You might also like
- Новый документDocument2 pagesНовый документro1977No ratings yet
- José M. Montiel, Juliana F. Cecato, Daniel Bartholomeu, José Eduardo MartinelliDocument9 pagesJosé M. Montiel, Juliana F. Cecato, Daniel Bartholomeu, José Eduardo Martinellimaria alejandraNo ratings yet
- Mmse, Moca, SPMSQ, SlumpDocument7 pagesMmse, Moca, SPMSQ, Slumpfadila anggrainiNo ratings yet
- Journal of The Neurological SciencesDocument6 pagesJournal of The Neurological SciencesnovialbarNo ratings yet
- Cribado de Deterioro Cognitivo 2018Document22 pagesCribado de Deterioro Cognitivo 2018Lalito Manuel Cabellos AcuñaNo ratings yet
- Cognitive TreatmentDocument12 pagesCognitive TreatmentSaul MorenoNo ratings yet
- Evaluation of Cognitive Impairment in Older AdultsDocument7 pagesEvaluation of Cognitive Impairment in Older AdultsnativaoneNo ratings yet
- Cognitive Assement - Woodford PDFDocument16 pagesCognitive Assement - Woodford PDFAnang MurdiatmokoNo ratings yet
- Clinical Applicability and Cutoff Values For AnDocument9 pagesClinical Applicability and Cutoff Values For AnDayanne SilvaNo ratings yet
- 2020 - Van Dongen - Introducing Multiple Screener - An Unsupervised Digital Screening Tool For Cognitive Deficits in MSDocument6 pages2020 - Van Dongen - Introducing Multiple Screener - An Unsupervised Digital Screening Tool For Cognitive Deficits in MSjesicaNo ratings yet
- Comparing Two Measures of Psychomotor Performance in Patients With HIV: The Coin Rotation Test and The Modified HIV Dementia ScreenDocument3 pagesComparing Two Measures of Psychomotor Performance in Patients With HIV: The Coin Rotation Test and The Modified HIV Dementia ScreenAngélica Montañez RobledoNo ratings yet
- Sweedish Normative DataDocument9 pagesSweedish Normative DataMa. Fe De GuzmanNo ratings yet
- MMSE Cross-Domain Variability Predicts Cognitive Decline in CentenariansDocument5 pagesMMSE Cross-Domain Variability Predicts Cognitive Decline in CentenariansMaimunahNo ratings yet
- Freitas 2013Document7 pagesFreitas 2013Francisco RachinasNo ratings yet
- Mini-Mental State Examination: Avaliação Dos Novos Dados Normativos No Rastreio e Diagnóstico Do Défice CognitivoDocument9 pagesMini-Mental State Examination: Avaliação Dos Novos Dados Normativos No Rastreio e Diagnóstico Do Défice CognitivoAndrade GuiNo ratings yet
- Final R PDocument22 pagesFinal R Pdisha groverNo ratings yet
- Childrens Colour Trail TestDocument5 pagesChildrens Colour Trail Testsreetama chowdhuryNo ratings yet
- tmp250 TMPDocument18 pagestmp250 TMPFrontiersNo ratings yet
- Av Cognitiva Pre OpDocument11 pagesAv Cognitiva Pre OpGeriatra Janaina TrentinNo ratings yet
- The Quick Dementia Rating System (QDRS) PDFDocument11 pagesThe Quick Dementia Rating System (QDRS) PDFnvggNo ratings yet
- A Brief Cognitive Assessment Tool PDFDocument8 pagesA Brief Cognitive Assessment Tool PDFKaram Ali ShahNo ratings yet
- Clock Drawing Test Normative DataDocument13 pagesClock Drawing Test Normative Datafatimaramos31No ratings yet
- MoCA Test Norms and Diagnostic Accuracy for Seniors with Varied Education in BrazilDocument7 pagesMoCA Test Norms and Diagnostic Accuracy for Seniors with Varied Education in BrazilMaria Victoria Ruperti ZimmermannNo ratings yet
- 2009 Oxford TestDocument18 pages2009 Oxford Testyani0707No ratings yet
- VAlidación Neuronorma en EM 2020Document7 pagesVAlidación Neuronorma en EM 2020juanpaNo ratings yet
- Cog Screen StrokeDocument11 pagesCog Screen StrokeMiriam NovoNo ratings yet
- Texto 10-CSDocument9 pagesTexto 10-CSHenrique SalmazoNo ratings yet
