You might also like
- Damon Jco 2012-11-667.PDF Dr. DamonDocument12 pagesDamon Jco 2012-11-667.PDF Dr. DamonАнна ЛужковскаяNo ratings yet
- The Child Medication Fact Book for Psychiatric PracticeFrom EverandThe Child Medication Fact Book for Psychiatric PracticeRating: 5 out of 5 stars5/5 (1)
- Chapter 1 - Intro Current Concepts and Clinical Decision Making in Electrotherapy PDFDocument7 pagesChapter 1 - Intro Current Concepts and Clinical Decision Making in Electrotherapy PDFTracy Magpoc0% (1)
- Energy Medicine Paper - Energy PsychologyDocument13 pagesEnergy Medicine Paper - Energy Psychologyapi-281779476No ratings yet
- Caregiver ResponsibilitiesDocument27 pagesCaregiver ResponsibilitiesRodolfo CorpuzNo ratings yet
- 2015 - DR Karl Maret-OverviewDocument171 pages2015 - DR Karl Maret-Overviewrooiberg100% (3)
- Facial NerveDocument45 pagesFacial Nerveyudhafp100% (1)
- WsasDocument2 pagesWsasFerdencel LaranangNo ratings yet
- Preservative Formulation and Effectiveness in Oral Solutions and Suspensions PDFDocument57 pagesPreservative Formulation and Effectiveness in Oral Solutions and Suspensions PDFethylenepluschlorine100% (1)
- Activated Carbon For Waste Water Treatment v2 NDocument8 pagesActivated Carbon For Waste Water Treatment v2 NMohammed A. Helal100% (1)
- Monografi AtropinDocument48 pagesMonografi AtropinWahyu AgustinaNo ratings yet
- HP Root Cause Testing GuideDocument9 pagesHP Root Cause Testing GuideNatasa EricNo ratings yet
- Acog Nausea Vomiting PregnancyDocument13 pagesAcog Nausea Vomiting PregnancymispNo ratings yet
- Detailed Lesson Plan in TLE 10 (Wellness Massage) : Nicanor David Vergara High SchoolDocument4 pagesDetailed Lesson Plan in TLE 10 (Wellness Massage) : Nicanor David Vergara High SchoolFatima Dela Cruz Lascano50% (2)
- DTH 13548Document7 pagesDTH 13548Bryan NguyenNo ratings yet
- Ab Si Acnee VulgaraDocument9 pagesAb Si Acnee Vulgaraapotek padasukaNo ratings yet
- Terapi Akne Ciproterone Acetate Oleh Dr. Abraham Arimuko SPKK Mars Finsdv FaadvDocument32 pagesTerapi Akne Ciproterone Acetate Oleh Dr. Abraham Arimuko SPKK Mars Finsdv FaadvshabrinaerinNo ratings yet
- Biosimilars - So Where Are We in The EU?: Robert WilliamsDocument14 pagesBiosimilars - So Where Are We in The EU?: Robert WilliamsPhani KumarNo ratings yet
- Top 10 Perlas Clã Nicas en Acne Dermatologic Clinics 2015Document11 pagesTop 10 Perlas Clã Nicas en Acne Dermatologic Clinics 2015Yulay HBNo ratings yet
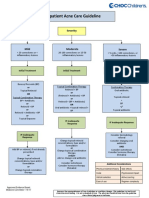
- Outpatient Acne Care Guideline: SeverityDocument5 pagesOutpatient Acne Care Guideline: SeverityMarrauNo ratings yet
- 10 1016@j Jpba 2014 06 010Document7 pages10 1016@j Jpba 2014 06 010tahafeNo ratings yet
- Management of Poisoning - Booklet PDFDocument344 pagesManagement of Poisoning - Booklet PDFkrysteenNo ratings yet
- Side Effects of Retinoid Therapy On The Quality of Vision: DOI: 10.1515/acph-2016-0039Document8 pagesSide Effects of Retinoid Therapy On The Quality of Vision: DOI: 10.1515/acph-2016-0039Ulul AzmiNo ratings yet
