You might also like
- Single Subject Design: Group 5Document16 pagesSingle Subject Design: Group 5Zam JonalynNo ratings yet
- Single-Subject ResearchDocument24 pagesSingle-Subject ResearchNaurah NazhifahNo ratings yet
- Single Case Research DesignDocument10 pagesSingle Case Research DesignDashMadNo ratings yet
- Tres PilaresDocument3 pagesTres Pilaresyoyo73No ratings yet
- Repeated Measure DesignDocument8 pagesRepeated Measure Designstudent0990No ratings yet
- Crossover DesignDocument9 pagesCrossover DesignkhadiijahameedNo ratings yet
- ABA TechAssessmentDocument49 pagesABA TechAssessmentRavi Varakala100% (1)
- Single Subject Design SEEDDocument40 pagesSingle Subject Design SEEDMuhammad FaisalNo ratings yet
- Pr2 HandoutDocument6 pagesPr2 HandoutShahanna GarciaNo ratings yet
- Borusyak, Jaravel - 2017 - Revisiting Event Study DesignsDocument25 pagesBorusyak, Jaravel - 2017 - Revisiting Event Study DesignsvladtarkoNo ratings yet
- Basic Principles of Single System DesignDocument7 pagesBasic Principles of Single System DesignVictor OhasNo ratings yet
- Quan GuidelinesDocument11 pagesQuan GuidelinesRusty KuuleNo ratings yet
- Propensity Scores: A Practical Introduction Using RDocument21 pagesPropensity Scores: A Practical Introduction Using RMunirul UlaNo ratings yet
- QuantguideDocument11 pagesQuantguideJorge Lopez FerminNo ratings yet
- Artikel 2 Greenwald, Within Subjects Designs To Use or Not To UseDocument7 pagesArtikel 2 Greenwald, Within Subjects Designs To Use or Not To UseBilqis HumairaNo ratings yet
- ExP Psych-11Document29 pagesExP Psych-11Louise L.No ratings yet
- Single Case Time Series With Bayesian Analysis A Practitioner S GuideDocument13 pagesSingle Case Time Series With Bayesian Analysis A Practitioner S GuideCai PengpengNo ratings yet
- Untitled DocumentDocument4 pagesUntitled DocumentAyesha ZiaNo ratings yet
- Mastering ChainDocument15 pagesMastering ChainMarianela Rossi100% (1)
- Design Type DefinitionsDocument4 pagesDesign Type DefinitionskiranNo ratings yet
- Lecture Notes: Take Note! Characteristics of A Good Experimental DesignDocument5 pagesLecture Notes: Take Note! Characteristics of A Good Experimental Designmarvin jayNo ratings yet
- Textual Notes - Research DesignDocument12 pagesTextual Notes - Research DesignSandesh WaghmareNo ratings yet
- Solved Assignment Ms - 95 Dec 2013Document7 pagesSolved Assignment Ms - 95 Dec 2013Anu K PeterNo ratings yet
- Day 2 Reporting PR 2Document5 pagesDay 2 Reporting PR 2Loujean Gudes MarNo ratings yet
- GugefBM Statsupport 20230912 DesignDocument4 pagesGugefBM Statsupport 20230912 Designtjopza31No ratings yet
- Research DesignDocument11 pagesResearch DesignJarel LakandulaNo ratings yet
- DiD Review PaperDocument54 pagesDiD Review PaperJennyfer Flores CerratoNo ratings yet
- Quasi-Experimental and Single-Case DesignsDocument11 pagesQuasi-Experimental and Single-Case DesignsericantwiNo ratings yet
- Oxford Journal PracticesDocument6 pagesOxford Journal PracticesBruno GrisoliaNo ratings yet
- Design of Experiments & ANOVADocument7 pagesDesign of Experiments & ANOVAvelkus2013No ratings yet
- Applied Behavior Analysis (ABA)Document22 pagesApplied Behavior Analysis (ABA)Ravi Varakala86% (7)
- Article Review BPRDocument6 pagesArticle Review BPRbelay27haileNo ratings yet
- In-Methodology & DesignDocument45 pagesIn-Methodology & Designnica pidlaoanNo ratings yet
- Lecture Notes (Chap 12,1,3)Document6 pagesLecture Notes (Chap 12,1,3)sarasNo ratings yet
- Additional (Required Reading)Document15 pagesAdditional (Required Reading)handeimam39No ratings yet
- Jomo Kenyatta University of Agriculture and TechnologyDocument5 pagesJomo Kenyatta University of Agriculture and TechnologysolocheruicNo ratings yet
