You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (843)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Electrical Engineering (EEE) Projects For Final Year StudentsDocument3 pagesElectrical Engineering (EEE) Projects For Final Year Studentsthyristorscr100% (3)
- Quality Circle Forum of India: Problem Solving TechniquesDocument88 pagesQuality Circle Forum of India: Problem Solving TechniquesSamNo ratings yet
- SetsDocument15 pagesSetsabulug nrvhsNo ratings yet
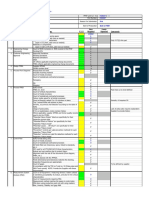
- SQD-025 PPAP ChecklistDocument7 pagesSQD-025 PPAP Checklist오동욱No ratings yet
- Comparative Evaluation of in Vitro Physicochemical Parameters of Some Commercially Available Metformin HCL 500mg Tablets in BangladeshDocument5 pagesComparative Evaluation of in Vitro Physicochemical Parameters of Some Commercially Available Metformin HCL 500mg Tablets in BangladeshInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Ville's ResearchDocument20 pagesVille's ResearchthedrdrownNo ratings yet
- Prediction of Kabaddi Playing AbilityDocument7 pagesPrediction of Kabaddi Playing AbilityIAEME PublicationNo ratings yet
- Handbook of Induction Heating: Second EditionDocument22 pagesHandbook of Induction Heating: Second EditionMohammed El-AwamryNo ratings yet
- Journal of ChemotherapyDocument23 pagesJournal of ChemotherapyomicspublishinggroupNo ratings yet
- ABC of DiabetesDocument111 pagesABC of DiabetesCandy E Ri ViNo ratings yet
- Advocacy EssayDocument8 pagesAdvocacy EssaySamantha SinghaNo ratings yet
- Chemtronics Flux-Off No Clean Safety Data SheetDocument11 pagesChemtronics Flux-Off No Clean Safety Data SheetMoisés Antonio Gamboa MartínezNo ratings yet
- Writing Assignment ECO313 Fall 2022Document5 pagesWriting Assignment ECO313 Fall 2022Maxwell MaundNo ratings yet
- Safety Manual B1Document78 pagesSafety Manual B1parthasarathipkNo ratings yet
- R-K Equation of StateDocument31 pagesR-K Equation of StateNAYAN SATISHKUMAR SHARMANo ratings yet
- Story Structure 2 Die 4Document56 pagesStory Structure 2 Die 4Naido Neji100% (2)
- Lesson 2 (Government Policies and Filipino Scientists)Document30 pagesLesson 2 (Government Policies and Filipino Scientists)Niñarita Fe BuotNo ratings yet
- Ren 4Document3 pagesRen 4ray72roNo ratings yet
- Spoil Pile SafetyDocument94 pagesSpoil Pile SafetymornewpNo ratings yet
- Elements Compound MixtureDocument42 pagesElements Compound MixtureRecilia MarthaNo ratings yet
- Binomial GreeksDocument11 pagesBinomial Greeksjshew_jr_junkNo ratings yet
- Articulo Cientifico Derivado Del FenilpropanoDocument23 pagesArticulo Cientifico Derivado Del FenilpropanoKaren GonzalezNo ratings yet
- Deficient Knowledge - NCPDocument2 pagesDeficient Knowledge - NCPEmmeline Dycangchon-GarmaNo ratings yet
- Impact AR500 PlateDocument2 pagesImpact AR500 PlateMario Diez100% (1)
- Handbook On Agroecology: Farmer's Manual On Sustainable Practices Different Agroecological PracticesDocument3 pagesHandbook On Agroecology: Farmer's Manual On Sustainable Practices Different Agroecological PracticesJanly ArroyoNo ratings yet
- Reading Comprehension Drill Tes Evaluasi Reading Comprehension 6Document5 pagesReading Comprehension Drill Tes Evaluasi Reading Comprehension 6Andi Muhammad Abigail Ghalib Athallah Surya PutraNo ratings yet
- 5 Electromagnetic Waves Sum QuestionDocument5 pages5 Electromagnetic Waves Sum QuestionDhanush Raman100% (1)
- SI-01 - R03 Banksman-Crane Operations PDFDocument64 pagesSI-01 - R03 Banksman-Crane Operations PDFFatih D. PrasetioNo ratings yet
- Does Dove Soap Make Chocolate - Google SearchDocument1 pageDoes Dove Soap Make Chocolate - Google SearchballfuckNo ratings yet
- AS1576.2, BS1139: Drop Forged Putlog CouplerDocument1 pageAS1576.2, BS1139: Drop Forged Putlog CoupleraraboooNo ratings yet