You might also like
- Nurse Assessment ChecklistDocument3 pagesNurse Assessment Checklistclarimer100% (3)
- Gordon's Functional Health Pattern For Geriatric ClientsDocument8 pagesGordon's Functional Health Pattern For Geriatric ClientsGEN ERIGBUAGASNo ratings yet
- I. Preoperative Assessment 1. Physical: Philippine Heart Center Perioperative Nursing RecordDocument2 pagesI. Preoperative Assessment 1. Physical: Philippine Heart Center Perioperative Nursing RecordERWINNo ratings yet
- 10 Adult Anesthesia Pre-Operative Evaluation FormDocument1 page10 Adult Anesthesia Pre-Operative Evaluation FormAina HaravataNo ratings yet
- 09 Living On The FrontlineDocument5 pages09 Living On The FrontlineAjitkumar PulagurthaNo ratings yet
- CASE PRES PreeclampsiaDocument51 pagesCASE PRES PreeclampsiaRaiza Love Caparas-PablicoNo ratings yet
- Acute Abdomen WorkbookDocument11 pagesAcute Abdomen WorkbookFarid AkbarNo ratings yet
- Cagayan de Oro City College of Nursing Assessment Form General InformationDocument11 pagesCagayan de Oro City College of Nursing Assessment Form General Informationdjanggo18No ratings yet
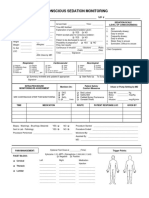
- 34 An Consious Sedation MonitoringDocument2 pages34 An Consious Sedation Monitoringabu alauon abed almohsenNo ratings yet
- CRT 7Document8 pagesCRT 7api-643868511No ratings yet
- Cardiac Tamponade: Tarlac State University College of Science Department of NursingDocument17 pagesCardiac Tamponade: Tarlac State University College of Science Department of NursingKrisianne Mae Lorenzo FranciscoNo ratings yet
- Atrial FibrillationDocument28 pagesAtrial FibrillationKrisianne Mae Lorenzo FranciscoNo ratings yet
- 01 Nursing Note SampleDocument1 page01 Nursing Note Sampletesttest testNo ratings yet
- Related Learning Experience Requirements For Medical and Surgical Ward AreasDocument14 pagesRelated Learning Experience Requirements For Medical and Surgical Ward AreasDummy AccountNo ratings yet
- Form "D" Report of Practical Experience: Nursing Clinical Practice IDocument29 pagesForm "D" Report of Practical Experience: Nursing Clinical Practice IAnderson RebaNo ratings yet
- Medical Ward RequirementsDocument16 pagesMedical Ward RequirementsZymer Lee AbasoloNo ratings yet
- Physicalexam Score SheetDocument2 pagesPhysicalexam Score SheetMarieCrisNo ratings yet
- Heath Assessment ToolDocument8 pagesHeath Assessment ToolHouda Hayek100% (1)
- Nursing Care Plan 1Document20 pagesNursing Care Plan 1Mary Beth Smyrl Stalnaker100% (1)
- OB Patho Assessment Tool EditedDocument6 pagesOB Patho Assessment Tool EditedDarren RobertoNo ratings yet
- Physical Assessment ChecklistDocument3 pagesPhysical Assessment ChecklistEm NagalNo ratings yet
- Home Health Solutions Group Home Companion Services: Nursing Assessment Form - RecertificationDocument5 pagesHome Health Solutions Group Home Companion Services: Nursing Assessment Form - RecertificationCitra Puspita SariNo ratings yet
- S Satisfactory, US Unsatisfactory, ND Not Done: Slu Clinical Skills Assessment Physical Examination ChecklistDocument3 pagesS Satisfactory, US Unsatisfactory, ND Not Done: Slu Clinical Skills Assessment Physical Examination ChecklistJeffrey RamosNo ratings yet
- Physical Assessment ChecklistDocument3 pagesPhysical Assessment ChecklistMaria PunoNo ratings yet
- Cagayan de Oro City College of Nursing Assessment FormDocument12 pagesCagayan de Oro City College of Nursing Assessment Formsticdo_nursing2011No ratings yet
- Floating or Superficial Pulse: Located in the ExteriorDocument7 pagesFloating or Superficial Pulse: Located in the ExteriorIssaiah Nicolle CeciliaNo ratings yet
- Health AssessmentDocument12 pagesHealth Assessmentjmzxmdy597No ratings yet
- SCAN Davao Responder Accident DetailsDocument1 pageSCAN Davao Responder Accident DetailsIts BorabogNo ratings yet
- History TakingDocument6 pagesHistory Takingdharti daveNo ratings yet
- 11 Trauma Emergency Form 19102023Document2 pages11 Trauma Emergency Form 19102023Marjorie BricenioNo ratings yet
- LRDR Forms PDFDocument17 pagesLRDR Forms PDFnursing filesNo ratings yet