- Research Article: Machine Learning For The Preliminary Diagnosis of DementiaDocument10 pagesResearch Article: Machine Learning For The Preliminary Diagnosis of DementiaAyon DattaNo ratings yet
- Artigo Chaves e Izquierdo 1992 Mini MentalDocument5 pagesArtigo Chaves e Izquierdo 1992 Mini Mentals3.neuropsicologiaNo ratings yet
- DownloadDocument7 pagesDownloadCesarNo ratings yet
- General Hospital Psychiatry: Review ArticleDocument10 pagesGeneral Hospital Psychiatry: Review Articlehevi_tarsumNo ratings yet
- 10 1002@gps 3787Document7 pages10 1002@gps 3787Gabriel VelozoNo ratings yet
- Early Alzheimer's Disease Prediction in Machine Learning Setup: Empirical Analysis With Missing Value ComputationDocument8 pagesEarly Alzheimer's Disease Prediction in Machine Learning Setup: Empirical Analysis With Missing Value Computationqurat ul ain annieNo ratings yet
- J Neurol Neurosurg Psychiatry 1998 Royall 588 94Document8 pagesJ Neurol Neurosurg Psychiatry 1998 Royall 588 9454321000No ratings yet
- Fig. 1 Fig. 1Document5 pagesFig. 1 Fig. 1SeanVerMartneyNo ratings yet
- Test-retest Reliability of WCST in SchizophreniaDocument6 pagesTest-retest Reliability of WCST in SchizophreniaDiana ParraNo ratings yet
- Art:10.1186/s12877 015 0103 3 1Document9 pagesArt:10.1186/s12877 015 0103 3 1RajabSaputraNo ratings yet
- Lembar Jawaban Skillab Evidence Based Medicine (Ebm) Nama: Reihan Putri Awaliah NIM: 04011181621037 Kelas: BETA 2016Document22 pagesLembar Jawaban Skillab Evidence Based Medicine (Ebm) Nama: Reihan Putri Awaliah NIM: 04011181621037 Kelas: BETA 2016Reihan Putri AwaliahNo ratings yet
- Brief International Cognitive Assessment For MS (BICAMS) : International Standards For ValidationDocument8 pagesBrief International Cognitive Assessment For MS (BICAMS) : International Standards For ValidationandreapalmapNo ratings yet
- A Web-Based Normative Calculator For The Uniform Data Set (UDS) Neuropsychological Test BatteryDocument9 pagesA Web-Based Normative Calculator For The Uniform Data Set (UDS) Neuropsychological Test BatteryVicente CáceresNo ratings yet
- Moca ReviewDocument4 pagesMoca ReviewLuthfi IndiwirawanNo ratings yet
- A Brief Cognitive Assessment Tool For SchizophreniaDocument8 pagesA Brief Cognitive Assessment Tool For SchizophreniaRatriningdyah DewiNo ratings yet
- Relationship Between The Activities of Daily Living Questionnaire and The Montreal Cognitive AssessmentDocument4 pagesRelationship Between The Activities of Daily Living Questionnaire and The Montreal Cognitive AssessmentCristina SavaNo ratings yet
- Cognitive Distortion QuestionnaireDocument7 pagesCognitive Distortion QuestionnaireagusNo ratings yet
- 2017 - Clinical and Demographic Predictors of Conversion To Dementia in Mexican Elderly With Mild Cognitive ImpairmentDocument7 pages2017 - Clinical and Demographic Predictors of Conversion To Dementia in Mexican Elderly With Mild Cognitive ImpairmentRaúl VerdugoNo ratings yet
- MSE Research 1Document11 pagesMSE Research 1kuro hanabusaNo ratings yet
- Five-Minute Cognitive Test As A New Quick Screening of Cognitive Impairment in The ElderlyDocument12 pagesFive-Minute Cognitive Test As A New Quick Screening of Cognitive Impairment in The ElderlyMaria Jose AdameNo ratings yet
- Новый документDocument2 pagesНовый документro1977No ratings yet
- Clinical Toolkit For Early Dementia Phase: 1. Standardized Mini-Mental Status Examination (MMSE)Document4 pagesClinical Toolkit For Early Dementia Phase: 1. Standardized Mini-Mental Status Examination (MMSE)Carolina MalheiroNo ratings yet
- Test Your Memory Spanish Version TYM SDocument11 pagesTest Your Memory Spanish Version TYM SMariana HernandezNo ratings yet
