You might also like
- How to Be Loving: The Journal: Relax Your Mind. Connect with the Divine.From EverandHow to Be Loving: The Journal: Relax Your Mind. Connect with the Divine.Rating: 5 out of 5 stars5/5 (1)
- Patient Assessment Form: Assess Scene Secondary SurveyDocument2 pagesPatient Assessment Form: Assess Scene Secondary Surveydeepeezee_beenNo ratings yet
- One Minute Healing: The PAWS Distress Relief Technique, alleviating Pain, Anger, Worry, & Sadness * A Complete GuideFrom EverandOne Minute Healing: The PAWS Distress Relief Technique, alleviating Pain, Anger, Worry, & Sadness * A Complete GuideNo ratings yet
- Iii. Physical Assessment and Review of SystemDocument7 pagesIii. Physical Assessment and Review of SystemBiya MacunteNo ratings yet
- 2 Gordons GeriaDocument7 pages2 Gordons GeriaAiraa ShaneNo ratings yet
- RevisedDocument16 pagesRevisedZymer Lee AbasoloNo ratings yet
- 01 Nursing Note SampleDocument1 page01 Nursing Note Sampletesttest testNo ratings yet
- Heath Assessment ToolDocument8 pagesHeath Assessment ToolHouda Hayek100% (1)
- Gordon's Functional Health Pattern For Geriatric ClientsDocument8 pagesGordon's Functional Health Pattern For Geriatric ClientsGEN ERIGBUAGASNo ratings yet
- Related Learning Experience Requirements For Medical and Surgical Ward AreasDocument14 pagesRelated Learning Experience Requirements For Medical and Surgical Ward AreasDummy AccountNo ratings yet
- 13 Areas FormDocument3 pages13 Areas FormSareno PJhēaNo ratings yet
- History TakingDocument6 pagesHistory Takingdharti daveNo ratings yet
- SkeletonDocument3 pagesSkeletonGoody Freking FuttonNo ratings yet
- Lasustech Medical FormDocument2 pagesLasustech Medical FormAl MubarakNo ratings yet
- Medical FormDocument2 pagesMedical FormDuván ArleyNo ratings yet
- Antipolo City Senior High School District I-A: Last Menstruation Period: - (For Girls Only)Document2 pagesAntipolo City Senior High School District I-A: Last Menstruation Period: - (For Girls Only)Chlong ArtuzNo ratings yet
- Fitness Form & Hospital ListDocument15 pagesFitness Form & Hospital Listjohn thomasNo ratings yet
- Medical Certificate of Athlete: To Whom It May ConcernDocument3 pagesMedical Certificate of Athlete: To Whom It May ConcernRoderick CruzNo ratings yet
- Clinical Assessment Sheet 2Document2 pagesClinical Assessment Sheet 2Lidya StevensNo ratings yet
- Head To Toe Patient AssessmentDocument2 pagesHead To Toe Patient AssessmentJaypee Nuñez100% (2)
- Acute Abdomen WorkbookDocument11 pagesAcute Abdomen WorkbookFarid AkbarNo ratings yet
- New Assessment ToolDocument9 pagesNew Assessment Toolneri_pearlNo ratings yet
- Physical ExaminDocument1 pagePhysical ExaminВячеслав ЖадаевNo ratings yet
- Case Study 3 CVD Bleed HCVD Type 2 DM CICD Stage 5 WorksheetDocument27 pagesCase Study 3 CVD Bleed HCVD Type 2 DM CICD Stage 5 WorksheetJade HemmingsNo ratings yet
- Interview Pa Tool.Document5 pagesInterview Pa Tool.Raisah Bint AbdullahNo ratings yet
- Clinical Area: - Student NameDocument2 pagesClinical Area: - Student NamebunzelcakeNo ratings yet
- Cagayan de Oro City College of Nursing Assessment Form General InformationDocument11 pagesCagayan de Oro City College of Nursing Assessment Form General Informationdjanggo18No ratings yet
- Assessment Tool On Neurological System: Baseline DataDocument21 pagesAssessment Tool On Neurological System: Baseline DataK HepsibaNo ratings yet
- 3 Skin Hair NailsDocument1 page3 Skin Hair NailsSophia MarieNo ratings yet
- PT Intake FormDocument4 pagesPT Intake FormChifor FlorinNo ratings yet
- Day1application For Care History ADocument3 pagesDay1application For Care History Aapi-314956618No ratings yet
