You might also like
- Mẫu giấy KSK song ngữDocument3 pagesMẫu giấy KSK song ngữNguyen LawlietNo ratings yet
- Blood Donation Application FormDocument2 pagesBlood Donation Application FormFadjar MulyaNo ratings yet
- Admissions Medical ApplicationDocument2 pagesAdmissions Medical ApplicationkesnaNo ratings yet
- Kel 4 DM 1Document19 pagesKel 4 DM 1nabilaNo ratings yet
- Format Gadar IriDocument10 pagesFormat Gadar IriDianarisqiya WatiNo ratings yet
- Medical Examination - FormDocument3 pagesMedical Examination - FormVivek KumarNo ratings yet
- Merck Interest AreasDocument40 pagesMerck Interest AreasPhil MurrayNo ratings yet
- Pemeriksaan Kesihatan BiDocument3 pagesPemeriksaan Kesihatan BiWilson LimNo ratings yet
- Format Resume & AskepDocument26 pagesFormat Resume & AskepDinah ChieGadiz VerowhiteBlueNo ratings yet
- 3.medical FormDocument5 pages3.medical Formamistudio30No ratings yet
- Progestogen-Only ContraceptivesDocument22 pagesProgestogen-Only ContraceptivesazifadewiatasyaNo ratings yet
- Resume Keperawatan Pasien Medik Ruang Instalasi Gawat Darurat Sekolah Tinggi Ilmu Kesehatan Sari MuliaDocument15 pagesResume Keperawatan Pasien Medik Ruang Instalasi Gawat Darurat Sekolah Tinggi Ilmu Kesehatan Sari MuliasrirusmilaNo ratings yet
- Anxiety Depression QuestionnaireDocument2 pagesAnxiety Depression QuestionnairetatacrtNo ratings yet
- TN TRA Blood Donor QuestionnaireDocument2 pagesTN TRA Blood Donor QuestionnaireEman KarisNo ratings yet
- Lampiran Format Askep KtiDocument59 pagesLampiran Format Askep KtiAyu DwiraNo ratings yet
- National Hospital Discharge Survey 1978Document86 pagesNational Hospital Discharge Survey 1978Arjun RaoNo ratings yet
- Physical Fitness Certificate Form Revised 1910 Mysore Service RegulationsDocument1 pagePhysical Fitness Certificate Form Revised 1910 Mysore Service Regulationsdilip50% (8)
- Format Soap PNCDocument3 pagesFormat Soap PNCDewi KurniantyNo ratings yet
- Schizophrenia HandbookDocument268 pagesSchizophrenia HandbookArchana JMNo ratings yet
- I.M.E. Life Insurance Company LTD.: Physician'S Statement For Critical IllnessDocument2 pagesI.M.E. Life Insurance Company LTD.: Physician'S Statement For Critical IllnessMystic MilanNo ratings yet
- Admissions Medical ApplicationDocument2 pagesAdmissions Medical ApplicationDajueNo ratings yet
- Cochrane: LibraryDocument81 pagesCochrane: LibraryeczhilalcilogluNo ratings yet
- Health Questionaire: Public Service of NamibiaDocument2 pagesHealth Questionaire: Public Service of NamibiaHelen IngaNamibiaNo ratings yet
- Format Asuhan Keperawatan Medikal BedahDocument9 pagesFormat Asuhan Keperawatan Medikal Bedahkhairunisa AnnurNo ratings yet
- Lamp 1 Format KMB For UDocument9 pagesLamp 1 Format KMB For UAgusTinusNo ratings yet
- Medical Form 24.10.2023Document1 pageMedical Form 24.10.2023gdspriyadarshana84No ratings yet
- AutoRecovery save of revised MEDICAL EXAMINATION REPORTDocument3 pagesAutoRecovery save of revised MEDICAL EXAMINATION REPORTFred mungaNo ratings yet
- Women's Encyclopedia of Natural Medicine: Alternative Therapies and Integrative Medicine for Total Health and WellnessFrom EverandWomen's Encyclopedia of Natural Medicine: Alternative Therapies and Integrative Medicine for Total Health and WellnessRating: 5 out of 5 stars5/5 (7)
- Summary Health Statistics For U.S. Adults: National Health Interview Survey, 2012Document171 pagesSummary Health Statistics For U.S. Adults: National Health Interview Survey, 2012Zulfikar BasriNo ratings yet
