Avoidant/Restrictive Food Intake Disorder in Adult Neurogastroenterology PatientsDocument30 pagesPrevalence and Characteristics of Avoidant/Restrictive Food Intake Disorder in Adult Neurogastroenterology Patientsalexandra robuNo ratings yet
- FisherDocument4 pagesFisherNelson Syah HabibiNo ratings yet
- AFRIDarticle2020 Davis StoneDocument6 pagesAFRIDarticle2020 Davis Stonepico 24No ratings yet
- Eating Disorders in Children and Adolescents: Nina K. Anderson, and Olivier F. NicolayDocument4 pagesEating Disorders in Children and Adolescents: Nina K. Anderson, and Olivier F. NicolayParameswaran ManiNo ratings yet
- Mairs R Et Al 2016Document8 pagesMairs R Et Al 2016Camilla ValeNo ratings yet
- Intl J Eating Disorders - 2020 - Hilbert - Psychometric Evaluation of The Eating Disorders in Youth Questionnaire When UsedDocument10 pagesIntl J Eating Disorders - 2020 - Hilbert - Psychometric Evaluation of The Eating Disorders in Youth Questionnaire When UsedKariena PermanasariNo ratings yet
- Prevalence and Characteristics of Avoidant/ Restrictive Food Intake Disorder in A Cohort of Young Patients in Day Treatment For Eating DisordersDocument8 pagesPrevalence and Characteristics of Avoidant/ Restrictive Food Intake Disorder in A Cohort of Young Patients in Day Treatment For Eating DisordersAhmad Tri Anggara SasmitaNo ratings yet
- 10 1016@j Jand 2020 10 017 PDFDocument26 pages10 1016@j Jand 2020 10 017 PDFNatália GiovanaNo ratings yet
- Nutritionalproblems Affectingolderadults: Neva L. CroganDocument13 pagesNutritionalproblems Affectingolderadults: Neva L. CroganALBERTO LUIS LIZCANO GONZALEZ ESTUDIANTENo ratings yet
- Holly A HarrisDocument7 pagesHolly A HarrisRemy MohammedNo ratings yet
- Eriatric Nutrition: A Prosthodontic Review: AsssaasasasssDocument5 pagesEriatric Nutrition: A Prosthodontic Review: AsssaasasasssMaqbul AlamNo ratings yet
- 2021 REVIEW Dysphagia Texture Modification The Elderly and Micronutrient DeficiencyDocument17 pages2021 REVIEW Dysphagia Texture Modification The Elderly and Micronutrient DeficiencyJuan P. CortésNo ratings yet
- 1 s2.0 S0140673622026125 MainDocument16 pages1 s2.0 S0140673622026125 MainCaylynn WoWNo ratings yet
- 10 1002@eat 23236Document12 pages10 1002@eat 23236LucíaNo ratings yet
- Eating Disorders in The Adolescent PatientDocument15 pagesEating Disorders in The Adolescent PatientThaily MoralesNo ratings yet
- Eating Disorders and Its Dental ImpactDocument4 pagesEating Disorders and Its Dental ImpactInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Nutritional Epidemiology-Past, Present, Future: EditorialDocument3 pagesNutritional Epidemiology-Past, Present, Future: Editorialisabel sedanoNo ratings yet
- ARFID ZimmermanDocument3 pagesARFID ZimmermanSaray De la TorreNo ratings yet
- Arfid, 2017Document9 pagesArfid, 2017Camilla ValeNo ratings yet
- TangDocument16 pagesTangEvelynNo ratings yet
- Early Detection of Eating Disorders in General PracticeDocument7 pagesEarly Detection of Eating Disorders in General PracticeManny RosengallegosNo ratings yet
- A Guide To Selecting Evidence-Based Psychological TherapiesDocument19 pagesA Guide To Selecting Evidence-Based Psychological Therapiesangela cabrejosNo ratings yet
- Anorexia of Aging and Its Role For FrailtyDocument7 pagesAnorexia of Aging and Its Role For FrailtyBruno Limaverde LoboNo ratings yet
- Artículo de La EpidemiologiaDocument3 pagesArtículo de La EpidemiologiaPaulaNo ratings yet
- Intervencoes Nutricionais No TEA 2019 OxfordDocument17 pagesIntervencoes Nutricionais No TEA 2019 OxfordalinecanavezNo ratings yet
- Nutrición Personalizada para Prevención de DemenciaDocument14 pagesNutrición Personalizada para Prevención de DemenciaMelisa RieloNo ratings yet
- Jurnal Nutrisi 4Document16 pagesJurnal Nutrisi 4agung suprasthaNo ratings yet
- Eating Disorders: Evaluation and Management: Key PointsDocument21 pagesEating Disorders: Evaluation and Management: Key PointsCassandra BoduchNo ratings yet