- Physical AssessmentDocument23 pagesPhysical AssessmentJack BangcoyoNo ratings yet
- Nursing Head To Toe Assessment Checklist Revised SP 2013Document3 pagesNursing Head To Toe Assessment Checklist Revised SP 2013clarimer100% (3)
- History Form IntroductoryDocument6 pagesHistory Form Introductoryrawan.abujodahNo ratings yet
- Physical Assessment ChecklistDocument3 pagesPhysical Assessment ChecklistMaria PunoNo ratings yet
- Form-1-Medical-Form-Back-to-back 2023-04-23 06 - 10 - 49Document2 pagesForm-1-Medical-Form-Back-to-back 2023-04-23 06 - 10 - 49Climaco EdwinNo ratings yet
- Physical Assessment Form (Adult)Document7 pagesPhysical Assessment Form (Adult)Mart Juaresa YambaoNo ratings yet
- Students Medical RecordDocument2 pagesStudents Medical RecordMary Grace EncisaNo ratings yet
- CRT 7Document8 pagesCRT 7api-643868511No ratings yet
- Physical Assessment ChecklistDocument3 pagesPhysical Assessment ChecklistEm NagalNo ratings yet
- Physical Assessment ChecklistDocument3 pagesPhysical Assessment ChecklistIsang ButaNo ratings yet
- BFI Annual Medical Fitness Certificate-6Document3 pagesBFI Annual Medical Fitness Certificate-6JalajNo ratings yet
- Mohammad Almana College For Medical Sciences Division of NursingDocument13 pagesMohammad Almana College For Medical Sciences Division of NursingAmalNo ratings yet
- 030 - Blood Transfusion Vital Signs SheetDocument3 pages030 - Blood Transfusion Vital Signs Sheetعبدالله الرعويNo ratings yet
- Sleep 50 QuestionnaireDocument5 pagesSleep 50 QuestionnaireSónia Alves100% (1)
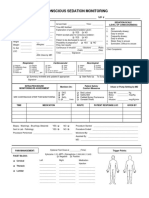
- 34 An Consious Sedation MonitoringDocument2 pages34 An Consious Sedation Monitoringabu alauon abed almohsenNo ratings yet
- Radiant Healing Hypnosis: Thank You For Following Your Heart To MineDocument7 pagesRadiant Healing Hypnosis: Thank You For Following Your Heart To Mineapi-26417375No ratings yet
- JHS Remote PFA Module Activity SheetDocument16 pagesJHS Remote PFA Module Activity SheetJun MarkNo ratings yet
- Nursing Health Assessment Guide: San Pedro CollegeDocument3 pagesNursing Health Assessment Guide: San Pedro CollegeRue Cheng MaNo ratings yet
- Nursing Health Assessment Guide: San Pedro CollegeDocument3 pagesNursing Health Assessment Guide: San Pedro CollegeKim ZNo ratings yet
- QVASDocument1 pageQVASAnjaswati Farida AdyanaNo ratings yet
- 2017 MedicalCertificate For Boxing 2Document1 page2017 MedicalCertificate For Boxing 2Majhi PeraltaNo ratings yet
- Universal - Functional Analysis With Doppler ExaminationDocument3 pagesUniversal - Functional Analysis With Doppler ExaminationPP MulayNo ratings yet
- ACT1 Audition Form - Minor PDFDocument1 pageACT1 Audition Form - Minor PDFteenwolf4006No ratings yet
- NURS 225V Principles III Data Collection ToolDocument2 pagesNURS 225V Principles III Data Collection ToolKrisNo ratings yet
- Health History FormDocument1 pageHealth History Formapi-353679123No ratings yet
- Confidential Patient Information: C L C CDocument6 pagesConfidential Patient Information: C L C CPedroNo ratings yet
- Nursing Administration AssessmentDocument6 pagesNursing Administration Assessmentkatnebrija89No ratings yet
- Activity HilDocument1 pageActivity HilPORTEZANo ratings yet
- Patient PaperworkDocument6 pagesPatient Paperworkharrisk31No ratings yet
- JHS - MATH 7 - 2nd Grading Module - GERRY R. LOMBRESDocument60 pagesJHS - MATH 7 - 2nd Grading Module - GERRY R. LOMBRESIts BorabogNo ratings yet
- 2021 2022 Annual PlanDocument5 pages2021 2022 Annual PlanIts BorabogNo ratings yet
- E Portfolio Teachning InternshipDocument92 pagesE Portfolio Teachning InternshipIts BorabogNo ratings yet
- 2nd Quarter TOS Fil 5Document1 page2nd Quarter TOS Fil 5Its BorabogNo ratings yet