- EMEA - BioSimilar Guidelines 2Document32 pagesEMEA - BioSimilar Guidelines 2Shrinivas TamaskarNo ratings yet
- Mono Red Clover Isoflavone Extract EnglishDocument6 pagesMono Red Clover Isoflavone Extract EnglishTom DelongeNo ratings yet
- IMW025.04 Immunoglobulin Handbood Diphtheria Update AUG 2018 v2Document9 pagesIMW025.04 Immunoglobulin Handbood Diphtheria Update AUG 2018 v2Ak62442No ratings yet
- Management of SepsisDocument10 pagesManagement of SepsisJahangir AlamNo ratings yet
- Article WJPR 1490959171Document6 pagesArticle WJPR 1490959171diva syifaniNo ratings yet
- Experiment No. 1: Pre-Laboratory Review SheetDocument2 pagesExperiment No. 1: Pre-Laboratory Review SheetGraciel Iris ArupoNo ratings yet
- 2020-08-24 Drug Discovery & DevelopmentDocument25 pages2020-08-24 Drug Discovery & DevelopmentGalz RoomNo ratings yet
- Biological Methods IVDocument69 pagesBiological Methods IVFitsum DemissieNo ratings yet
- Journal of Chemical and Pharmaceutical Research, 2015, 7 (7) :274-282Document9 pagesJournal of Chemical and Pharmaceutical Research, 2015, 7 (7) :274-282indra hennyNo ratings yet
- Morgan, Breyonna-Principles of Toxicology-Chapter 1 AssignmentDocument4 pagesMorgan, Breyonna-Principles of Toxicology-Chapter 1 AssignmentBreyonnaMorganNo ratings yet
- Ragelle - Nanoemulsion Formulation of Fisetin Improves Bioavailability and Antitumour Activity in Mice - 2012Document8 pagesRagelle - Nanoemulsion Formulation of Fisetin Improves Bioavailability and Antitumour Activity in Mice - 2012thrNo ratings yet
- Efficacy, Safety and Tolerability of Tiger Balm® Ointments: A Systematic Review and A Meta-Analysis of PrevalenceDocument18 pagesEfficacy, Safety and Tolerability of Tiger Balm® Ointments: A Systematic Review and A Meta-Analysis of Prevalencesidra anjumNo ratings yet
- Acute Intermittent Porphyria: The Right Clinical Information, Right Where It's NeededDocument29 pagesAcute Intermittent Porphyria: The Right Clinical Information, Right Where It's NeededMUHAMMAD09No ratings yet
- Report Cphi South East Asia 2012Document15 pagesReport Cphi South East Asia 2012dedieNo ratings yet
- ParekhDocument4 pagesParekhmominul haqueNo ratings yet
- Thioguanine 20 MG - ML Oral Suspension PDFDocument4 pagesThioguanine 20 MG - ML Oral Suspension PDFAlexander MeloNo ratings yet
- 144TD (C) 25 (E3) - Issue No 4 - Ear Nose and Throat (ENT) Infections Antibiotic GuidelinesDocument9 pages144TD (C) 25 (E3) - Issue No 4 - Ear Nose and Throat (ENT) Infections Antibiotic GuidelinesOprea DoruNo ratings yet
- Widal Test Teaching Kit (Tube Test)Document6 pagesWidal Test Teaching Kit (Tube Test)Jeje Mystearica100% (1)
- Dr. Ricky Yue - Allergic RhinitisDocument27 pagesDr. Ricky Yue - Allergic RhinitisLydwiNa JcNo ratings yet
- The Role of Dissolution Testing in Complementary and African Traditional Medicines: Development of Methods and ApplicationsDocument21 pagesThe Role of Dissolution Testing in Complementary and African Traditional Medicines: Development of Methods and ApplicationsPriyanshu JainNo ratings yet