- Applied Behavior Analysis: Areas of ApplicationDocument16 pagesApplied Behavior Analysis: Areas of ApplicationFelipe SantosNo ratings yet
- Journal Club 4: Intervention StudiesDocument4 pagesJournal Club 4: Intervention StudiesSpeech & Language Therapy in PracticeNo ratings yet
- LECTURE NOTES On Pretest and PosttestDocument4 pagesLECTURE NOTES On Pretest and Posttestmarvin jayNo ratings yet
- Applied Behaviour AnalysisDocument13 pagesApplied Behaviour Analysisdatta_suNo ratings yet
- Q2 Week 2 Intro To Experimental DesignDocument35 pagesQ2 Week 2 Intro To Experimental Designyakovapura1No ratings yet
- Answer 3Document6 pagesAnswer 3Manjushree RandiveNo ratings yet
- Formulation of The Research Problem & Development of The Research HypothesesDocument29 pagesFormulation of The Research Problem & Development of The Research HypothesesADITYA SHARMA 1927706No ratings yet
- Applied Behavior AnalysisDocument14 pagesApplied Behavior Analysiseduardoflores40100% (2)
- Behavior ModificationDocument8 pagesBehavior ModificationAsifa SultanaNo ratings yet
- #2. The Psychology Professor Has Two Sections of Students That Were Not RandomlyDocument2 pages#2. The Psychology Professor Has Two Sections of Students That Were Not RandomlyShrey MangalNo ratings yet
- Compendium OF Research MethodsDocument9 pagesCompendium OF Research MethodsTarusengaNo ratings yet
- Using The Leapfrog Design As A Simple Form of AdDocument17 pagesUsing The Leapfrog Design As A Simple Form of AdSimonia CoutinhoNo ratings yet
- Research DesignDocument43 pagesResearch DesignUIBS DelhiNo ratings yet
- Research Ii PartDocument62 pagesResearch Ii PartPrecilla C. StephenNo ratings yet
- Pr2 Week 1Document17 pagesPr2 Week 1Julie CabusaoNo ratings yet
- Characteristics of Quantitative ResearchDocument31 pagesCharacteristics of Quantitative ResearchDayhen Afable BianesNo ratings yet
- Checklist 2 Armed RCT Default CapDocument26 pagesChecklist 2 Armed RCT Default CapBaiq DysaNo ratings yet
- The Effectiveness of Intervention On The Behavior of Individuals With AutismDocument21 pagesThe Effectiveness of Intervention On The Behavior of Individuals With AutismrarasNo ratings yet
- Alan E. Kazdin - Research Design in Clinical Psychology-Pearson (2016)Document49 pagesAlan E. Kazdin - Research Design in Clinical Psychology-Pearson (2016)Paula LeónNo ratings yet
- Normative Case StudyDocument4 pagesNormative Case StudySessylu TalaveraNo ratings yet
- Lesson 1 2 Characteristics of Quantitative Research and Importance Across FieldsDocument13 pagesLesson 1 2 Characteristics of Quantitative Research and Importance Across FieldsBAUTISTA, CASHIESCA M.No ratings yet
- Week 1 IiiDocument25 pagesWeek 1 IiiPaul Jean MerinoNo ratings yet
- Experimental Design - Within-Subjects DesignDocument27 pagesExperimental Design - Within-Subjects Designfauzan.abdullahNo ratings yet
- High Spatial-Temporal Resolution MRI Reconstruction For Speech Production AnalysisDocument10 pagesHigh Spatial-Temporal Resolution MRI Reconstruction For Speech Production AnalysisNANDANA MURALINo ratings yet
- Magnetic Resonance Imaging (Mri) : Basics and ApplicationsDocument31 pagesMagnetic Resonance Imaging (Mri) : Basics and ApplicationsNANDANA MURALINo ratings yet
- AssignmentDocument1 pageAssignmentNANDANA MURALINo ratings yet
- HM Case Analysis-1Document3 pagesHM Case Analysis-1NANDANA MURALINo ratings yet
- Receptor Autoradiography: Yajusha RanadiveDocument11 pagesReceptor Autoradiography: Yajusha RanadiveNANDANA MURALINo ratings yet
- A Measure of Finger DixterityDocument4 pagesA Measure of Finger DixterityNANDANA MURALINo ratings yet
