You might also like
- Lyle Mcdonald - The Ketogenic Diet PDFDocument323 pagesLyle Mcdonald - The Ketogenic Diet PDFJohnny Ice100% (5)
- The Ketogenic Diet: A Detailed Beginner's GuideDocument20 pagesThe Ketogenic Diet: A Detailed Beginner's GuideSarthak Mishra100% (1)
- A Reversing Fatty LiverDocument12 pagesA Reversing Fatty LiverDaz100% (1)
- TOPNOTCH Ob-Gyne Supplement Handout by Joan Cabanting and Nina Banzuela - UPDATED DECEMBER 2017 PDFDocument27 pagesTOPNOTCH Ob-Gyne Supplement Handout by Joan Cabanting and Nina Banzuela - UPDATED DECEMBER 2017 PDFWaiwit KritayakiranaNo ratings yet
- Understand Acid-Base DisordersDocument89 pagesUnderstand Acid-Base DisordersEdouinaNo ratings yet
- The Dates and Lemon Detox Protocol Sheet Official V-1.2Document20 pagesThe Dates and Lemon Detox Protocol Sheet Official V-1.2Shaun Oneill100% (1)
- The Ketogenic Diet: A Comprehensive Overview of Its History, Mechanisms, Applications and Safety ConsiderationsDocument33 pagesThe Ketogenic Diet: A Comprehensive Overview of Its History, Mechanisms, Applications and Safety ConsiderationsAyat RajpootNo ratings yet
- Anatomy Catalogue 2017 PDFDocument4 pagesAnatomy Catalogue 2017 PDFujala singhNo ratings yet
- ABG Answers Sheet - 2Document1 pageABG Answers Sheet - 2khryss100% (1)
- Ebook To A Ketogenic Diet For Weight Loss and Metabolic DiseaseDocument43 pagesEbook To A Ketogenic Diet For Weight Loss and Metabolic Diseasemerlinchabochi100% (1)
- Benefits and Risks of the Ketogenic DietDocument14 pagesBenefits and Risks of the Ketogenic DietMaya Ballout100% (2)
- Clinical ChemistryDocument24 pagesClinical ChemistryQueency Dangilan100% (1)
- Role of Ketogenic Diets in Neurodegenerative DiseasesDocument11 pagesRole of Ketogenic Diets in Neurodegenerative DiseasesAhmed AmerNo ratings yet
- Human Sexuality Unit: Reproductive SystemsDocument38 pagesHuman Sexuality Unit: Reproductive SystemsMary Grace CacalNo ratings yet
- Detailed Ketogenic Diet For EvryoneDocument16 pagesDetailed Ketogenic Diet For EvryoneAmit Raj100% (1)
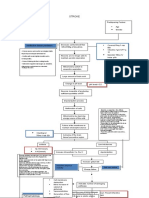
- Concept Map CVADocument1 pageConcept Map CVASuzette Rae Tate100% (2)
- Ketogenic Diets For Weight Loss A Review of Their Principles Safety and EfficacyDocument13 pagesKetogenic Diets For Weight Loss A Review of Their Principles Safety and EfficacyAchmad Yudi100% (1)
- Obesity KetogenicDocument16 pagesObesity KetogenicReza Firsandaya MalikNo ratings yet
- 247 Ketogenic Diet and Its Role in Eliminating PDFDocument14 pages247 Ketogenic Diet and Its Role in Eliminating PDFAnil Batta100% (1)
- Beyond Weight Loss: A Review of The Therapeutic Uses of Very-Low-Carbohydrate (Ketogenic) DietsDocument8 pagesBeyond Weight Loss: A Review of The Therapeutic Uses of Very-Low-Carbohydrate (Ketogenic) DietsChrisostomus AltiusNo ratings yet
- Ketogenic DietDocument60 pagesKetogenic DietKanchi Mitra BhargavNo ratings yet
- Dietabajaencarbohidratos Moreno Capponi 2020Document11 pagesDietabajaencarbohidratos Moreno Capponi 2020PerlaNo ratings yet
- Beyond Weight Loss A Review of The Therapeutic Uses of Very-Low-Carbohydrate (Ketogenic) DietsDocument8 pagesBeyond Weight Loss A Review of The Therapeutic Uses of Very-Low-Carbohydrate (Ketogenic) DietsmrsilvNo ratings yet
- Benefits of Ketogenic Diet For Management of DiabetesDocument4 pagesBenefits of Ketogenic Diet For Management of Diabetescristian david hurtado peñaNo ratings yet
