You might also like
- Computing Model For Alzheimer Prediction Using Support Vector Machine ClassifierDocument10 pagesComputing Model For Alzheimer Prediction Using Support Vector Machine ClassifierKishore Kanna Ravi KumarNo ratings yet
- Jad - 2020 - 75 1 - Jad 75 1 Jad191169 - Jad 75 Jad191169Document12 pagesJad - 2020 - 75 1 - Jad 75 1 Jad191169 - Jad 75 Jad191169Ayon DattaNo ratings yet
- A Web-Based Normative Calculator For The Uniform Data Set (UDS) Neuropsychological Test BatteryDocument9 pagesA Web-Based Normative Calculator For The Uniform Data Set (UDS) Neuropsychological Test BatteryVicente CáceresNo ratings yet
- Abnormal MoCA and Normal Range MMSE Scores in Parkinson D Without DementiaDocument15 pagesAbnormal MoCA and Normal Range MMSE Scores in Parkinson D Without DementiadquebradasNo ratings yet
- A Deep Feature-Based Real-Time System For Alzheimer Disease Stage DetectionDocument19 pagesA Deep Feature-Based Real-Time System For Alzheimer Disease Stage Detectionmozhganeutoop1998No ratings yet
- Paper 218061Document14 pagesPaper 218061laura EstaloteNo ratings yet
- Paper 07Document15 pagesPaper 07Electro ElkoranyNo ratings yet
- Brain Sciences: A Deep Siamese Convolution Neural Network For Multi-Class Classification of Alzheimer DiseaseDocument15 pagesBrain Sciences: A Deep Siamese Convolution Neural Network For Multi-Class Classification of Alzheimer DiseaseVictorvikkNo ratings yet
- Optimized_Transfer_Learning_Based_Dementia_Prediction_System_for_Rehabilitation_Therapy_PlanningDocument13 pagesOptimized_Transfer_Learning_Based_Dementia_Prediction_System_for_Rehabilitation_Therapy_Planningxavierknight817No ratings yet
- Classification of Adult Autistic Spectrum Disorder Using Machine Learning ApproachDocument9 pagesClassification of Adult Autistic Spectrum Disorder Using Machine Learning ApproachIAES IJAINo ratings yet
- Predicting Alzheimer's Disease Progression Using Multi-Modal Deep Learning ApproachDocument12 pagesPredicting Alzheimer's Disease Progression Using Multi-Modal Deep Learning ApproachMayssa SOUSSIANo ratings yet
- Machine Learning Classification of MRI Features of AlzheimerDocument4 pagesMachine Learning Classification of MRI Features of AlzheimerReshma KhemchandaniNo ratings yet
- ML 2020Document18 pagesML 2020Bhaskar Rao PNo ratings yet
- A New Weakly Supervised Deep Neural Network For Recognizing Alzheimer's DiseaseDocument12 pagesA New Weakly Supervised Deep Neural Network For Recognizing Alzheimer's DiseasepelodepuyaNo ratings yet
- Alzheimers Disease Detection Using Different Machine Learning AlgorithmsDocument7 pagesAlzheimers Disease Detection Using Different Machine Learning AlgorithmsIJRASETPublications100% (1)
- Predicting Alzheimer's Disease Progression Using Multi-Modal Deep Learning ApproachDocument12 pagesPredicting Alzheimer's Disease Progression Using Multi-Modal Deep Learning ApproachManoj MaggotNo ratings yet
- Research Article: Machine Learning For The Preliminary Diagnosis of DementiaDocument10 pagesResearch Article: Machine Learning For The Preliminary Diagnosis of DementiaAyon DattaNo ratings yet
- j.trsl.2018.01.001Document34 pagesj.trsl.2018.01.001k6fqcwfczfNo ratings yet
- Av Cognitiva Pre OpDocument11 pagesAv Cognitiva Pre OpGeriatra Janaina TrentinNo ratings yet
- Specific Algorithm Method of Scoring The Clock Drawing Test Applied in Cognitively Normal ElderlyDocument8 pagesSpecific Algorithm Method of Scoring The Clock Drawing Test Applied in Cognitively Normal ElderlyAlexandru MartNo ratings yet
- (IJCST-V10I5P50) :DR K. Sailaja, Guttalasandu Vasudeva ReddyDocument7 pages(IJCST-V10I5P50) :DR K. Sailaja, Guttalasandu Vasudeva ReddyEighthSenseGroupNo ratings yet