- Introduction To Evidence-Based MedicineDocument28 pagesIntroduction To Evidence-Based Medicinedila2706No ratings yet
- Protein Solubility and Stability KitsDocument30 pagesProtein Solubility and Stability KitsSoluble BioScienceNo ratings yet
- In Vivo and in Vitro Efficacy of Florfenicol, Terbinafine, and Mometasone Furoate Topical Otic Solution For The Treatment of Canine Otitis ExternaDocument6 pagesIn Vivo and in Vitro Efficacy of Florfenicol, Terbinafine, and Mometasone Furoate Topical Otic Solution For The Treatment of Canine Otitis ExternaEvandro D'OrnellasNo ratings yet
- Efficacy and Adverse Events of Oral Isotretinoin For Acne: A Systematic ReviewDocument23 pagesEfficacy and Adverse Events of Oral Isotretinoin For Acne: A Systematic Reviewjnn drewjnNo ratings yet
- Is It A Clinical Trial of A Medicinal Product?Document2 pagesIs It A Clinical Trial of A Medicinal Product?Colin DidotNo ratings yet
- Biuret-Gornall Protein Assay: Product DescriptionDocument3 pagesBiuret-Gornall Protein Assay: Product Descriptioninsiya insiyaNo ratings yet
- Tadatrona ParDocument6 pagesTadatrona Parzakarya wadiNo ratings yet
- Generic NameDocument2 pagesGeneric NameIrene Hechanova Completo-BatomalaqueNo ratings yet
- Hepatitis C Treatments in Current Clinical Development Alan Franciscus Editor-in-ChiefDocument32 pagesHepatitis C Treatments in Current Clinical Development Alan Franciscus Editor-in-ChiefAhmed KamelNo ratings yet
- EJMCM - Volume 9 - Issue 7 - Pages 8448-8453 PDFDocument6 pagesEJMCM - Volume 9 - Issue 7 - Pages 8448-8453 PDFVijayakumarNo ratings yet
- Delfia Hafp A004-201 enDocument21 pagesDelfia Hafp A004-201 enJonny MossNo ratings yet
- Poractant Alfa Versus Bovine Lipid Extract Surfactant For Infants 24+0 To 31+6 Weeks Gestational Age: A Randomized Controlled TrialDocument14 pagesPoractant Alfa Versus Bovine Lipid Extract Surfactant For Infants 24+0 To 31+6 Weeks Gestational Age: A Randomized Controlled TrialBryan HoriandoNo ratings yet
- Chemistry in Everyday LifeDocument108 pagesChemistry in Everyday LifeBoss OfficialNo ratings yet
- BILT3 en V6Document4 pagesBILT3 en V6Fahrurrozi AdanNo ratings yet
- Comvac5 BrochureDocument2 pagesComvac5 BrochureSai SapNo ratings yet
- Pharmacokinetic Testing For Systemic Exposure of Orally Inhaled and Nasal DrugsDocument24 pagesPharmacokinetic Testing For Systemic Exposure of Orally Inhaled and Nasal Drugsmjamil0995No ratings yet
- Formulation and Evaluation of Novel HerbalThroat Spray Containing Triphala and Liquorice ExtractsDocument6 pagesFormulation and Evaluation of Novel HerbalThroat Spray Containing Triphala and Liquorice ExtractsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Management of Sore Throats in ChildrenDocument8 pagesManagement of Sore Throats in ChildrenelisabethNo ratings yet
- Guideline PneumoniaDocument12 pagesGuideline PneumoniaNanthakumar GovindNo ratings yet
- Study of The Acceptability of Antibiotic Syrups, Suspensions, and Oral Solutions Prescribed To Pediatric OutpatientsDocument7 pagesStudy of The Acceptability of Antibiotic Syrups, Suspensions, and Oral Solutions Prescribed To Pediatric OutpatientsBeatriz PatricioNo ratings yet