- UntitledDocument12 pagesUntitledKaltsum HafizhahpNo ratings yet
- Ketogenic DietsDocument23 pagesKetogenic DietsNorma Edith López DíazGuerreroNo ratings yet
- Nutrients: Ketogenic Diets and Exercise PerformanceDocument16 pagesNutrients: Ketogenic Diets and Exercise PerformanceBrandon HeatNo ratings yet
- The Impact On Metabolic and Reproductive Diseases of Low-Carbohydrate and Ketogenic DietsDocument10 pagesThe Impact On Metabolic and Reproductive Diseases of Low-Carbohydrate and Ketogenic DietsRonell Ernesto GonzalezNo ratings yet
- 3-Dieta Cetogénica o Baja en CHODocument10 pages3-Dieta Cetogénica o Baja en CHOSol Araceli FischerNo ratings yet
- What is Ketogenic Diet: Diet for Weight Loss: Ketogenic Diet and what comes with it, #1From EverandWhat is Ketogenic Diet: Diet for Weight Loss: Ketogenic Diet and what comes with it, #1No ratings yet
- Nutrients: The Potential Health Benefits of The Ketogenic Diet: A Narrative ReviewDocument29 pagesNutrients: The Potential Health Benefits of The Ketogenic Diet: A Narrative ReviewInez AliNo ratings yet
- KETOsDocument6 pagesKETOsMinal KhanNo ratings yet
- Keto GenicDocument4 pagesKeto GenicRay MunozNo ratings yet
- Untitled DocumentDocument7 pagesUntitled DocumentAbdulRasoolNo ratings yet
- The Ketogenic Diet - A Detailed Beginner's Guide To KetoDocument19 pagesThe Ketogenic Diet - A Detailed Beginner's Guide To Ketoradhika1992No ratings yet
- Long-Term Effects of A Ketogenic Diet in Obese PatientsDocument10 pagesLong-Term Effects of A Ketogenic Diet in Obese Patientsrobertofca2266No ratings yet
- Makalah Pi Pangan Kelompok 3Document4 pagesMakalah Pi Pangan Kelompok 3kristina sipayungNo ratings yet
- Raihah Nabilah Hashim - ENGLISH FOR ACADEMIC WRITING ASSESSMENT 3Document9 pagesRaihah Nabilah Hashim - ENGLISH FOR ACADEMIC WRITING ASSESSMENT 3Raihah Nabilah HashimNo ratings yet
- Original Article The Effect of A Low-Fat, High-Protein or High-Carbohydrate Ad Libitum Diet On Weight Loss Maintenance and Metabolic Risk FactorsDocument9 pagesOriginal Article The Effect of A Low-Fat, High-Protein or High-Carbohydrate Ad Libitum Diet On Weight Loss Maintenance and Metabolic Risk FactorsIyappan SubramaniNo ratings yet
- The Power Of Exogenous Ketones: Learn Their Proven Benefits To Lose Weight And Improve Your Physical / Mental StateFrom EverandThe Power Of Exogenous Ketones: Learn Their Proven Benefits To Lose Weight And Improve Your Physical / Mental StateNo ratings yet
- Paper The Effect of Low Carbohydrate On Energy Metabolism: C Erlanson-Albertsson and J MeiDocument5 pagesPaper The Effect of Low Carbohydrate On Energy Metabolism: C Erlanson-Albertsson and J MeiNalle AguilarNo ratings yet
- Effects of A High-Protein Ketogenic Diet On Hunger, Appetite, and Weight Loss in Obese Men Feeding Ad Libitum-Am J Clin Nutr-2008-Johnstone-44-55Document12 pagesEffects of A High-Protein Ketogenic Diet On Hunger, Appetite, and Weight Loss in Obese Men Feeding Ad Libitum-Am J Clin Nutr-2008-Johnstone-44-55Ivonne BarrazaNo ratings yet
- Keto DietDocument9 pagesKeto DietEttu SobirahNo ratings yet
- Is A Calorie Really A Calorie - Metabolic Advantage of Low-Carbohydrate DietsDocument6 pagesIs A Calorie Really A Calorie - Metabolic Advantage of Low-Carbohydrate DietsGustavo CastroNo ratings yet
- SalmanDocument13 pagesSalmansalman ahmadNo ratings yet