- 2nd Quarter TOS Fil 4Document1 page2nd Quarter TOS Fil 4Its BorabogNo ratings yet
- Sumerian 1Document12 pagesSumerian 1Its BorabogNo ratings yet
- Heimbach - Keeping Formingfabrics CleanDocument4 pagesHeimbach - Keeping Formingfabrics CleanTunç TürkNo ratings yet
- Applications SeawaterDocument23 pagesApplications SeawaterQatar home RentNo ratings yet
- Quarter 1 - Module 1Document31 pagesQuarter 1 - Module 1Roger Santos Peña75% (4)
- DBMS Lab ManualDocument57 pagesDBMS Lab ManualNarendh SubramanianNo ratings yet
- Sakui, K., & Cowie, N. (2012) - The Dark Side of Motivation - Teachers' Perspectives On 'Unmotivation'. ELTJ, 66 (2), 205-213.Document9 pagesSakui, K., & Cowie, N. (2012) - The Dark Side of Motivation - Teachers' Perspectives On 'Unmotivation'. ELTJ, 66 (2), 205-213.Robert HutchinsonNo ratings yet
- 1 in 8.5 60KG PSC Sleepers TurnoutDocument9 pages1 in 8.5 60KG PSC Sleepers Turnoutrailway maintenanceNo ratings yet
- Fundaciones Con PilotesDocument48 pagesFundaciones Con PilotesReddy M.Ch.No ratings yet
- An Evaluation of MGNREGA in SikkimDocument7 pagesAn Evaluation of MGNREGA in SikkimBittu SubbaNo ratings yet
- Journal of Biology EducationDocument13 pagesJournal of Biology EducationFarah ArrumyNo ratings yet
- Cisco BGP ASPATH FilterDocument115 pagesCisco BGP ASPATH FilterHalison SantosNo ratings yet
- Intellirent 2009 CatalogDocument68 pagesIntellirent 2009 Catalograza239No ratings yet
- Scholastica: Mock 1Document14 pagesScholastica: Mock 1Fatema KhatunNo ratings yet
- CL57T V4.0Document14 pagesCL57T V4.0dimitriNo ratings yet
- Clark SM 616 Service ManualDocument20 pagesClark SM 616 Service Manualenid100% (55)
- Julia Dito ResumeDocument3 pagesJulia Dito Resumeapi-253713289No ratings yet
- 40 People vs. Rafanan, Jr.Document10 pages40 People vs. Rafanan, Jr.Simeon TutaanNo ratings yet
- Neonatal Mortality - A Community ApproachDocument13 pagesNeonatal Mortality - A Community ApproachJalam Singh RathoreNo ratings yet
- Close Enough To Touch by Victoria Dahl - Chapter SamplerDocument23 pagesClose Enough To Touch by Victoria Dahl - Chapter SamplerHarlequinAustraliaNo ratings yet
- Progressive Muscle RelaxationDocument4 pagesProgressive Muscle RelaxationEstéphany Rodrigues ZanonatoNo ratings yet
- MCI Approved Medical College in Uzbekistan PDFDocument3 pagesMCI Approved Medical College in Uzbekistan PDFMBBS ABROADNo ratings yet
- Bom Details FormatDocument6 pagesBom Details FormatPrince MittalNo ratings yet
- A Survey On Security and Privacy Issues of Bitcoin-1Document39 pagesA Survey On Security and Privacy Issues of Bitcoin-1Ramineni HarshaNo ratings yet
- Student Exploration: Inclined Plane - Simple MachineDocument9 pagesStudent Exploration: Inclined Plane - Simple MachineLuka MkrtichyanNo ratings yet
- Nanolithography - Processing Methods PDFDocument10 pagesNanolithography - Processing Methods PDFNilesh BhardwajNo ratings yet
- Book 1518450482Document14 pagesBook 1518450482rajer13No ratings yet
- Bachelor of Arts in Theology: Christian Apologetics/ Seventh-Day Adventist Contemporary IssuesDocument13 pagesBachelor of Arts in Theology: Christian Apologetics/ Seventh-Day Adventist Contemporary IssuesRamel LigueNo ratings yet
- WAQF Podium Design Presentation 16 April 2018Document23 pagesWAQF Podium Design Presentation 16 April 2018hoodqy99No ratings yet
- WarringFleets Complete PDFDocument26 pagesWarringFleets Complete PDFlingshu8100% (1)
- SLA in PEGA How To Configue Service Level Agreement - HKRDocument7 pagesSLA in PEGA How To Configue Service Level Agreement - HKRsridhar varmaNo ratings yet
- CV Augusto Brasil Ocampo MedinaDocument4 pagesCV Augusto Brasil Ocampo MedinaAugusto Brasil Ocampo MedinaNo ratings yet