- Avoidant Restrictive Food Intake Disorder: An Illustrative Case ExampleDocument4 pagesAvoidant Restrictive Food Intake Disorder: An Illustrative Case ExampleAnonymous fPQaCe8100% (1)
- Nutritional Interventions PDFDocument17 pagesNutritional Interventions PDFLalit MittalNo ratings yet
- Page 2021Document20 pagesPage 2021maria cristina aravenaNo ratings yet
- Reporte de Caso TERIA AdultoDocument4 pagesReporte de Caso TERIA AdultoLautaro FerreiraNo ratings yet
- Eating Disorders and Their Implications On Oral Health - Role of DentistsDocument6 pagesEating Disorders and Their Implications On Oral Health - Role of DentistsThaily MoralesNo ratings yet
- Artigo 1 1Document17 pagesArtigo 1 1Millena CristinaNo ratings yet
- Lit Review - Eating DisorderDocument4 pagesLit Review - Eating DisorderAlien4mearthNo ratings yet
- Malnutrition in Older Adults: Screening and DeterminantsDocument8 pagesMalnutrition in Older Adults: Screening and DeterminantsDaniela Aguilar SánchezNo ratings yet
- PS 305 Milestone 2Document2 pagesPS 305 Milestone 2Ashika LataNo ratings yet
- Diagnosis and Evaluation of Eating Disorders in The Pediatric PatientDocument6 pagesDiagnosis and Evaluation of Eating Disorders in The Pediatric Patientcrisitane TadaNo ratings yet
- The Characteristics, Risks, Effects, and Pathophysiology of Eating Disorders - A Review of Anorexia Nervosa and Bulimia NervosaDocument9 pagesThe Characteristics, Risks, Effects, and Pathophysiology of Eating Disorders - A Review of Anorexia Nervosa and Bulimia NervosaIJRASETPublicationsNo ratings yet
- Cognitive-Behavioral Treatment of Avoidant - Restrictive Food Intake DisorderDocument6 pagesCognitive-Behavioral Treatment of Avoidant - Restrictive Food Intake DisordervvvNo ratings yet
- HHS Public Access: Cognitive-Behavioral Treatment of Avoidant/Restrictive Food Intake DisorderDocument11 pagesHHS Public Access: Cognitive-Behavioral Treatment of Avoidant/Restrictive Food Intake DisorderAhmad Tri Anggara SasmitaNo ratings yet
- Behavioural Eating Disorders: Table 4Document8 pagesBehavioural Eating Disorders: Table 4Lina SantosNo ratings yet
- 2016 Article 110Document11 pages2016 Article 110Ahmad Tri Anggara SasmitaNo ratings yet
- Feeding and Eating Disorders in DSM 5Document3 pagesFeeding and Eating Disorders in DSM 5zoyachaudharycollegeNo ratings yet
- Journal KeperawatanDocument16 pagesJournal KeperawatanAmiLia CandrasariNo ratings yet
- Disorders 1 Running Head: Eating DisordersDocument9 pagesDisorders 1 Running Head: Eating Disordersvgonz1No ratings yet
- Research in Autism Spectrum Disorders: SciencedirectDocument9 pagesResearch in Autism Spectrum Disorders: Sciencedirectcsepulveda10No ratings yet
- DolmanDocument13 pagesDolmanNelson Syah HabibiNo ratings yet
- TreasureDocument21 pagesTreasureAndrea EspinosaNo ratings yet
- Current Approach To Eating DisordersDocument6 pagesCurrent Approach To Eating DisordersaaliiizNo ratings yet
- Jcp0617review StefanacciDocument6 pagesJcp0617review StefanacciIzlam Ing TyazNo ratings yet
- Ating Isorders AND Iabetes: W S F O G C & H E G T WDocument25 pagesAting Isorders AND Iabetes: W S F O G C & H E G T WAnonymous QOCn5dNo ratings yet
- Development of The Pica, ARFID, and Rumination Disorder Interview, A Multi-Informant, Semi-Structured Interview of Feeding Disorders Across The Lifespan: A Pilot Study For Ages 10 - 22Document10 pagesDevelopment of The Pica, ARFID, and Rumination Disorder Interview, A Multi-Informant, Semi-Structured Interview of Feeding Disorders Across The Lifespan: A Pilot Study For Ages 10 - 22LAURA CRISTINA TORRES CATANONo ratings yet
- Building Evidence For The Use of Descriptive Subtypes in Youth With Avoidant Restrictive Food Intake DisorderDocument4 pagesBuilding Evidence For The Use of Descriptive Subtypes in Youth With Avoidant Restrictive Food Intake DisorderValentina Castro MottaNo ratings yet
- Age, Gender, and Women 'S Health and The PatientDocument16 pagesAge, Gender, and Women 'S Health and The Patientmarii de los angelesNo ratings yet
