You might also like
- Adrenal and PheochromocytomaDocument86 pagesAdrenal and Pheochromocytomarajan kumar100% (1)
- Fasting-Secrets RevHealthDocument51 pagesFasting-Secrets RevHealthkoponic100% (2)
- Endocrinology Notes for Medical StudentsFrom EverandEndocrinology Notes for Medical StudentsRating: 4 out of 5 stars4/5 (1)
- Disorders of Calcium and Phosphate MetabolismDocument20 pagesDisorders of Calcium and Phosphate MetabolismThirupathi Jakkani100% (1)
- Primal Testosterone: Written by DobrynjaDocument14 pagesPrimal Testosterone: Written by DobrynjaTyler Davis100% (5)
- Endocrine PathologyDocument13 pagesEndocrine Pathologysarguss14100% (1)
- NBME 15 BLOCK 1-4 (No Answers Version)Document203 pagesNBME 15 BLOCK 1-4 (No Answers Version)Monica Li81% (16)
- Acute Liver Failure Group 3Document16 pagesAcute Liver Failure Group 31S VILLEGAS GabrielNo ratings yet
- Dave Feldman's Cholesterol Drop ProtocolDocument4 pagesDave Feldman's Cholesterol Drop ProtocolEvan Martin100% (2)
- Bone Marrow FailureDocument2 pagesBone Marrow FailureGerardLum100% (1)
- PathophysiologyDocument7 pagesPathophysiologyJerica Mae VenoyaNo ratings yet
- CVD Case StudyDocument9 pagesCVD Case StudyMarlon AbadNo ratings yet
- Alzheimer's Disease (Mini Presentation)Document51 pagesAlzheimer's Disease (Mini Presentation)Tiger KneeNo ratings yet
- How To Increase GABA and Balance GlutamateDocument13 pagesHow To Increase GABA and Balance GlutamateAnonymous Puj7S1t100% (3)
- Medical Surgical Nursing Review Notes 30pgsDocument32 pagesMedical Surgical Nursing Review Notes 30pgsNormala Macabuntal SaripadaNo ratings yet
- PheochromocytomaDocument97 pagesPheochromocytomajamestery100% (1)
- PheochromocytomaDocument50 pagesPheochromocytomaPavani Damera100% (2)
- DRUG STUDY AmoxicillinDocument1 pageDRUG STUDY Amoxicillinjulesubayubay542886% (14)
- Character Hypertrophic Scar Keloid: Nutshell Series For FMGE/DNB/NEET-PG-General SurgeryDocument26 pagesCharacter Hypertrophic Scar Keloid: Nutshell Series For FMGE/DNB/NEET-PG-General SurgeryAbdalsalaam AbraikNo ratings yet
- Med-Surg 1Document42 pagesMed-Surg 1Stephen Gabriel Tito100% (1)
- Objectives: Pre-Analytical Considerations in PhlebotomyDocument9 pagesObjectives: Pre-Analytical Considerations in PhlebotomyMr. Potatohead100% (1)
- Medical Surgical Nursing Review NotesDocument78 pagesMedical Surgical Nursing Review NotesLouie ParillaNo ratings yet
- PathophysiologyDocument4 pagesPathophysiologyDante SalesNo ratings yet
- Tumori Mozga (Prof. Stevic) PDFDocument14 pagesTumori Mozga (Prof. Stevic) PDFБогдан ЛажетићNo ratings yet
- PHEOCHROMOCYTOMASDocument5 pagesPHEOCHROMOCYTOMASasaaa1No ratings yet
- Pulmonary Hypertension (PH) Cor Pulmonale (CP) : Professor Miron BOGDAN UMF "Carol Davila" BucurestiDocument63 pagesPulmonary Hypertension (PH) Cor Pulmonale (CP) : Professor Miron BOGDAN UMF "Carol Davila" BucurestiIoana VasileNo ratings yet
- 441 PheochromoDocument48 pages441 Pheochromograyburn_10% (1)
- Physiosynthesis of SCLCDocument4 pagesPhysiosynthesis of SCLCkuro hanabusaNo ratings yet
- Adrenal Tumor-Pheochromocytoma 10-10-19Document30 pagesAdrenal Tumor-Pheochromocytoma 10-10-19JessicaNo ratings yet
- NCMB 316 Lec Midterm 1Document14 pagesNCMB 316 Lec Midterm 1zh4hft6pnzNo ratings yet
- B17M4L4B PheochromocytomaDocument6 pagesB17M4L4B PheochromocytomaJoaquim RodriguezNo ratings yet
- Examinations of Endocrine DisordersDocument72 pagesExaminations of Endocrine Disorderskyle otedaNo ratings yet
- Examinations of Endocrine Disorders: Dr. Pavel MarunaDocument74 pagesExaminations of Endocrine Disorders: Dr. Pavel MarunaJavier SaadNo ratings yet
- PHEOCHROMOCYTOMADocument37 pagesPHEOCHROMOCYTOMAYosi OktarinaNo ratings yet