- Health Screening and Assessment Form - SampleDocument3 pagesHealth Screening and Assessment Form - SampleRhu1 San Ildefonso100% (1)
- Neonatal Assessmnt Tool PDFDocument2 pagesNeonatal Assessmnt Tool PDFYestin Reece Corpus ArcegaNo ratings yet
- Physical Assessment ChecklistDocument3 pagesPhysical Assessment ChecklistIsang ButaNo ratings yet
- NU 260-Pediatric Assessment FormDocument3 pagesNU 260-Pediatric Assessment FormMarie Holder67% (6)
- Report Sheet - NursingDocument1 pageReport Sheet - NursingMario LemirNo ratings yet
- NURS 481L - Patient Profile DatabaseDocument7 pagesNURS 481L - Patient Profile DatabaseinnocentforeternityNo ratings yet
- Pleural Aspiration Safety Check List and Report: Procedure Checklist and Report Post-Procedure Checklist (Sign Out)Document1 pagePleural Aspiration Safety Check List and Report: Procedure Checklist and Report Post-Procedure Checklist (Sign Out)soniNo ratings yet
- Ischemic Stroke: Tarlac State University College of Science Department of NursingDocument21 pagesIschemic Stroke: Tarlac State University College of Science Department of NursingKrisianne Mae Lorenzo FranciscoNo ratings yet
- Multan College of NursingDocument9 pagesMultan College of NursingM Kamran QadirNo ratings yet
- Health Examination RecordDocument4 pagesHealth Examination Recordmary joy dela cruzNo ratings yet
- P.A. Tool (Case Pres FINAL.)Document23 pagesP.A. Tool (Case Pres FINAL.)Crystal Ann TadiamonNo ratings yet
- Downtime Daily Nursing Assessment & Care Plan: 1 of 5 Date: TimeDocument5 pagesDowntime Daily Nursing Assessment & Care Plan: 1 of 5 Date: TimerupaliNo ratings yet
- Sedation Record: Patient Selection Criteria DateDocument2 pagesSedation Record: Patient Selection Criteria Datenona aryanNo ratings yet
- Commed Template Family Report 2 1Document18 pagesCommed Template Family Report 2 1Ge NavNo ratings yet
- Gordons Functional Health Pattern Assessment Tool (Bano, R.)Document3 pagesGordons Functional Health Pattern Assessment Tool (Bano, R.)ojay880% (1)
- Live @,upbringing, Schooling, Marriage: When:, S/O:, Home SituationsDocument5 pagesLive @,upbringing, Schooling, Marriage: When:, S/O:, Home SituationsJoy SalvadorNo ratings yet
- Case Study 3 CVD Bleed HCVD Type 2 DM CICD Stage 5 WorksheetDocument27 pagesCase Study 3 CVD Bleed HCVD Type 2 DM CICD Stage 5 WorksheetJade HemmingsNo ratings yet
- OBSTETRIC ASSESSMENT TOOLDocument5 pagesOBSTETRIC ASSESSMENT TOOLDud AccNo ratings yet
- Flea InfestationDocument2 pagesFlea Infestationasad idreesNo ratings yet
- 2 Gordons GeriaDocument7 pages2 Gordons GeriaAiraa ShaneNo ratings yet
- NR450 Nursing Care Plan for DysphagiaDocument8 pagesNR450 Nursing Care Plan for DysphagiaJ15No ratings yet
- Geriatric Case KitDocument6 pagesGeriatric Case KitMay Chelle ErazoNo ratings yet
- Organizational WorksheetDocument4 pagesOrganizational WorksheetJennifer AprilNo ratings yet
- 1 Match The Vital Signs With The DefinitionsDocument8 pages1 Match The Vital Signs With The DefinitionsTeresa Ines Di ComoNo ratings yet
- Revised Checklist of Physical Examination Results: - Student ExaminerDocument17 pagesRevised Checklist of Physical Examination Results: - Student ExaminerSaj Royam AllivomNo ratings yet
- NURS 225V Principles III Data Collection ToolDocument2 pagesNURS 225V Principles III Data Collection ToolKrisNo ratings yet
- 7.8 Collect Data & Come Up With Plan For Day & Nursing Diagnosis Pre-Conference 8-9 Vitals Then Chart, AM Care, StartDocument2 pages7.8 Collect Data & Come Up With Plan For Day & Nursing Diagnosis Pre-Conference 8-9 Vitals Then Chart, AM Care, StartSade' CovingtonNo ratings yet
- SBAR Change of Shift Report: DoctorDocument2 pagesSBAR Change of Shift Report: DoctorLora100% (1)
- Heart of the Field "Refresher & Nha Certification Quick Notes"From EverandHeart of the Field "Refresher & Nha Certification Quick Notes"No ratings yet
- Mindanao Nurses Energize Patients with Exercise and Play TherapyDocument4 pagesMindanao Nurses Energize Patients with Exercise and Play TherapyBiya MacunteNo ratings yet
