You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Ob Gyn Notes - UWorld 2018Document17 pagesOb Gyn Notes - UWorld 2018Fake person0% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Histamine, Serotonin & The Ergot AlkaloidsDocument31 pagesHistamine, Serotonin & The Ergot AlkaloidsnicewanNo ratings yet
- Short Answer Question SurgeryDocument9 pagesShort Answer Question SurgeryJohn M. Hemsworth100% (2)
- Toxicity and Toxicokinetics of Metformin in RatsDocument26 pagesToxicity and Toxicokinetics of Metformin in RatsPooja ReddyNo ratings yet
- Lesson 8&9 Eating Disorders G7Document19 pagesLesson 8&9 Eating Disorders G7ANACORITA O. SILAGANNo ratings yet
- HydronephrosisDocument17 pagesHydronephrosisShradha Khurana100% (2)
- Immunization Handbook For Medical Officers 2017Document346 pagesImmunization Handbook For Medical Officers 2017B. Vineeth ReddyNo ratings yet
- Cordyceps 16mayvjDocument2 pagesCordyceps 16mayvjwarpansy15No ratings yet
- Development of Automatic Temperature Control Brooder System For ChicksDocument73 pagesDevelopment of Automatic Temperature Control Brooder System For ChicksEJ D. ManlangitNo ratings yet
- COVID-19 Vaccines To Prevent SARS-CoV-2 Infection - UpToDateDocument86 pagesCOVID-19 Vaccines To Prevent SARS-CoV-2 Infection - UpToDateXochilt Mejia GarciaNo ratings yet
- Medicine Get Price by DiseaseDocument2 pagesMedicine Get Price by DiseaseYasir ImamNo ratings yet
- Sample Paper - 2Document17 pagesSample Paper - 2sourabhkumarrai7No ratings yet
- Biology The Essentials 3Rd Edition Marielle Hoefnagels Full ChapterDocument67 pagesBiology The Essentials 3Rd Edition Marielle Hoefnagels Full Chaptermilton.alvarado146100% (2)
- Questions and Answers On Describing Adverse Events in The Product Information (Summary of Product Characteristics (SPC) and Package Leaflet (PL) )Document4 pagesQuestions and Answers On Describing Adverse Events in The Product Information (Summary of Product Characteristics (SPC) and Package Leaflet (PL) )Sadgi MehtaNo ratings yet
- Harm Reduction: A British Columbia Community GuideDocument30 pagesHarm Reduction: A British Columbia Community GuideStephen OlsonNo ratings yet
- Essentials of Pharmacology For Health Professions 7th Edition Woodrow Test BankDocument25 pagesEssentials of Pharmacology For Health Professions 7th Edition Woodrow Test BankNormanDanielsyftz100% (54)
- Biological EspionageDocument3 pagesBiological EspionageSasiii SoniiiNo ratings yet
- Defining A High-Performance lCU System For The - , 21st Century: A Position PaperDocument11 pagesDefining A High-Performance lCU System For The - , 21st Century: A Position PaperRodrigoSachiFreitasNo ratings yet
- Basella Alba Extract As Potential Glass CleanerDocument14 pagesBasella Alba Extract As Potential Glass CleanerJandell LagarizaNo ratings yet
- Alamri Ashwaq S2019Document76 pagesAlamri Ashwaq S2019Moonlight 01No ratings yet
- Answers and RationaleDocument6 pagesAnswers and RationaleSheana TmplNo ratings yet
- Sexual Assault Opinion PieceDocument2 pagesSexual Assault Opinion Pieceapi-253813581No ratings yet
- HPV Testing in The Follow-Up of Women Post Colposcopy Treatment - Final VersionDocument16 pagesHPV Testing in The Follow-Up of Women Post Colposcopy Treatment - Final VersionPaulo César López BarrientosNo ratings yet
- 800 Tavill Anatomy-Physiology-Liver PDFDocument29 pages800 Tavill Anatomy-Physiology-Liver PDFSheen AponNo ratings yet
- Acetylcholinesterase InhibitorDocument11 pagesAcetylcholinesterase InhibitorAssassin's j :uNo ratings yet
- E2language Test IDocument11 pagesE2language Test IBünyamin EmerNo ratings yet
- Case Study 1Document9 pagesCase Study 1andry natanel tonyNo ratings yet
- N7 by Novo - Methods of ContraceptionDocument34 pagesN7 by Novo - Methods of ContraceptionEllen Rose NovoNo ratings yet
- HIV Infection and AIDS: Practice EssentialsDocument52 pagesHIV Infection and AIDS: Practice EssentialsRimaNo ratings yet
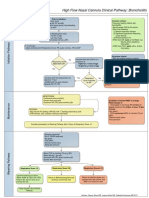
- High Flow Nasal Cannula Clinical Pathway: Bronchiolitis: Prior To Initiation: Inclusion CriteriaDocument1 pageHigh Flow Nasal Cannula Clinical Pathway: Bronchiolitis: Prior To Initiation: Inclusion Criteriad'Agung NugrohoNo ratings yet