- Ketogenic Diet Guide: Beginner's Guide to Keto Diet BenefitsDocument37 pagesKetogenic Diet Guide: Beginner's Guide to Keto Diet BenefitsVimal KumarNo ratings yet
- Fat Vs Carb RestrictedDocument4 pagesFat Vs Carb RestrictedGiolla HijabNo ratings yet
- Scientific Evidence of Diets For Weight Loss Different Macronutrient... (BITAN ČLANAK)Document11 pagesScientific Evidence of Diets For Weight Loss Different Macronutrient... (BITAN ČLANAK)mirkoNo ratings yet
- Rosenbaum Et Al-2019-ObesityDocument12 pagesRosenbaum Et Al-2019-ObesityaloverofdanceNo ratings yet
- Benefits of Ketogenic DietDocument2 pagesBenefits of Ketogenic DietgiziNo ratings yet
- Advantages and Disadvantages of The Ketogenic Diet: A Review ArticleDocument5 pagesAdvantages and Disadvantages of The Ketogenic Diet: A Review ArticleBEFNo ratings yet
- The Ketogenic Diet For Obesity and Diabetes-Enthusiasm Outpaces EvidenceDocument2 pagesThe Ketogenic Diet For Obesity and Diabetes-Enthusiasm Outpaces EvidenceBrian LeungNo ratings yet
- Impaired Metabolic Flexibility To High-Fat Overfeeding Predicts Future Weight Gain in Healthy AdultsDocument12 pagesImpaired Metabolic Flexibility To High-Fat Overfeeding Predicts Future Weight Gain in Healthy AdultsclemeNo ratings yet
- Screenshot 2023-11-20 at 6.21.49 PMDocument11 pagesScreenshot 2023-11-20 at 6.21.49 PMwaed.mohammad16No ratings yet
- Argumentative Research Paper Final Revised AgainDocument14 pagesArgumentative Research Paper Final Revised Againapi-548755021No ratings yet
- Different Types of Ketogenic Diets: Keto BasicsDocument4 pagesDifferent Types of Ketogenic Diets: Keto BasicsIoana PunctNo ratings yet
- They Help in CholesterolDocument82 pagesThey Help in CholesterolEileen del RosarioNo ratings yet
- The Complete Keto Diet For Beginners: A Practical Approach to Living a Ketogenic LifestyleFrom EverandThe Complete Keto Diet For Beginners: A Practical Approach to Living a Ketogenic LifestyleNo ratings yet
- 10.1007@s11154 019 09514 yDocument12 pages10.1007@s11154 019 09514 ysimonNo ratings yet
- Vantagens+e+desvantagens+da+dieta+cetoge Nica++Document8 pagesVantagens+e+desvantagens+da+dieta+cetoge Nica++Carolina Pereira dos ReisNo ratings yet
- Evidencia Científica de Dietas para Bajar de Peso Diferente Composición de Macronutrientes, Ayuno Intermitente y Dietas PopularesDocument35 pagesEvidencia Científica de Dietas para Bajar de Peso Diferente Composición de Macronutrientes, Ayuno Intermitente y Dietas PopularesCesar Flores ValleNo ratings yet
- Ketogenic Diet Bible: The Ultimate Ketogenic Guide to Feel Energetic, Healthy, and Maximize Weight Loss The Easy WayFrom EverandKetogenic Diet Bible: The Ultimate Ketogenic Guide to Feel Energetic, Healthy, and Maximize Weight Loss The Easy WayNo ratings yet
- The Comprehension To The Keto DietDocument28 pagesThe Comprehension To The Keto DietMishti ChhattaniNo ratings yet
- Is Keto Diet Is Really A ThreatDocument6 pagesIs Keto Diet Is Really A ThreatTanvir AhmedNo ratings yet
- Food Beliefs and Taboos in IslamDocument15 pagesFood Beliefs and Taboos in IslamRaaidah WahabNo ratings yet
- Associations Between Polymorphisms in The and Gene Regions and Habitual Caffeine ConsumptionDocument14 pagesAssociations Between Polymorphisms in The and Gene Regions and Habitual Caffeine ConsumptionRaaidah WahabNo ratings yet
- Mid-Term Assignment: Raaidah WahabDocument14 pagesMid-Term Assignment: Raaidah WahabRaaidah WahabNo ratings yet