- Prediction of Heart Diseases Using Machine LearningDocument49 pagesPrediction of Heart Diseases Using Machine Learningandyy4663No ratings yet
- Author NoteDocument58 pagesAuthor Noteedmilson júniorNo ratings yet
- Mmse, Moca, SPMSQ, SlumpDocument7 pagesMmse, Moca, SPMSQ, Slumpfadila anggrainiNo ratings yet
- Heart Disease Prediction Using MLDocument8 pagesHeart Disease Prediction Using MLAppleNo ratings yet
- AlzheimerDocument3 pagesAlzheimersoumya salianNo ratings yet
- Survival Study On Medical Disease Diagnosis With Coronavirus DatabaseDocument9 pagesSurvival Study On Medical Disease Diagnosis With Coronavirus DatabaseIJRASETPublicationsNo ratings yet
- A Machine Learning Framework Involving EEG Based Functional Connectivity To Diagnose Major Depressive Disorder (MDD)Document14 pagesA Machine Learning Framework Involving EEG Based Functional Connectivity To Diagnose Major Depressive Disorder (MDD)asma khanNo ratings yet
- 4958-Article Text-9220-1-10-20210503Document11 pages4958-Article Text-9220-1-10-20210503Abdunabi MuhamadievNo ratings yet
- Literature SurveyDocument4 pagesLiterature Surveyravikumar89386No ratings yet
- CKD Stage Prediction and Suitable Diet Recommendation A SurveyDocument6 pagesCKD Stage Prediction and Suitable Diet Recommendation A SurveyIJRASETPublicationsNo ratings yet
- E23MTCG0003 ShivenShiwachDocument50 pagesE23MTCG0003 ShivenShiwachSHAILJA TRIPATHI 097No ratings yet
- V5i9 0240Document4 pagesV5i9 0240Nogo LumutenNo ratings yet
- Machine Learning in Alzheimer’s DiseaseDocument17 pagesMachine Learning in Alzheimer’s DiseaseBella ChenNo ratings yet
- Predicting Cardiovascular Disease Using Hybrid MLDocument9 pagesPredicting Cardiovascular Disease Using Hybrid MLewuiplkw phuvdjNo ratings yet
- Efficient Binary Classifier For Prediction of Diabetes Using Data Preprocessing and Support Vector MachineDocument2 pagesEfficient Binary Classifier For Prediction of Diabetes Using Data Preprocessing and Support Vector MachineParvinder McCartneyNo ratings yet
- A Machine Learning Methodology For Diagnosing Chronic Kidney DiseaseDocument2 pagesA Machine Learning Methodology For Diagnosing Chronic Kidney DiseaseWebsoft Tech-HydNo ratings yet
- Alzheimer's Disease Classification Using Feed Forwarded Deep Neural Networks For Brain MRI ImagesDocument15 pagesAlzheimer's Disease Classification Using Feed Forwarded Deep Neural Networks For Brain MRI ImagesWided HechkelNo ratings yet
- IEEE Conference TemplateDocument4 pagesIEEE Conference TemplatepriyalNo ratings yet
- Machine Learning Techniques For Heart Disease PredictionDocument8 pagesMachine Learning Techniques For Heart Disease PredictionRicky ThanmaiNo ratings yet
- alzh_JAD_final2Document18 pagesalzh_JAD_final2psychometrie.copeNo ratings yet
- Machine Learning Prediction of Coronary Heart DiseaseDocument6 pagesMachine Learning Prediction of Coronary Heart DiseaseNowreen HaqueNo ratings yet
- Corrected SynopsisDocument8 pagesCorrected SynopsisVenkatKanthNo ratings yet
- Diagnostic Support For Alzheimers Disease Through Feature-Based Brain MRI Retrieval and Unsupervised Distance LearningDocument8 pagesDiagnostic Support For Alzheimers Disease Through Feature-Based Brain MRI Retrieval and Unsupervised Distance Learning1NT20CS076 KAMSALA THARUNNo ratings yet
- Disease Prediction Using Machine Learning Algorithms KNN and CNNDocument7 pagesDisease Prediction Using Machine Learning Algorithms KNN and CNNIJRASETPublications100% (1)
- Ieeeicassp PD 1.2.1Document5 pagesIeeeicassp PD 1.2.1Vyom RavalNo ratings yet
- Machine Learning For Comprehensive Forecasting of Alzheimer's Disease ProgressionDocument14 pagesMachine Learning For Comprehensive Forecasting of Alzheimer's Disease Progressionth8yvv4gpmNo ratings yet
- Relationship Between The Activities of Daily Living Questionnaire and The Montreal Cognitive AssessmentDocument4 pagesRelationship Between The Activities of Daily Living Questionnaire and The Montreal Cognitive AssessmentCristina SavaNo ratings yet
- Early Cognitive Changes and Predictive Models: A Multilayer Perceptron With Neuropsychological Test DataDocument8 pagesEarly Cognitive Changes and Predictive Models: A Multilayer Perceptron With Neuropsychological Test DataInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Multiple Disease Prediction System Using Machine LearningDocument5 pagesMultiple Disease Prediction System Using Machine Learningsamashbal7No ratings yet
- Machine Learning Solutions Applied To Amyotrophic Lateral Sclerosis Prognosis: A ReviewDocument12 pagesMachine Learning Solutions Applied To Amyotrophic Lateral Sclerosis Prognosis: A ReviewJoel ArraisNo ratings yet
- A Detection and Segmentation of Medical Image Using Machine Learning AlgorithmsDocument5 pagesA Detection and Segmentation of Medical Image Using Machine Learning AlgorithmsNazmul HassanNo ratings yet
- CNN Technique For Detecting Alzheimer's Disease by Using MRI ImagesDocument13 pagesCNN Technique For Detecting Alzheimer's Disease by Using MRI Imagesali hamdiNo ratings yet
- Evaluation of Cognitive Impairment in Older AdultsDocument7 pagesEvaluation of Cognitive Impairment in Older AdultsnativaoneNo ratings yet
- A Machine Learning Perspective: Prediction of Chronic Kidney DiseaseDocument22 pagesA Machine Learning Perspective: Prediction of Chronic Kidney DiseaseSadiNo ratings yet
- 2nd Review ReportDocument6 pages2nd Review ReportHarshNo ratings yet
- Machine Learning Classification for Diabetes DetectionDocument6 pagesMachine Learning Classification for Diabetes DetectionHoàng NamNo ratings yet
- Early Detection of Parkinson's Disease Through Patient Questionnaire and Predictive ModellingDocument42 pagesEarly Detection of Parkinson's Disease Through Patient Questionnaire and Predictive ModellingKanagaraj SubramaniNo ratings yet
- Mental Health Detection Using Machine LearningDocument31 pagesMental Health Detection Using Machine LearninggvarshithavarshiNo ratings yet
- Data Science Project Ideas, Methodology & Python Codes in Health CareFrom EverandData Science Project Ideas, Methodology & Python Codes in Health CareNo ratings yet
- The-New-Educational-Imperative - Improving CS EducationDocument90 pagesThe-New-Educational-Imperative - Improving CS Educationqurat ul ain annieNo ratings yet
- Programming in SML Harper CMU 2011Document298 pagesProgramming in SML Harper CMU 2011qurat ul ain annieNo ratings yet
- Beowulf ClusterDocument528 pagesBeowulf ClusterPaulo CaldeiraNo ratings yet
- Bajang Amad by Col. Muhammad KhanDocument111 pagesBajang Amad by Col. Muhammad Khanroadsign100% (3)
- Standardizing In-Car Sensors with TinyOSDocument8 pagesStandardizing In-Car Sensors with TinyOSqurat ul ain annieNo ratings yet
- Logical Approach To Home AutomationDocument4 pagesLogical Approach To Home Automationqurat ul ain annieNo ratings yet
- Hybrid Fuzzy-Statistical Model for Learning Analytics PredictionDocument6 pagesHybrid Fuzzy-Statistical Model for Learning Analytics Predictionqurat ul ain annieNo ratings yet
- Controlling Real World Pervasive Environments With Knowledge BasesDocument10 pagesControlling Real World Pervasive Environments With Knowledge Basesk1988No ratings yet
- Student Performance Prediction Using Supervised LearningDocument13 pagesStudent Performance Prediction Using Supervised LearningAnjana SNo ratings yet
- Monthly Magzine JAN 2023Document165 pagesMonthly Magzine JAN 2023charan100% (1)
- Plato - The RepublicDocument4 pagesPlato - The Republicanon_709158140No ratings yet
- Elements of Arts Lesson PlanDocument9 pagesElements of Arts Lesson PlanMicahCastro100% (3)
- LPS Training - 2015 Update FINALDocument65 pagesLPS Training - 2015 Update FINALAsriSaffuan86% (7)
- Pmi ThesisDocument4 pagesPmi Thesisgj9vq5z0100% (2)
- Lesson PlanDocument1 pageLesson Planapi-551142254No ratings yet
- Effects of Kahramanmaras Earthquakes in South of Turkey On Livestock ActivitiesDocument10 pagesEffects of Kahramanmaras Earthquakes in South of Turkey On Livestock ActivitiesIJAR JOURNALNo ratings yet
- Water Budget Equation Exercise Problems SolvedDocument10 pagesWater Budget Equation Exercise Problems SolvedSheeraz AhmedNo ratings yet
- 4.sisgp Eligible Master Programmes 2024 2025-UaDocument74 pages4.sisgp Eligible Master Programmes 2024 2025-UaRuddro IslamNo ratings yet
- Chi-Square Test of IndependenceDocument15 pagesChi-Square Test of IndependenceGaming AccountNo ratings yet
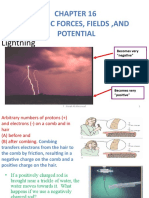
- Electric Forces, Fields, and Potential: LightningDocument164 pagesElectric Forces, Fields, and Potential: LightningIsmail Medhat SalahNo ratings yet
- C1990-EH(HC)ver 1 0英文Document6 pagesC1990-EH(HC)ver 1 0英文顏健軒No ratings yet
- Metaphors in Kapampangan: Mike Pangilinan and Hiroaki KitanoDocument7 pagesMetaphors in Kapampangan: Mike Pangilinan and Hiroaki KitanoThe DigilakansNo ratings yet
- Ceramage: Light-Curing Microhybrid CompositeDocument3 pagesCeramage: Light-Curing Microhybrid CompositeVero GrambergNo ratings yet
- ASTM E1845 - Standard Practice For Calculating Pavement Macrotexture Mean Profile Depth PDFDocument4 pagesASTM E1845 - Standard Practice For Calculating Pavement Macrotexture Mean Profile Depth PDFrendy100% (1)
- Syllabus CoperativeDocument22 pagesSyllabus CoperativeSiva LingamNo ratings yet
- Syllabus of Eeb162Document2 pagesSyllabus of Eeb162Dr. Tirupathiraju KanumuriNo ratings yet
- Winmena - DPGDocument1 pageWinmena - DPGFAIYAZ AHMEDNo ratings yet
- Energy and Entropy (Alekseev, G. N.) (1986) (208p)Document208 pagesEnergy and Entropy (Alekseev, G. N.) (1986) (208p)Lucas Kiel100% (2)
- Competitive Club Soccer: Parents' Assessments of Children's Early and Later Sport Specialization - PDocument12 pagesCompetitive Club Soccer: Parents' Assessments of Children's Early and Later Sport Specialization - PAodhan Jane MooneyNo ratings yet
- SWOT Analysis PaperDocument10 pagesSWOT Analysis Paperrushilmanchanda07No ratings yet
- Modelling and simulating patient pathways at a Moroccan mother-child hospitalDocument7 pagesModelling and simulating patient pathways at a Moroccan mother-child hospitalashlyduartNo ratings yet
- BEMEF - Implementation and M&E PlansDocument2 pagesBEMEF - Implementation and M&E PlansCarmelito C. BongcawelNo ratings yet
- Mathematics 11 00820Document38 pagesMathematics 11 00820Endorsement PECNo ratings yet
- Mesozoic Rock Formations of the South-West Rusca Montana BasinDocument27 pagesMesozoic Rock Formations of the South-West Rusca Montana BasinplanessNo ratings yet
- Work EthicDocument57 pagesWork EthicRambo FranciscoNo ratings yet
- UPP PE Tank Sump Installation GuideDocument32 pagesUPP PE Tank Sump Installation GuidelowiyaunNo ratings yet
- Interpersonal Communication Self Reflection #1Document5 pagesInterpersonal Communication Self Reflection #1monicawoods705No ratings yet
- Jadual Waktu SPM 2010Document2 pagesJadual Waktu SPM 2010sallehGNo ratings yet
- I've Got To Be MeDocument35 pagesI've Got To Be MeRosejen MangubatNo ratings yet