- PheochromocytomaDocument6 pagesPheochromocytomaVenkatesh Tammineni100% (1)
- PheochromocytomaDocument50 pagesPheochromocytomaashishpandeygNo ratings yet
- Patologi Endokrin 2016Document132 pagesPatologi Endokrin 2016agusNo ratings yet
- Deepika HasdaDocument30 pagesDeepika HasdaDeepika HasdaNo ratings yet
- Disorders of Adrenal Medulla OLUSAYODocument33 pagesDisorders of Adrenal Medulla OLUSAYOIiiNo ratings yet
- Neurology: - Neuron: Nerve, Logos: Knowledge - Neurology: Deals With The Prevention, Therapy andDocument49 pagesNeurology: - Neuron: Nerve, Logos: Knowledge - Neurology: Deals With The Prevention, Therapy andis kimNo ratings yet
- A695 PDFDocument9 pagesA695 PDFFauzi NoviaNo ratings yet
- ENDOCRINOLOGYDocument28 pagesENDOCRINOLOGYjsreyes.402No ratings yet
- Week 17Document13 pagesWeek 17jmmacar19No ratings yet
- Pheochromocytoma: Dr. Suvyl Rodricks Dr. Meera KharbandaDocument74 pagesPheochromocytoma: Dr. Suvyl Rodricks Dr. Meera KharbandaRichgirl DayawonNo ratings yet
- Brain Tumor.Document19 pagesBrain Tumor.Mission JupiterNo ratings yet
- ALSANGEDY BULLETS FOR PACES ChoreaDocument2 pagesALSANGEDY BULLETS FOR PACES ChoreasohailsuNo ratings yet
- Cell Injury - Part 1Document58 pagesCell Injury - Part 1Mirleyka GonzálezNo ratings yet
- PATH 1 ALL Lectures Final1Document2,054 pagesPATH 1 ALL Lectures Final1Andleeb ImranNo ratings yet
- Endocrine GM Eng 2020Document32 pagesEndocrine GM Eng 2020snowrose2609No ratings yet
- Introduction To Psychology (Psych 10) Professor Keith HolyoakDocument60 pagesIntroduction To Psychology (Psych 10) Professor Keith HolyoakRosalind W. WongNo ratings yet
- Patogenesis DepresiDocument14 pagesPatogenesis DepresiNikoFebriRyandoNo ratings yet
- Drug Study 1Document9 pagesDrug Study 1Claire Louise PeñaNo ratings yet
- UntitledDocument2 pagesUntitledVin TagenNo ratings yet
- Respiratory 03 - Bronchiogenic CA: 1) Smoking/industrial Hazards/air Pollution 2) Molecular Genetic MutationDocument2 pagesRespiratory 03 - Bronchiogenic CA: 1) Smoking/industrial Hazards/air Pollution 2) Molecular Genetic Mutationkamil malikNo ratings yet
- Presentation Ectopic HormonesDocument12 pagesPresentation Ectopic HormonesCritic CrazzyNo ratings yet
- Shock in Covid PatientDocument21 pagesShock in Covid PatientGHALEB A. AlmekhlafiNo ratings yet
- Movement Disorders EmergenciesDocument12 pagesMovement Disorders EmergenciesAnonymous QLadTClydkNo ratings yet
- Men's HealthDocument6 pagesMen's HealthkellyjackykjNo ratings yet
- Pathophysiology Plueral Effusion Secondary To Pneumonia: GreenDocument7 pagesPathophysiology Plueral Effusion Secondary To Pneumonia: Greenkuro hanabusaNo ratings yet
- DocumentDocument4 pagesDocumentALi AL-kwafiNo ratings yet
- Delayed Recovery - RamDocument48 pagesDelayed Recovery - RamRaam NaikNo ratings yet
- N505 NSG Care Plan Template F19Document13 pagesN505 NSG Care Plan Template F19Gelsey Gelsinator JianNo ratings yet
- HypertensionDocument10 pagesHypertensionSalman MajidNo ratings yet
- Unconscious and Comatose Patients DR Moses KazevuDocument17 pagesUnconscious and Comatose Patients DR Moses KazevuMoses Jr KazevuNo ratings yet
- Pitutary HeadDocument26 pagesPitutary Headdevutty 123No ratings yet
- Adrenal Function: T. Creighton Mitchell, A. Wayne MeikleDocument19 pagesAdrenal Function: T. Creighton Mitchell, A. Wayne MeikleWho KnowsNo ratings yet
- Nomad:Endocrine Physiology IntroductionDocument40 pagesNomad:Endocrine Physiology IntroductionDr.M.Anthony David100% (11)
- Pathophysiology of CushingDocument3 pagesPathophysiology of CushingAj MacotoNo ratings yet
- Clinical Autonomic and Mitochondrial Disorders: Diagnosis, Prevention, and Treatment for Mind-Body WellnessFrom EverandClinical Autonomic and Mitochondrial Disorders: Diagnosis, Prevention, and Treatment for Mind-Body WellnessNo ratings yet