- The Mediterranian Diet & Metabolic SyndromeDocument26 pagesThe Mediterranian Diet & Metabolic SyndromeRaaidah WahabNo ratings yet
- SPEED Endocrine e-Dialogues (SEED) Virtual ConferenceDocument7 pagesSPEED Endocrine e-Dialogues (SEED) Virtual ConferenceRajendra ChavanNo ratings yet
- Alcoholism Common and Oxidative Damage Biomarkers 2161 0495.1000 S7 006Document8 pagesAlcoholism Common and Oxidative Damage Biomarkers 2161 0495.1000 S7 006EddafeNo ratings yet
- Early Clinical Exposure (Ece)Document30 pagesEarly Clinical Exposure (Ece)sandeepNo ratings yet
- Journal Pre-Proof: PharmanutritionDocument33 pagesJournal Pre-Proof: PharmanutritionAlonso FernandezNo ratings yet
- Hba1C: A Review of Non-Glycaemic Variables: Leon Campbell, Tessa Pepper, Kate ShipmanDocument8 pagesHba1C: A Review of Non-Glycaemic Variables: Leon Campbell, Tessa Pepper, Kate ShipmanDerison MarsinovaNo ratings yet
- Ezetimibe An Overeview of Analytical Methods For The Drug SubstanceDocument6 pagesEzetimibe An Overeview of Analytical Methods For The Drug SubstanceEditor IJTSRDNo ratings yet
- Non-Alcoholic Fatty Liver Disease (NAFLD) : A Review of Epidemiology, Risk Factors, Diagnosis and ManagementDocument16 pagesNon-Alcoholic Fatty Liver Disease (NAFLD) : A Review of Epidemiology, Risk Factors, Diagnosis and Managementdekatria 2020No ratings yet
- Day 23 Photosynthesis vs. Cellular RespirationDocument22 pagesDay 23 Photosynthesis vs. Cellular RespirationPrincess Rhiane PingkianNo ratings yet
- Tutorial - Metabolism and Fatigue (Student Notes)Document2 pagesTutorial - Metabolism and Fatigue (Student Notes)Ronak SinaeiNo ratings yet
- ApproachpatientpwDocument8 pagesApproachpatientpwPatricia Rearte CarvalhoNo ratings yet
- Physiology of Puberty in Females: A Review: Vasantha SKI and Kona SSRDocument4 pagesPhysiology of Puberty in Females: A Review: Vasantha SKI and Kona SSRWAQAS SHAHIDNo ratings yet
- Galactosemia by Group 9Document41 pagesGalactosemia by Group 9Sree Balaji Srinivas Katakam100% (1)
- Differences in Uric Acid Levels Between Perimenopausal and Menopausal WomenDocument4 pagesDifferences in Uric Acid Levels Between Perimenopausal and Menopausal Womenria kartini panjaitanNo ratings yet
- IsotachophoresisDocument7 pagesIsotachophoresisEka HerlinaNo ratings yet
- SwissADME tool evaluates ADME propertiesDocument8 pagesSwissADME tool evaluates ADME propertiesChai MichelleNo ratings yet
- GROUP-44 RadiographerDocument2 pagesGROUP-44 Radiographeryadav dNo ratings yet
- Hipertiroidismo en GatosDocument20 pagesHipertiroidismo en GatosBrenda GómezNo ratings yet
- Pengaruh Kitosan Cangkang Udang Putih (Penaeus Merguiensis) Terhadap Jumlah Sel Osteoblas Tulang Femur Tikus Wistar Betina Pasca Ovariektomi (The Effect of White Shrimp (Penaeus Merguiensis)Document5 pagesPengaruh Kitosan Cangkang Udang Putih (Penaeus Merguiensis) Terhadap Jumlah Sel Osteoblas Tulang Femur Tikus Wistar Betina Pasca Ovariektomi (The Effect of White Shrimp (Penaeus Merguiensis)fatimah LubisNo ratings yet
- Materi Krisis Tiroid PPDSDocument10 pagesMateri Krisis Tiroid PPDSRudy Arindra WijayaNo ratings yet
- Ovulation and Menstration: Hormone ActionDocument4 pagesOvulation and Menstration: Hormone ActionPaolo QuezonNo ratings yet
- Pharmacards CompilationDocument53 pagesPharmacards CompilationchristianfcualNo ratings yet