- Subtle Deficits in Instrumental Activities of Daily Living in Subtypes of Mild Cognitive ImpairmentDocument10 pagesSubtle Deficits in Instrumental Activities of Daily Living in Subtypes of Mild Cognitive ImpairmentAlejandra GutiérrezNo ratings yet
- Explanation of Evaluation Table/Review of The LiteratureDocument14 pagesExplanation of Evaluation Table/Review of The LiteratureTIMOTHY ADUNGANo ratings yet
- Assessing Alzheimer's with cognitive testsDocument14 pagesAssessing Alzheimer's with cognitive testsLanna RegoNo ratings yet
- Towards reporting standards for neuropsychological study resultsDocument8 pagesTowards reporting standards for neuropsychological study resultseup_1983No ratings yet
- REvisión sistemática sobre Bicams 2020Document20 pagesREvisión sistemática sobre Bicams 2020juanpaNo ratings yet
- Paper ACE-R Final 04-1.02.12 Def CMDocument32 pagesPaper ACE-R Final 04-1.02.12 Def CMIngridNo ratings yet
- A Machine Learning Framework Involving EEG Based Functional Connectivity To Diagnose Major Depressive Disorder (MDD)Document14 pagesA Machine Learning Framework Involving EEG Based Functional Connectivity To Diagnose Major Depressive Disorder (MDD)asma khanNo ratings yet
- Tom N. Tombaugh Et Al (1992) The MiniMental State Examination - A Comprehensive ReviewDocument14 pagesTom N. Tombaugh Et Al (1992) The MiniMental State Examination - A Comprehensive ReviewAna AlcántaraNo ratings yet
- Cognitive Discernible Factors Between Schizophrenia and Schizoavective DisorderDocument4 pagesCognitive Discernible Factors Between Schizophrenia and Schizoavective DisorderdarkarotNo ratings yet
- Psychophysiological assessment of human cognition and its enhancement by a non-invasive methodFrom EverandPsychophysiological assessment of human cognition and its enhancement by a non-invasive methodNo ratings yet
- Cognitiv Si Insf CardiacaDocument20 pagesCognitiv Si Insf CardiacaAlexandru MartNo ratings yet
- Cognitive Decline in Heart Failure: More Attention Is NeededDocument4 pagesCognitive Decline in Heart Failure: More Attention Is NeededAlexandru MartNo ratings yet
- European J of Heart Fail - 2017 - Gorter - Right Heart Dysfunction and Failure in Heart Failure With Preserved EjectionDocument22 pagesEuropean J of Heart Fail - 2017 - Gorter - Right Heart Dysfunction and Failure in Heart Failure With Preserved EjectionAlexandru MartNo ratings yet
- EasyOneAir Operators Manual V01 ENDocument143 pagesEasyOneAir Operators Manual V01 ENAlexandru MartNo ratings yet
- Esc Beta Blocker Expert ConsensusDocument1 pageEsc Beta Blocker Expert ConsensusAkhmad HidayatNo ratings yet
- 2015 ChamberQuantificationREVDocument53 pages2015 ChamberQuantificationREVViktor GorbatykhNo ratings yet
- Cognitive Deficits in Healthy ElderlyDocument7 pagesCognitive Deficits in Healthy ElderlyAlexandru MartNo ratings yet
- LARESHA LILAVATIE - 0517140087 - Nilai Prognostik Pengulangan Resonansi Magnetik Jantung Di Indonesia Penderita Miokarditis AkutDocument10 pagesLARESHA LILAVATIE - 0517140087 - Nilai Prognostik Pengulangan Resonansi Magnetik Jantung Di Indonesia Penderita Miokarditis AkutLaresha LilavatieNo ratings yet
- Quantitative and Qualitative Analyses of Clock Drawings in Alzheimer's and Huntington's DiseaseDocument18 pagesQuantitative and Qualitative Analyses of Clock Drawings in Alzheimer's and Huntington's DiseaseAlexandru MartNo ratings yet
- A Meta-Analysis of The Accuracy of The Mini-Mental State Examination PDFDocument21 pagesA Meta-Analysis of The Accuracy of The Mini-Mental State Examination PDFAlexandru MartNo ratings yet
- Referat Medical Anexa2Document1 pageReferat Medical Anexa2Alexandru MartNo ratings yet