- History Model in Pediatrics Course: Personal DataDocument6 pagesHistory Model in Pediatrics Course: Personal DataAbdullahNo ratings yet
- Obstetric & Gynecology Departement Medical School / General Hospital FK UKIDocument7 pagesObstetric & Gynecology Departement Medical School / General Hospital FK UKIImanuel CristiantoNo ratings yet
- Young People With CancerDocument120 pagesYoung People With Cancerandra1982100% (1)
- Preventing Disease Through A Healthier and Safer WorkplaceDocument100 pagesPreventing Disease Through A Healthier and Safer WorkplaceRudolof YaroserayNo ratings yet
- Format LatuDocument9 pagesFormat Latuwira adi antariNo ratings yet
- Format ICU NewDocument18 pagesFormat ICU NewNovie AhdiyatNo ratings yet
- Medical Form For StudentsDocument1 pageMedical Form For Studentssafsafu786No ratings yet
- Annex II: 2. Family HistoryDocument4 pagesAnnex II: 2. Family HistoryFeteneNo ratings yet
- 029 General SurgeryDocument4 pages029 General Surgeryعبدالله الرعويNo ratings yet
- TA Medical CertificateDocument1 pageTA Medical CertificateLuthra&Chandelia InvestigationsNo ratings yet
- Medical CertificateDocument1 pageMedical CertificateArsalan RaisaniNo ratings yet
- Format ASKEP KMBDocument15 pagesFormat ASKEP KMBayutyasNo ratings yet
- ? - 9 Dec 2020 2Document1 page? - 9 Dec 2020 2wafaa moNo ratings yet
- Case Study-Adult NursingDocument10 pagesCase Study-Adult NursingٌREEM ALINo ratings yet
- Format Askeb BayiDocument4 pagesFormat Askeb BayijihanNo ratings yet
- Show PDFDocument2 pagesShow PDFSandip MandalNo ratings yet
- History TakingDocument2 pagesHistory TakingMnsor svNo ratings yet
- Medical Report: Name: Rank: Nationality: Address: Manning AgentDocument4 pagesMedical Report: Name: Rank: Nationality: Address: Manning AgentМарина ГанжинаNo ratings yet
- Psoriasis Solution EbookDocument102 pagesPsoriasis Solution EbookKristen ForsytheNo ratings yet
- Induction Booklet - Final VersionDocument60 pagesInduction Booklet - Final VersionMuhammad YousufNo ratings yet
- Gynecology surgical documentation guideDocument147 pagesGynecology surgical documentation guideMohammadAbuelhaija100% (4)
- Confidential: Medical History and Personal Particulars of Students Joining at IIT MadrasDocument4 pagesConfidential: Medical History and Personal Particulars of Students Joining at IIT MadrasNehaNo ratings yet
- Delhi Public School, Mathura Road, New Delhi-110003: Health History (Part-I)Document2 pagesDelhi Public School, Mathura Road, New Delhi-110003: Health History (Part-I)shoaibali09usNo ratings yet
- Medical Certificate of AppDocument2 pagesMedical Certificate of AppRaju RajNo ratings yet
- Keterangan Sebab Kematian: Rs. Surya Asih PringsewuDocument1 pageKeterangan Sebab Kematian: Rs. Surya Asih PringsewuAtika Eka RachmayatiNo ratings yet
- 2 PDFDocument47 pages2 PDFRista RiaNo ratings yet
- Prasalnik ENDocument7 pagesPrasalnik ENDamjanNo ratings yet
- Gut Core HealingDocument54 pagesGut Core Healinganafagulha100% (2)
- Printable Weekly Expense ReportDocument1 pagePrintable Weekly Expense ReportXYZNo ratings yet
- Generic Travel Expense ReportDocument1 pageGeneric Travel Expense ReportXYZNo ratings yet
- Monthly Sales Expense ReportDocument1 pageMonthly Sales Expense ReportXYZNo ratings yet
- Expenditure ReportDocument8 pagesExpenditure ReportXYZNo ratings yet