- Please Provide The Following Information About YourselfDocument2 pagesPlease Provide The Following Information About YourselfBiya MacunteNo ratings yet
- Compilation OF Psychotherapies: Psychiatric-Mental Health NursingDocument24 pagesCompilation OF Psychotherapies: Psychiatric-Mental Health NursingBiya MacunteNo ratings yet
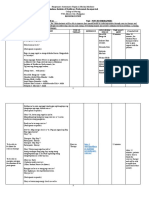
- Specific Objectives Topic/Content Teaching Strategi ES Reference Responsible Person Time Allot-Ment EvaluationDocument11 pagesSpecific Objectives Topic/Content Teaching Strategi ES Reference Responsible Person Time Allot-Ment EvaluationBiya MacunteNo ratings yet
- Pheochromocytoma: PHEO - Dark CHROMO - Color CYT - Cell OMA - TumorDocument3 pagesPheochromocytoma: PHEO - Dark CHROMO - Color CYT - Cell OMA - TumorBiya MacunteNo ratings yet
- DRUG STUDY AmoxicillinDocument1 pageDRUG STUDY Amoxicillinjulesubayubay542886% (14)
- Non Sterile Dressing ChangeDocument2 pagesNon Sterile Dressing ChangePam West0% (1)
- Animals Research DebateDocument2 pagesAnimals Research DebateearlzyNo ratings yet
- The Long and Short of The Issue of Counsellors - The Star OnlineDocument2 pagesThe Long and Short of The Issue of Counsellors - The Star OnlinefareedhashimNo ratings yet
- Essay For The Atlantis ProjectDocument2 pagesEssay For The Atlantis ProjectDaniela BocaNo ratings yet
- Tata Memorial Centre Final Add V 020513Document6 pagesTata Memorial Centre Final Add V 020513Rupal SojitraNo ratings yet
- Investigation and Treatment of Surgical JaundiceDocument38 pagesInvestigation and Treatment of Surgical JaundiceUjas PatelNo ratings yet
- People vs. Ventura, G.R. No. L-15079Document5 pagesPeople vs. Ventura, G.R. No. L-15079Ina Villarica100% (1)
- Dramatically Lower Blood Pressure in Just 17 Days NaturallyDocument29 pagesDramatically Lower Blood Pressure in Just 17 Days NaturallyRamon Alberto Portillo MedinaNo ratings yet
- NCLEX Review Question 101-200Document14 pagesNCLEX Review Question 101-200Felimon BugtongNo ratings yet
- Polycythemia in NeonatesDocument12 pagesPolycythemia in NeonatesjethrochristopherNo ratings yet
- Calabadion A New Agent To Reverse The Effects Of.18Document9 pagesCalabadion A New Agent To Reverse The Effects Of.18Hilton EmilNo ratings yet
- UntitledDocument41 pagesUntitledgladyannNo ratings yet
- AnophthalmiaDocument6 pagesAnophthalmialeny zabidiNo ratings yet
- Cholecystitis - Complications of Cholecystitis A Comprehensive Contemporary Imaging ReviewDocument17 pagesCholecystitis - Complications of Cholecystitis A Comprehensive Contemporary Imaging ReviewSamuel WidjajaNo ratings yet
- PIIS1098301518308854Document1 pagePIIS1098301518308854Angga PratamaNo ratings yet
- Logbook PSM 2021Document103 pagesLogbook PSM 2021Youtube SubNo ratings yet
- Case Report Final Impression Centric Jaw RelationDocument4 pagesCase Report Final Impression Centric Jaw RelationIndri Nurul AiniNo ratings yet
- T1 - Introduction To Health EducationDocument32 pagesT1 - Introduction To Health EducationJake CarvajalNo ratings yet
- Meeting The Evolving Demands of Neurointervention: Implementation and Utilization of Nurse PractitionersDocument5 pagesMeeting The Evolving Demands of Neurointervention: Implementation and Utilization of Nurse PractitionersAANPNo ratings yet
- CDFDocument76 pagesCDFmishra.nagendra7311No ratings yet
- 2019 Afk ProtocolDocument10 pages2019 Afk Protocoldrsunny159840% (1)
- CovocationDocument3 pagesCovocationGauresh NaikNo ratings yet
- Asepsis 1Document52 pagesAsepsis 1严子明 Renz Ryan SevillenoNo ratings yet
- Stilnox 10 MGDocument4 pagesStilnox 10 MGperkinstop2000No ratings yet
- Acute GastroenteritisDocument2 pagesAcute GastroenteritisErika CadawanNo ratings yet
- Anthony J. Destefano, PHD: Growing ThreatsDocument23 pagesAnthony J. Destefano, PHD: Growing Threatstamuno7No ratings yet
- Medicare Initial Preventive Physical Examination Encounter Form ("Welcome To Medicare Physical")Document2 pagesMedicare Initial Preventive Physical Examination Encounter Form ("Welcome To Medicare Physical")B PNo ratings yet
- CV Pack FacDocument53 pagesCV Pack FacdoodrillNo ratings yet