- Article 2013 Plan MealDocument11 pagesArticle 2013 Plan MealpaulacamposorpiNo ratings yet
- Anthroposophical Approach To Cancer Rita Leroi MDDocument26 pagesAnthroposophical Approach To Cancer Rita Leroi MD144bob144No ratings yet
- Parameatal Cyst :A Case ReportDocument3 pagesParameatal Cyst :A Case ReportDr.ankit AnandNo ratings yet
- Milia AriaDocument8 pagesMilia AriaAtsabitFarisNo ratings yet
- LetrozoleDocument3 pagesLetrozoleAlmarie PasaoaNo ratings yet
- Appendix DuplicationDocument3 pagesAppendix DuplicationMario TrejoNo ratings yet
- Nursing Management - Colon CancerDocument7 pagesNursing Management - Colon CancerReese Alessandra GandulfoNo ratings yet
- Case Analysis and Concept MapDocument2 pagesCase Analysis and Concept MapHoney Bitas Orias100% (1)
- Liqui-Prep LBC: Second Generation Liquid-Based CytologyDocument30 pagesLiqui-Prep LBC: Second Generation Liquid-Based Cytologyerick.caballeroNo ratings yet
- Epidemiology (Approaches &methods), Disease Causation and ScreeningDocument37 pagesEpidemiology (Approaches &methods), Disease Causation and ScreeningSyed Arifa AndrabiNo ratings yet
- The Anaesthetic Crisis Manual Is An Excellent Companion The Anaesthetic Crisis Manual Has All Drug Doses ConvenientlyDocument1 pageThe Anaesthetic Crisis Manual Is An Excellent Companion The Anaesthetic Crisis Manual Has All Drug Doses Convenientlyali etikarNo ratings yet
- AV UWorld EOs (Rough Draft) - Data - QID LandscapeDocument139 pagesAV UWorld EOs (Rough Draft) - Data - QID LandscapeFeroz RaZa SoomrOo100% (2)
- Date/time Doctor's Order RationaleDocument2 pagesDate/time Doctor's Order Rationalejames pasionNo ratings yet
- Case Presentation (Exam)Document42 pagesCase Presentation (Exam)JAHNAVI KAYASTHANo ratings yet
- Occupational Therapy Initial EvaluationDocument10 pagesOccupational Therapy Initial EvaluationNerissa BanguiNo ratings yet
- Riltrava Aerosphere Epar Product Information enDocument42 pagesRiltrava Aerosphere Epar Product Information enshihyanghuangNo ratings yet
- Hematologic System Practice QuestionsDocument3 pagesHematologic System Practice QuestionsJoslyn GrossNo ratings yet
- Common Brain MalformationsDocument10 pagesCommon Brain MalformationsradiologyNo ratings yet
- Case StudyDocument19 pagesCase StudySELENA MARIE ROSSNo ratings yet
- Neurosurgery Lecture Notes: Abdul Gofar SastrodiningratDocument14 pagesNeurosurgery Lecture Notes: Abdul Gofar SastrodiningratAnggita Setya LudtianingmaNo ratings yet
- Evidence Based For Failed Back Syndrome: Salim M. Ghazi, MDDocument50 pagesEvidence Based For Failed Back Syndrome: Salim M. Ghazi, MDneareastspineNo ratings yet
- Testing For Tuberculosis (TB) : Tuberculin Skin Test (TST)Document2 pagesTesting For Tuberculosis (TB) : Tuberculin Skin Test (TST)Aluh L DiniNo ratings yet
- Evaluation of Microscopic HematuriaDocument15 pagesEvaluation of Microscopic HematuriaAndi SusiloNo ratings yet
- White LesionsDocument53 pagesWhite Lesionsmmali5853No ratings yet
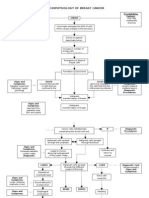
- Pathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsDocument3 pagesPathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsKevin Ercia100% (1)
- Chapter OneDocument7 pagesChapter OneJerome WunujiNo ratings yet
- Infections Dr. Mowafy 2nd EditionDocument26 pagesInfections Dr. Mowafy 2nd EditionMohammed RisqNo ratings yet
- Geriatric Index of Comorbidity: Validation and Comparison With Other Measures of ComorbidityDocument9 pagesGeriatric Index of Comorbidity: Validation and Comparison With Other Measures of ComorbidityDesya EspriliaNo ratings yet
- NP NotesDocument271 pagesNP Notesfataianifowose100% (12)
- Medicolegal DeathDocument13 pagesMedicolegal DeathWASIF ISMAILNo ratings yet
- Urnal Vox Sanguinis - 2023 - Pons - Prevalence of Red Blood Cell Alloantibodies Among Blood Donors in The French Military BloodDocument5 pagesUrnal Vox Sanguinis - 2023 - Pons - Prevalence of Red Blood Cell Alloantibodies Among Blood Donors in The French Military BloodFauzan.ANo ratings yet