- Printable Weekly Expense ReportDocument1 pagePrintable Weekly Expense ReportXYZNo ratings yet
- Monthly Expense Summary ReportDocument26 pagesMonthly Expense Summary ReportXYZNo ratings yet
- Monthly Travel Expense ReportDocument2 pagesMonthly Travel Expense ReportXYZNo ratings yet
- Printable Monthly Expense ReportDocument2 pagesPrintable Monthly Expense ReportXYZNo ratings yet
- Weekly Expense Report (Company Name / Logo) : Employee Name: Email: Phone: Manager Name: Purpose: Department: LocationDocument2 pagesWeekly Expense Report (Company Name / Logo) : Employee Name: Email: Phone: Manager Name: Purpose: Department: LocationXYZNo ratings yet
- Monthly Personal Expense ReportDocument2 pagesMonthly Personal Expense ReportXYZNo ratings yet
- Monthly Business Expense ReportDocument3 pagesMonthly Business Expense ReportXYZNo ratings yet
- Free Annual Expense ReportDocument3 pagesFree Annual Expense ReportXYZNo ratings yet
- Patient Injury Incident ReportDocument2 pagesPatient Injury Incident ReportXYZNo ratings yet
- Monthly Mileage Expense ReportDocument2 pagesMonthly Mileage Expense ReportXYZNo ratings yet
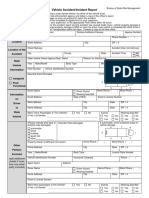
- Company Vehicle Incident ReportDocument2 pagesCompany Vehicle Incident ReportXYZNo ratings yet
- Patient Safety Incident ReportDocument2 pagesPatient Safety Incident ReportXYZNo ratings yet
- Physician. Submittal of A Completed DWC-1 ClaimDocument2 pagesPhysician. Submittal of A Completed DWC-1 ClaimXYZNo ratings yet
- Small Business Expense ReportDocument7 pagesSmall Business Expense ReportXYZNo ratings yet
- Dental Office Incident ReportDocument2 pagesDental Office Incident ReportXYZNo ratings yet
- Nursing Home Incident ReportDocument30 pagesNursing Home Incident ReportXYZNo ratings yet
- Patient Fall Incident ReportDocument2 pagesPatient Fall Incident ReportXYZ100% (1)
- Information Security Incident ReportDocument3 pagesInformation Security Incident ReportHoney Nhassie Marie GonzagaNo ratings yet
- 006 Sample of Report Form F15-11R1-ADocument4 pages006 Sample of Report Form F15-11R1-AZilma MarquesNo ratings yet
- NTCC Employee Accident Report FormDocument3 pagesNTCC Employee Accident Report FormXYZNo ratings yet
- Business Reports: Preparing and Planning: The Audience and The PurposeDocument5 pagesBusiness Reports: Preparing and Planning: The Audience and The Purposenaytunaung7650No ratings yet
- Market ReportDocument19 pagesMarket ReportXYZNo ratings yet
- Fire Incident ReportDocument18 pagesFire Incident ReportXYZNo ratings yet
- Business Reports: Preparing and Planning: The Audience and The PurposeDocument5 pagesBusiness Reports: Preparing and Planning: The Audience and The Purposenaytunaung7650No ratings yet
- Accident Report: (Other Than Motor Vehicle)Document2 pagesAccident Report: (Other Than Motor Vehicle)XYZNo ratings yet
- 22 Imobilisasi Pada Usia LanjutDocument34 pages22 Imobilisasi Pada Usia LanjutGian KalalembangNo ratings yet
- Global Resort List by Country (38 charactersDocument51 pagesGlobal Resort List by Country (38 charactersMaulik ShahNo ratings yet
- Magellans of The Sky - Prologue - Summer 2010Document12 pagesMagellans of The Sky - Prologue - Summer 2010Prologue MagazineNo ratings yet
- The Following Functional Health Pattern Assessment Is Based On A 65 Year Old Scottish Woman Who Lives Independently With Her Husband in Their Home at Happy ValleyDocument9 pagesThe Following Functional Health Pattern Assessment Is Based On A 65 Year Old Scottish Woman Who Lives Independently With Her Husband in Their Home at Happy ValleyJajangNo ratings yet