- Carbon Coder Format Guide PDFDocument7 pagesCarbon Coder Format Guide PDFPeter Earl FormillezaNo ratings yet
- DSR 200apDocument4 pagesDSR 200apprismadigitallNo ratings yet
- Sony HVR HD1000 V1 PDFDocument410 pagesSony HVR HD1000 V1 PDFHeNeXeNo ratings yet
- TMIcat 2002Document38 pagesTMIcat 2002djokanomcaNo ratings yet
- AG HVX201AE Leaflet 485Document16 pagesAG HVX201AE Leaflet 485Marcelo Rodriguez EscuderoNo ratings yet
- Kodak White Paper 4208Document14 pagesKodak White Paper 4208manuelbascoy1988No ratings yet
- Hvr-Z7u, Hvr-z7j, Hvr-z7n, Hvr-Z7e, Hvr-z7p, Hvr-z7c Service ManualDocument494 pagesHvr-Z7u, Hvr-z7j, Hvr-z7n, Hvr-Z7e, Hvr-z7p, Hvr-z7c Service ManualjemcrookNo ratings yet
- Understanding Omneon Data Stripe, TC and Type of FileDocument28 pagesUnderstanding Omneon Data Stripe, TC and Type of FileRobertNo ratings yet
- Panasonic AG-HPX300Document176 pagesPanasonic AG-HPX300StepanNo ratings yet
- Aja Kona Lhi Manual v10.3Document78 pagesAja Kona Lhi Manual v10.3RizkyNo ratings yet
- 15 Minute Film School by The Hollywood Film InstituteDocument4 pages15 Minute Film School by The Hollywood Film InstituteTony Dushkov100% (1)
- Manual Sony DCR PC105Document240 pagesManual Sony DCR PC105janreNo ratings yet
- Blu-Ray Disc Seminar Report On 2011-2012: Dept of Computer Engineering 10 G.P.T.C.KaduthuruthyDocument27 pagesBlu-Ray Disc Seminar Report On 2011-2012: Dept of Computer Engineering 10 G.P.T.C.Kaduthuruthygosu320No ratings yet
- JVC Mini DV and S-VHS Deck Instruction Sheet: I. Capturing FootageDocument3 pagesJVC Mini DV and S-VHS Deck Instruction Sheet: I. Capturing Footagecabonedu0340No ratings yet
- Manual Id879 - EngDocument96 pagesManual Id879 - EngIdjoskoNo ratings yet
- Nexio Nxamp3801hdx Userguide 175 100244 00 RevaDocument140 pagesNexio Nxamp3801hdx Userguide 175 100244 00 RevasanqcNo ratings yet
- Submersible Semi Vortex Pumps ModelDocument2 pagesSubmersible Semi Vortex Pumps ModelFilipNo ratings yet
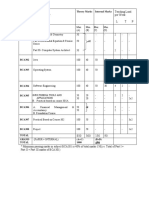
- Teaching Load Per Week L T P: Subject Code Subject Paper Theory Marks Internal MarksDocument14 pagesTeaching Load Per Week L T P: Subject Code Subject Paper Theory Marks Internal MarksAk GuptaNo ratings yet
- Sonar™ 8: (Windows XP, Windows Vista)Document22 pagesSonar™ 8: (Windows XP, Windows Vista)Andhang HabsoroNo ratings yet
- DV Formats - Everything You Need To KnowDocument70 pagesDV Formats - Everything You Need To KnowJelena NikolićNo ratings yet
- Sony DSR450 Operation ManualDocument140 pagesSony DSR450 Operation Manualsonytecho50% (2)
- Sony DSR 45 45p ETDocument305 pagesSony DSR 45 45p ETNanji ChauhanNo ratings yet
- Gr-dvm70 JVC CamcorderDocument112 pagesGr-dvm70 JVC Camcorderjt_scribdNo ratings yet
- Video Camera Video RecorderDocument57 pagesVideo Camera Video RecorderahadwarsiNo ratings yet
- Sony Hdr-fx7 Fx7e Ver-1.4 Level-2 SMDocument125 pagesSony Hdr-fx7 Fx7e Ver-1.4 Level-2 SMDanNo ratings yet
- WWW - Lkff.co - Uk: Call For Submissions For The 8 London Kurdish Film FestivalDocument8 pagesWWW - Lkff.co - Uk: Call For Submissions For The 8 London Kurdish Film Festivalapi-221355036No ratings yet
- Canon Mvx250i Mvx200i e SMDocument259 pagesCanon Mvx250i Mvx200i e SMfranzysNo ratings yet
- Fs-4 HD and Fs-4Pro HD: Focus FS-4 Portable DTE RecordersDocument2 pagesFs-4 HD and Fs-4Pro HD: Focus FS-4 Portable DTE RecordersPedro Camargo VargasNo ratings yet
- Service Manual: HVR-Z5C/Z5E/Z5J/Z5N/Z5P/Z5UDocument458 pagesService Manual: HVR-Z5C/Z5E/Z5J/Z5N/Z5P/Z5Upanasony1No ratings yet
- 1 MediaDeck 7000 IntroductionDocument20 pages1 MediaDeck 7000 IntroductionRobertNo ratings yet