- Iii. Physical Assessment and Review of SystemDocument7 pagesIii. Physical Assessment and Review of SystemBiya MacunteNo ratings yet
- Please Provide The Following Information About YourselfDocument2 pagesPlease Provide The Following Information About YourselfBiya MacunteNo ratings yet
- Specific Objectives Topic/Content Type of Therapy Reference Responsible Person Time Allot-Ment EvaluationDocument4 pagesSpecific Objectives Topic/Content Type of Therapy Reference Responsible Person Time Allot-Ment EvaluationBiya MacunteNo ratings yet
- Compilation OF Psychotherapies: Psychiatric-Mental Health NursingDocument24 pagesCompilation OF Psychotherapies: Psychiatric-Mental Health NursingBiya MacunteNo ratings yet
- Specific Objectives Topic/Content Teaching Strategi ES Reference Responsible Person Time Allot-Ment EvaluationDocument11 pagesSpecific Objectives Topic/Content Teaching Strategi ES Reference Responsible Person Time Allot-Ment EvaluationBiya MacunteNo ratings yet
- 03.cleveland Clinic of Pediatrics - Selected Questions PDFDocument17 pages03.cleveland Clinic of Pediatrics - Selected Questions PDFLakshaya SinghNo ratings yet
- Hypothyroidism Concept MapDocument1 pageHypothyroidism Concept Mapel shilohNo ratings yet
- What Is Perspiration?: Antiperspirant & DeodorantDocument9 pagesWhat Is Perspiration?: Antiperspirant & DeodorantMd. Abu Bakar Siddique TayefNo ratings yet
- Course Task #3: AnswerDocument5 pagesCourse Task #3: AnswerAria100% (3)
- Yogurt: The Product and Its Manufacture: December 2016Document10 pagesYogurt: The Product and Its Manufacture: December 2016MiqdadNo ratings yet
- Approach To ProteinuriaDocument14 pagesApproach To ProteinuriaRishi ShresthaNo ratings yet
- Articulo 2Document6 pagesArticulo 2Alexander RuizNo ratings yet
- HomeostasisDocument16 pagesHomeostasisNurfatiha RozlanNo ratings yet
- Biochemistry Week 8 - LipidsDocument7 pagesBiochemistry Week 8 - LipidsMicah JadeNo ratings yet
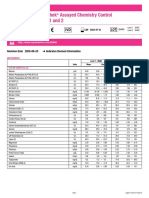
- Lyphochek Assayed Chemistry Control Levels 1 and 2: Revision Date 2020-06-25 Indicates Revised InformationDocument2 pagesLyphochek Assayed Chemistry Control Levels 1 and 2: Revision Date 2020-06-25 Indicates Revised InformationSivaNo ratings yet
- Menorrhagia (Heavy Menstrual Bleeding)Document55 pagesMenorrhagia (Heavy Menstrual Bleeding)Aizi DwimeilaNo ratings yet
- Ketogenic Diets For Treatment of EpilepsyDocument14 pagesKetogenic Diets For Treatment of EpilepsyAlejorNo ratings yet
- Outline: Prepared by Andrea D. LeonardDocument57 pagesOutline: Prepared by Andrea D. LeonardGion LuisNo ratings yet
- Human Physiology & Bio-ChemistryDocument22 pagesHuman Physiology & Bio-ChemistryPranav PawarNo ratings yet
- WLP Science q2 w3 Nov 28 Dec 2Document6 pagesWLP Science q2 w3 Nov 28 Dec 2Maria Aurea BorjaNo ratings yet
- ACE Inhibitors - HFDocument1 pageACE Inhibitors - HFMartha TreviñoNo ratings yet
- Theory PKCSMDocument8 pagesTheory PKCSMrabiatulNo ratings yet
- Appes Abstracts: Oral PresentationsDocument146 pagesAppes Abstracts: Oral PresentationsstoneNo ratings yet
- Hegde SS - Identification of Bone-Specific Alkaline Phosphatase in Saliva and Its Correlation With Skeletal Age.Document5 pagesHegde SS - Identification of Bone-Specific Alkaline Phosphatase in Saliva and Its Correlation With Skeletal Age.ShwethaNo ratings yet
- Growth and Reproduction Hormones of Ruminants Subjected To Heat StressDocument6 pagesGrowth and Reproduction Hormones of Ruminants Subjected To Heat StressEmia BarusNo ratings yet
- SEMI Final Coverage Fundamentals of NursingDocument14 pagesSEMI Final Coverage Fundamentals of NursingGlory NeriNo ratings yet