- SampleDocument8 pagesSampleAntônioNo ratings yet
- Chapter 1 and 2Document67 pagesChapter 1 and 2Tle SupawidNo ratings yet
- Effect of Water Immersion On Mechanical Properties of Polyurethane ...Document8 pagesEffect of Water Immersion On Mechanical Properties of Polyurethane ...konshoeNo ratings yet
- Nursing TheoriesDocument9 pagesNursing TheoriesMichelleneChenTadleNo ratings yet
- Aula 4 - Wooten - Organizational FieldsDocument28 pagesAula 4 - Wooten - Organizational FieldsferreiraccarolinaNo ratings yet
- Packaging Materials and Handling Technique: Dr. Ranjeet SinghDocument48 pagesPackaging Materials and Handling Technique: Dr. Ranjeet Singharon demagiba100% (1)
- Ac+lic Lab Manual 2018-19Document76 pagesAc+lic Lab Manual 2018-19Samanvi SaatviNo ratings yet
- Principles of Marketing - Product, Service and Experience DifferencesDocument26 pagesPrinciples of Marketing - Product, Service and Experience DifferencesVivien Leigh LopezNo ratings yet
- Line Pack Presentation - Dec 2018Document7 pagesLine Pack Presentation - Dec 2018Goran JakupovićNo ratings yet
- C32 MOTOR CAT Electronic Unit Injector - TestDocument2 pagesC32 MOTOR CAT Electronic Unit Injector - TestFreddy Villegas100% (1)
- Israel Is The MessIahDocument288 pagesIsrael Is The MessIahTeerayoot NoidaNo ratings yet
- Concept of StateDocument10 pagesConcept of StateAryansh ShuklaNo ratings yet
- Solvent Extraction: Please Submit Question 4 For MarkingDocument3 pagesSolvent Extraction: Please Submit Question 4 For MarkingThembi Matebula100% (1)
- Monthly Fire Extinguisher Inspection ChecklistDocument2 pagesMonthly Fire Extinguisher Inspection ChecklistisaacbombayNo ratings yet
- Estimating Hb Levels with Sahli's MethodDocument13 pagesEstimating Hb Levels with Sahli's MethodSANANo ratings yet
- Foundation of EducationDocument31 pagesFoundation of EducationM T Ząřřąř100% (1)
- Juxtaposition and Non Motion Varese BridDocument13 pagesJuxtaposition and Non Motion Varese BridIvan Eiji Yamauchi SimurraNo ratings yet
- ZTE UMTS KPI Optimization Analysis Guide V1 1 1Document62 pagesZTE UMTS KPI Optimization Analysis Guide V1 1 1GetitoutLetitgo100% (1)
- 2011 02 Huijben Spie Why Every Urea Plant Needs A Continuous NC Meter PDFDocument9 pages2011 02 Huijben Spie Why Every Urea Plant Needs A Continuous NC Meter PDFfawadintNo ratings yet
- Bipolar I Disorder Case ExampleDocument6 pagesBipolar I Disorder Case ExampleGrape JuiceNo ratings yet
- Design of Temporary Floating Road for Construction SiteDocument6 pagesDesign of Temporary Floating Road for Construction SiteAnonymous hRWwL7pZnCNo ratings yet
- Subjects Verbs PrepositionsDocument11 pagesSubjects Verbs Prepositionsგუგა ნოსელიძეNo ratings yet
- Anatomy of A Plated HoleDocument5 pagesAnatomy of A Plated Holepbs0707No ratings yet
- Caelus TT - Caelus Product TrainingDocument93 pagesCaelus TT - Caelus Product TrainingYader Daniel Ortiz CerdaNo ratings yet
- Whirlpool - Service Information Frontloader Washing Machine AWO/D 43115Document53 pagesWhirlpool - Service Information Frontloader Washing Machine AWO/D 43115amandialopes50% (2)
- PTC Document Status: (Updated 11 November 2015)Document5 pagesPTC Document Status: (Updated 11 November 2015)AndersonGabriel23No ratings yet