- January 1-2021Document76 pagesJanuary 1-2021Aseel AlsheeshNo ratings yet
- ARCO PP+ Total Skin: Plant PlacentaDocument27 pagesARCO PP+ Total Skin: Plant PlacentaRatu Lucky Baskara PutriNo ratings yet
- Pengantar FarmakologiDocument18 pagesPengantar FarmakologiHaidar AdiNo ratings yet
- Medicine (Pharmaceutical Chemistry)Document33 pagesMedicine (Pharmaceutical Chemistry)Crizaldo MempinNo ratings yet
- Verbeeck 2017Document35 pagesVerbeeck 2017giyan77No ratings yet
- Biological MethodsDocument91 pagesBiological MethodsnahomNo ratings yet
- Electroconvulsive Therapy (ECT) : Dr. Altaf Qadir Khan Professor of Psychiatry PGMI/ LGH, LahoreDocument44 pagesElectroconvulsive Therapy (ECT) : Dr. Altaf Qadir Khan Professor of Psychiatry PGMI/ LGH, LahoreAalia RanaNo ratings yet
- Norman 2017Document7 pagesNorman 2017Lee HaeunNo ratings yet
- Clinical Features AstriDocument3 pagesClinical Features AstriDian Sulistya EkaputriNo ratings yet
- Day 28 - Resource 5a - Designer Babies-Ethical ConsiderationsDocument6 pagesDay 28 - Resource 5a - Designer Babies-Ethical Considerationsapi-281167422No ratings yet
- Conceptual Practice Model Final VersionDocument12 pagesConceptual Practice Model Final Versiongkempf10No ratings yet
- Chemicals For ConsumersDocument50 pagesChemicals For ConsumersAzie Nurul Akhtar100% (1)
- Parenteral Administration of DrugsDocument3 pagesParenteral Administration of DrugspauchanmnlNo ratings yet
- Conclusion. MassageDocument1 pageConclusion. MassagemimiNo ratings yet
- Write The Differences and Similarities Between Piaget and KohlbergDocument5 pagesWrite The Differences and Similarities Between Piaget and KohlbergsohailNo ratings yet
- Konsensus HiperbilirubinemiaDocument8 pagesKonsensus Hiperbilirubinemiaanggi6No ratings yet
- Harga Beli Mersifarma Ekatalog 2019Document3 pagesHarga Beli Mersifarma Ekatalog 2019Jemmy GeraldzNo ratings yet
- Bio Mechanics of Tooth MovementDocument26 pagesBio Mechanics of Tooth MovementPriyanka Wadhawan100% (1)
- List EDProductDocument2 pagesList EDProductAgung SiCowok AssikandUgalNo ratings yet
- Maybe Not For Me: Ethics in OrthodonticsDocument1 pageMaybe Not For Me: Ethics in OrthodonticsDominikaSkórkaNo ratings yet
- Case Presentation: EclampsiaDocument44 pagesCase Presentation: Eclampsiamutiara sitepuNo ratings yet
- PL - 761.1 - Rehabilitation Programme After Dynamic Hip Screw (DHS) SurgeryDocument8 pagesPL - 761.1 - Rehabilitation Programme After Dynamic Hip Screw (DHS) Surgeryfarid.mohamed96No ratings yet
- Pathogenesis of Diabetic Atherosclerosis PDFDocument15 pagesPathogenesis of Diabetic Atherosclerosis PDFtkgoon6349No ratings yet
- Exoskeletons in Rehabilitation Robotics PDFDocument2 pagesExoskeletons in Rehabilitation Robotics PDFSarahNo ratings yet
- DSM IV TR CriteriaDocument3 pagesDSM IV TR CriteriapatrayatiNo ratings yet
- List of Drugs: DRUGS Acting On ANS Respiratory DrugsDocument2 pagesList of Drugs: DRUGS Acting On ANS Respiratory DrugsShambhu AshokNo ratings yet