You might also like
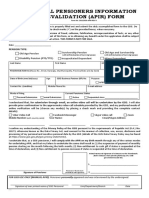
- Annual Pensioners Information Revalidation (APIR) Form: Pension TypeDocument1 pageAnnual Pensioners Information Revalidation (APIR) Form: Pension Typebenjie panlican85% (26)
- SSSForm Retirement ClaimDocument3 pagesSSSForm Retirement ClaimMark JosephNo ratings yet
- Project Report On Sugar IndustryDocument78 pagesProject Report On Sugar IndustryBahubali Khanapure62% (29)
- Forms Pension ResumptionDocument2 pagesForms Pension ResumptionMei Mei100% (1)
- Annexure-SHG/3 Self Help Group - Savings Bank Account Opening FormDocument4 pagesAnnexure-SHG/3 Self Help Group - Savings Bank Account Opening Formkethan kumar100% (1)
- PWD Certificate FormatDocument1 pagePWD Certificate FormatSourav Panda100% (1)
- Annexures 8-10 For PWDDocument5 pagesAnnexures 8-10 For PWDAbhishek TiwariNo ratings yet
- Disability Cert 15042019Document8 pagesDisability Cert 15042019Reshal AhmadNo ratings yet
- Disability Certificate (PWD) Form VI 2022Document2 pagesDisability Certificate (PWD) Form VI 2022blogwriter048No ratings yet
- AbndgjdksvdkkdjDocument4 pagesAbndgjdksvdkkdjEn KayNo ratings yet
- FINAL CAT-III ADVT (2022) Final - 39-42Document4 pagesFINAL CAT-III ADVT (2022) Final - 39-42jackNo ratings yet
- FORM-VI CERTIFICATE OF MULTIPLE DISABILITIESDocument2 pagesFORM-VI CERTIFICATE OF MULTIPLE DISABILITIESMadhu PanchadarlaNo ratings yet
- Certificate of Disability Form-VI PDFDocument3 pagesCertificate of Disability Form-VI PDFpyro_pradeepNo ratings yet
- Disability Certificate Application FormDocument7 pagesDisability Certificate Application FormFacebook Verification TeamNo ratings yet
- Disability Certificate Form - I: Recent PP Size Attested Photograph (Showing Face Only) of The Person With DisabilityDocument6 pagesDisability Certificate Form - I: Recent PP Size Attested Photograph (Showing Face Only) of The Person With DisabilityHemant KumarNo ratings yet
- FORM-PwD (III) Disability Certificate for Multiple DisabilitiesDocument2 pagesFORM-PwD (III) Disability Certificate for Multiple DisabilitiesRoman ReignsNo ratings yet
- Disability Certificate3Document1 pageDisability Certificate3anbarasan1981No ratings yet
- Disability Certificate2Document1 pageDisability Certificate2anbarasan1981No ratings yet
- Disability Certificate1Document1 pageDisability Certificate1anbarasan1981No ratings yet
- Disability CertificateDocument1 pageDisability Certificateanbarasan1981No ratings yet
- Disablity Certificate FormatDocument2 pagesDisablity Certificate FormatSudeshana JainNo ratings yet
- Certificates and FormatsDocument12 pagesCertificates and FormatsAnimesh PriyadarshiNo ratings yet
- EWS PWD OBC Certificate FormatsDocument5 pagesEWS PWD OBC Certificate FormatsbiztigerrNo ratings yet
- Appendix-1 13 PDFDocument1 pageAppendix-1 13 PDFMahesh BhatiyaNo ratings yet
- Application Form Syndicate Bank Temporary Part Time Sweeper PostsDocument2 pagesApplication Form Syndicate Bank Temporary Part Time Sweeper PostsNeha SharmaNo ratings yet
- Certificate of Mental Retardation For Government BenefitsDocument1 pageCertificate of Mental Retardation For Government BenefitsRanjan SahooNo ratings yet
- (Name and Address of The Medical Authority Issuing The Certificate) (See Rule 4)Document2 pages(Name and Address of The Medical Authority Issuing The Certificate) (See Rule 4)Saurav SharmaNo ratings yet
- Application Form Residence Certificate: Applicant DetailsDocument2 pagesApplication Form Residence Certificate: Applicant DetailsJaswant SainiNo ratings yet
- Forms CertificateDocument6 pagesForms CertificateMyheart MDNo ratings yet
- FM GSIS OPS CPR 01 - Pensioners Request Form FillableDocument1 pageFM GSIS OPS CPR 01 - Pensioners Request Form FillableAttorney Rhy Jay100% (2)
- YVOP Form FINALDocument3 pagesYVOP Form FINALJoshua O. ApuyaNo ratings yet
- KYC Gazetted Officer FormatDocument1 pageKYC Gazetted Officer FormatS.p. SainiNo ratings yet
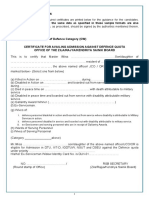
- Certificate For The Persons With DisabilitiesDocument1 pageCertificate For The Persons With DisabilitiesDebajit MalakarNo ratings yet
- Final Cat-III Advt (2022) Final - 35-38Document4 pagesFinal Cat-III Advt (2022) Final - 35-38jackNo ratings yet
- Application For MRI - SRI ClaimDocument2 pagesApplication For MRI - SRI ClaimivyNo ratings yet
- Registration Form Ethics-Oriented Personality Test (EOPT) : For BLGF Officials & EmployeesDocument1 pageRegistration Form Ethics-Oriented Personality Test (EOPT) : For BLGF Officials & EmployeesAttyGalva22No ratings yet
- Annexures - IIIDocument1 pageAnnexures - IIIAadarsh Vivek MitraNo ratings yet
- Ssy Application Form 1 EnglishDocument2 pagesSsy Application Form 1 EnglishSANKAR KUMAR DHARANo ratings yet
- InputForm SeniorCitizen 30sep2015v1.0 PDFDocument2 pagesInputForm SeniorCitizen 30sep2015v1.0 PDFmarivic caroNo ratings yet
- MemoDocument3 pagesMemoDHARMENDRA KHURANANo ratings yet
- FormDocument5 pagesFormSonu MehtaNo ratings yet
- LT Marine Crew ApplicationDocument4 pagesLT Marine Crew ApplicationEirvin JamesNo ratings yet
- Application Form Marriage Certificate: Bride's Details Groom's DetailsDocument6 pagesApplication Form Marriage Certificate: Bride's Details Groom's Detailsshubh9190No ratings yet
- Guarantors Statement FormDocument5 pagesGuarantors Statement FormVeerababu AdapaNo ratings yet
- InputForm Income 24sep2015v3.2Document2 pagesInputForm Income 24sep2015v3.2Mo MomayNo ratings yet
- Annexure A To H 11 12 2019Document4 pagesAnnexure A To H 11 12 2019nishanthk004No ratings yet
- