You might also like
- BIO DATA Form Filling Sheet On Arrival Day at ISSBDocument2 pagesBIO DATA Form Filling Sheet On Arrival Day at ISSBAsif Ali Ali64% (22)
- Test Bank For Introduction To Maternity and Pediatric Nursing 8th Edition by LeiferDocument36 pagesTest Bank For Introduction To Maternity and Pediatric Nursing 8th Edition by Leiferpatnesspertain.e2nd2o100% (45)
- Registration Form: Ministry of Primary and Secondary EducationDocument2 pagesRegistration Form: Ministry of Primary and Secondary EducationSigncraft & PrintNo ratings yet
- Standard Gastrointestinal Disease Questionnaire: in ConfidenceDocument8 pagesStandard Gastrointestinal Disease Questionnaire: in ConfidenceAni IoanaNo ratings yet
- Food Handlers Medical FormDocument1 pageFood Handlers Medical FormAnnu Rajesh100% (2)
- Questionnaire For Parents in KindergartenDocument5 pagesQuestionnaire For Parents in KindergartenDobos DóraNo ratings yet
- Medical ReportDocument5 pagesMedical ReportXYZNo ratings yet
- Sociological and Environmental Study of The Community Katukurunda 2Document2 pagesSociological and Environmental Study of The Community Katukurunda 2tharinduanjana323No ratings yet
- Circular No 001 2017 LWDocument31 pagesCircular No 001 2017 LWKenny Wong100% (1)
- AutoRecovery Save of Revised MEDICAL EXAMINATION REPORTDocument3 pagesAutoRecovery Save of Revised MEDICAL EXAMINATION REPORTFred mungaNo ratings yet
- Application For Employment Form ExternalDocument3 pagesApplication For Employment Form ExternalhamzstadiumNo ratings yet
- Confidential: Medical History and Personal Particulars of Students Joining at IIT MadrasDocument4 pagesConfidential: Medical History and Personal Particulars of Students Joining at IIT MadrasNehaNo ratings yet
- Obstetric & Gynecology Departement Medical School / General Hospital FK UKIDocument7 pagesObstetric & Gynecology Departement Medical School / General Hospital FK UKIImanuel CristiantoNo ratings yet
- Winter Weekend 08 PermDocument1 pageWinter Weekend 08 Permhellobeefchief3952No ratings yet
- Sekolah Tinggi Ilmu Kesehatan: Bina Usada BaliDocument16 pagesSekolah Tinggi Ilmu Kesehatan: Bina Usada Balihery gusmayanaNo ratings yet
- Nursery Application Form - Docx 2Document10 pagesNursery Application Form - Docx 2Hamza YasinNo ratings yet
- Conversion DisorderDocument2 pagesConversion DisorderSyeda Dua TanveerNo ratings yet
- COVID-19 Athlete Information FormDocument1 pageCOVID-19 Athlete Information FormGianluigi BuffonNo ratings yet
- Fill in The Admission Card Below! Admission Card: Past Medical and Surgical History Completed byDocument2 pagesFill in The Admission Card Below! Admission Card: Past Medical and Surgical History Completed byIntan Nur SholikahNo ratings yet
- Centenary Bank Head Office Application For Employment Form: Confidential - ExternalDocument3 pagesCentenary Bank Head Office Application For Employment Form: Confidential - ExternalTom SesenteNo ratings yet
- RM 3 Ugd Assesment Medis UgdDocument4 pagesRM 3 Ugd Assesment Medis UgdHajrah SaidNo ratings yet
- Winter PermissionDocument1 pageWinter Permissionhellobeefchief3952No ratings yet
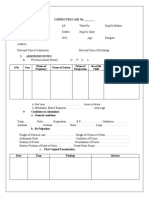
- S.No Year Nature of Pregnancy Nature of Labour Nature of Puerperium Sex of The Child RemarksDocument4 pagesS.No Year Nature of Pregnancy Nature of Labour Nature of Puerperium Sex of The Child RemarksRajaNo ratings yet
- Child Admission FormDocument6 pagesChild Admission FormA.N.M. neyaz MorshedNo ratings yet
- Blood Donation Application FormDocument2 pagesBlood Donation Application FormFadjar MulyaNo ratings yet
- Fitness FormDocument2 pagesFitness FormkaramatNo ratings yet
- Assessment Form UnairDocument6 pagesAssessment Form UnairAkiel Shinobe SlopengNo ratings yet
- Zambia PHF Exit Interview QuestionnaireDocument37 pagesZambia PHF Exit Interview QuestionnairenomdeplumNo ratings yet
- 3.medical FormDocument5 pages3.medical Formamistudio30No ratings yet
- PBC Boys Medical FormDocument4 pagesPBC Boys Medical FormJahred DominiqueNo ratings yet
- Pelvic Pain Patient Initial QuestionnaireDocument6 pagesPelvic Pain Patient Initial QuestionnaireVaralakshmi UppuNo ratings yet
- Mental-Status-exam Modified CleanDocument8 pagesMental-Status-exam Modified Cleanrana05853No ratings yet
- Application For Enrolment: Form No. - 1 National Cadet Corps Senior Division/ Wing Enrolment Form (See Rule 7 and 11)Document4 pagesApplication For Enrolment: Form No. - 1 National Cadet Corps Senior Division/ Wing Enrolment Form (See Rule 7 and 11)Sean May0% (1)
- Format For Inpection of Juvenile JusDocument4 pagesFormat For Inpection of Juvenile Jusvijay kantNo ratings yet
- Travel Questionnaire For PatientsDocument2 pagesTravel Questionnaire For PatientsVineet ShettyNo ratings yet
- Guyana Police ForceDocument16 pagesGuyana Police Forcemorrislinden481No ratings yet
- Supreme Court of India Self Declaration Form (For Entrants in The High Security Zone)Document1 pageSupreme Court of India Self Declaration Form (For Entrants in The High Security Zone)manojsh8887No ratings yet
- Phụ lục 2: (Ký, ghi rõ họ tên)Document3 pagesPhụ lục 2: (Ký, ghi rõ họ tên)Pham Huong LinhNo ratings yet
- Application For Employment: Politicsround PublicationsDocument4 pagesApplication For Employment: Politicsround PublicationsMariah A. BaigNo ratings yet
- Protocol BluebookDocument16 pagesProtocol BluebookItz D LifeNo ratings yet
- Medical CertificateDocument4 pagesMedical CertificateRishi ScifreakNo ratings yet
- Proposal (Editable)Document3 pagesProposal (Editable)Isanka WijerathneNo ratings yet
- Form of Claim For Senior Citizens' PensionDocument4 pagesForm of Claim For Senior Citizens' PensionAnthony BasantaNo ratings yet
- A2 - Remand Interview Sheet - Mar17Document2 pagesA2 - Remand Interview Sheet - Mar17Luqman HakeemNo ratings yet
- Acceptance of Offer of AppointmentDocument11 pagesAcceptance of Offer of AppointmentAditya ShrivastavaNo ratings yet
- Catergory 1 QuestionnaireDocument9 pagesCatergory 1 QuestionnaireShahroz AnsarNo ratings yet
- Mortuary Handover FormDocument1 pageMortuary Handover Formseminar bimckutaNo ratings yet
- To Be Completed by The Applicant: Coronavirus (Sars-Cov-2) Infection QuestionnaireDocument2 pagesTo Be Completed by The Applicant: Coronavirus (Sars-Cov-2) Infection Questionnairecky7vyfv48No ratings yet
- Standard Form of Application: A. Height: B. Colour of EyesDocument2 pagesStandard Form of Application: A. Height: B. Colour of EyesAditya YeoleNo ratings yet
- Fitness FormDocument2 pagesFitness FormnimmilabNo ratings yet
- AAU Medical FitnessDocument1 pageAAU Medical FitnessAnup TalukdarNo ratings yet
- Nursing History: Appendix - Nursing Process Formed CreatedDocument15 pagesNursing History: Appendix - Nursing Process Formed CreatedYuda AjiNo ratings yet
- RM 3 Ugd Assesment Medis UgdDocument3 pagesRM 3 Ugd Assesment Medis UgdHajrah SaidNo ratings yet
- Pasport Form DDNI06330312GO0330Document0 pagesPasport Form DDNI06330312GO0330Awdhesh Singh BhadoriyaNo ratings yet
- Beri Lingkaran Dan Isi Pada Tempat Yang Sesuai: Keterangan Kematian Perinatal-Neonatal Di Fasilitas KesehtanDocument4 pagesBeri Lingkaran Dan Isi Pada Tempat Yang Sesuai: Keterangan Kematian Perinatal-Neonatal Di Fasilitas KesehtanLusye AmaliaNo ratings yet
- 4 5987888106655714130Document16 pages4 5987888106655714130Dr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Keterangan Sebab Kematian: Rs. Surya Asih PringsewuDocument1 pageKeterangan Sebab Kematian: Rs. Surya Asih PringsewuAtika Eka RachmayatiNo ratings yet
- Health Fitness Certificate For The Purposes of Permission To Work in Confined SpaceDocument6 pagesHealth Fitness Certificate For The Purposes of Permission To Work in Confined SpaceNur ShaNo ratings yet
- Proforma For MCCD CertificateDocument1 pageProforma For MCCD CertificateEXAM INFONo ratings yet
- Physical Fitness CertificateDocument1 pagePhysical Fitness CertificateDilip SenthNo ratings yet
- Final Departure: EMBRACING YOUR FAREWELL: A GUIDE TO LEAVING A LASTING LEGACYFrom EverandFinal Departure: EMBRACING YOUR FAREWELL: A GUIDE TO LEAVING A LASTING LEGACYNo ratings yet
- Form VisaDocument2 pagesForm VisaSigncraft & PrintNo ratings yet
- Application For Police Certificate: BirthDocument3 pagesApplication For Police Certificate: BirthSigncraft & PrintNo ratings yet
- Gateway High School Enrolment FormDocument4 pagesGateway High School Enrolment FormSigncraft & PrintNo ratings yet
- Improving Hospital Performance and Productivity With The Balanced Scorecard - 2Document22 pagesImproving Hospital Performance and Productivity With The Balanced Scorecard - 2Yunita Soraya HusinNo ratings yet
- Master of Science in Pharmaceutical MedicineDocument7 pagesMaster of Science in Pharmaceutical MedicineGcwalaNo ratings yet
- FX 100 MSDS 031213Document5 pagesFX 100 MSDS 031213Achraf Ben DhifallahNo ratings yet
- Module 6Document26 pagesModule 6xtnreyesNo ratings yet
- Yojana - July - 2022 - On TribalsDocument41 pagesYojana - July - 2022 - On TribalsNAMANNo ratings yet
- Medical Ethics: Introduction To Basic PrinciplesDocument19 pagesMedical Ethics: Introduction To Basic PrinciplessatyachakrabortyNo ratings yet
- The Kaohsiung J of Med Scie - 2013 - Tsai - Pyoderma Gangrenosum Intractable Leg Ulcers in Sjogren S SyndromeDocument2 pagesThe Kaohsiung J of Med Scie - 2013 - Tsai - Pyoderma Gangrenosum Intractable Leg Ulcers in Sjogren S SyndromeAsad KakarNo ratings yet
- Group1 Week8298Document54 pagesGroup1 Week8298ABEGAIL BALLORANNo ratings yet
- Trixie Ann C. Salasibar BSN 2B-2DDocument6 pagesTrixie Ann C. Salasibar BSN 2B-2Dann camposNo ratings yet
- Rads - What To Order PDFDocument4 pagesRads - What To Order PDFsgod34No ratings yet
- Canmedaj01540 0049Document4 pagesCanmedaj01540 0049ImanNo ratings yet
- Helen's Story EBookFINALDocument19 pagesHelen's Story EBookFINALGMDMNo ratings yet
- Saying Good Goodbyes To Your ClientsDocument7 pagesSaying Good Goodbyes To Your ClientsVartaxNo ratings yet
- Barrientos Case Presentation Severe TetanusDocument10 pagesBarrientos Case Presentation Severe TetanusCalingalan Hussin CaluangNo ratings yet
- Bio Medical Waste Authorization Certificate: Haryana State Pollution Control BoardDocument3 pagesBio Medical Waste Authorization Certificate: Haryana State Pollution Control BoardManishNo ratings yet
- NCLEX IFC Virtual Class Rundown Questionnaire PDFDocument8 pagesNCLEX IFC Virtual Class Rundown Questionnaire PDFGrishma BudhathokiNo ratings yet
- Lean Body DietDocument68 pagesLean Body DietManiraj PalanikaniNo ratings yet
- Shikimic Acid Might Interrupt Spike Protein Functionality - Peak ProsperityDocument6 pagesShikimic Acid Might Interrupt Spike Protein Functionality - Peak ProsperityMas ThulanNo ratings yet
- 2011 Anglu K VBE PagrDocument16 pages2011 Anglu K VBE PagrTomas GuNo ratings yet
- STLS NVQ 3 CCLD NVQ 3 Unit 202 Witness Statement Unit 3 Element 3.2Document2 pagesSTLS NVQ 3 CCLD NVQ 3 Unit 202 Witness Statement Unit 3 Element 3.2Doodah2No ratings yet
- Division of Cebu Province: Curriculum Implementation Supervisory Plan (Cisp) SY 2018-2019Document3 pagesDivision of Cebu Province: Curriculum Implementation Supervisory Plan (Cisp) SY 2018-2019Charie P. GraciaNo ratings yet
- Medi 99 E11005Document6 pagesMedi 99 E11005maninagaNo ratings yet
- Proposal Form New India Mediclaim Policy 01102021Document6 pagesProposal Form New India Mediclaim Policy 01102021abcdefabcNo ratings yet
- Executive Order 202-202.67 (October 5)Document143 pagesExecutive Order 202-202.67 (October 5)OANo ratings yet
- Clinical Settings in Psychiatry: Psychiatric Nurses PerspectiveDocument30 pagesClinical Settings in Psychiatry: Psychiatric Nurses PerspectiveAnni BarbaNo ratings yet
- Risk AnalysisDocument50 pagesRisk AnalysisMunish DograNo ratings yet
- Burn and Reconstructive Centers of Colorado at Swedish Medical Center Raises Burn AwarenessDocument3 pagesBurn and Reconstructive Centers of Colorado at Swedish Medical Center Raises Burn AwarenessPR.comNo ratings yet
- RTOG 0529 IMRT Anal CancerDocument57 pagesRTOG 0529 IMRT Anal CancergammasharkNo ratings yet
- Chapter 1 - Group 1Document9 pagesChapter 1 - Group 1Wil UfanaNo ratings yet