- 3-Women Athletes Knee Injuries - 2005Document9 pages3-Women Athletes Knee Injuries - 2005Fernanda CarvalhoNo ratings yet
- Child Abuse Research JournalDocument9 pagesChild Abuse Research JournaladrianekattnerNo ratings yet
- Unilag MSC Environmenatl Toxicology SampleDocument4 pagesUnilag MSC Environmenatl Toxicology SamplebdianNo ratings yet
- Thomas Foot ReflexologyDocument112 pagesThomas Foot ReflexologySa MiNo ratings yet
- Ecg 01Document103 pagesEcg 01Bandar al ghamdi100% (1)
- City of Peterborough 2023 Draft Capital BudgetDocument535 pagesCity of Peterborough 2023 Draft Capital BudgetPeterborough ExaminerNo ratings yet
- 2020 Lamberti RCT Effectiveness of RBFT Slow Walking On Mobility in Severe Multiple SclerosisDocument11 pages2020 Lamberti RCT Effectiveness of RBFT Slow Walking On Mobility in Severe Multiple SclerosisArmin ParavlićNo ratings yet
- OBG ChapterDocument3 pagesOBG ChapterMohd IrfanNo ratings yet
- Live deer placenta stem cells not found in food supplement capsulesDocument1 pageLive deer placenta stem cells not found in food supplement capsulesJohn LêNo ratings yet
- 9 Types of Female Orgasms ExplainedDocument4 pages9 Types of Female Orgasms ExplainedAbdul SyukurNo ratings yet
- Anna Fagin Resume Aug 2014Document1 pageAnna Fagin Resume Aug 2014api-261821160No ratings yet
- PIL For Sudafed DecongestantDocument2 pagesPIL For Sudafed DecongestantOdunlamiNo ratings yet
- Human Resources Manager in San Jose CA Resume Priscilla CramerDocument2 pagesHuman Resources Manager in San Jose CA Resume Priscilla CramerPriscillaCramerNo ratings yet
- Anatomia SufletuluiDocument1 pageAnatomia SufletuluiAlexandrina DeaşNo ratings yet
- Berklee Intro Music Therapy PDFDocument17 pagesBerklee Intro Music Therapy PDFTheodore VaillantNo ratings yet
- Nurs 5019 - Soap Note 41-60 Year OldDocument7 pagesNurs 5019 - Soap Note 41-60 Year Oldapi-308904543100% (1)
- Penile Injection TherapyDocument4 pagesPenile Injection Therapydr NayanBharadwajNo ratings yet
- Prevalence of GERD in Dyspepsia PatientsDocument6 pagesPrevalence of GERD in Dyspepsia PatientsAbrar TaraNo ratings yet
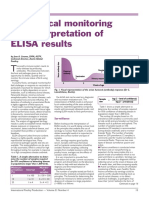
- Serological Monitoring by ELISADocument3 pagesSerological Monitoring by ELISAreza tavayef100% (1)
- Laparoscopic Management of Giant Ovarian Cyst A Case ReportDocument3 pagesLaparoscopic Management of Giant Ovarian Cyst A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Pothole Claim Form in PhiladelphiaDocument3 pagesPothole Claim Form in Philadelphiaphilly victorNo ratings yet
- High Birth Rate Is A Special Feature of All The Developing EconomiesDocument3 pagesHigh Birth Rate Is A Special Feature of All The Developing EconomiesMuhammad SohaibNo ratings yet
- Narrative ReportDocument23 pagesNarrative ReportErnest Gerard Baiño Durano100% (2)
- DMLC Part I & II Cyprus (Hyundai Busan)Document17 pagesDMLC Part I & II Cyprus (Hyundai Busan)Shankar Singh0% (1)
- SpitzDocument30 pagesSpitzprabhatNo ratings yet
- Hygiene Rules For Hotel Kitchen and Food Production StaffDocument3 pagesHygiene Rules For Hotel Kitchen and Food Production Staffvishnu nairNo ratings yet
- Mercury in The MistDocument2 pagesMercury in The MistAnand BhagwaniNo ratings yet
- Travel Guide to Thailand in 2021Document14 pagesTravel Guide to Thailand in 2021Russell KhanNo ratings yet
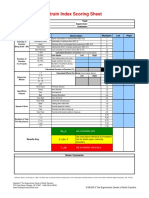
- Strain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorDocument1 pageStrain Index Scoring Sheet: Date: Task: Company: Supervisor: Dept: EvaluatorUdaydeep SinghNo ratings yet
- 210 419 1 SMDocument4 pages210 419 1 SMIneMeilaniNo ratings yet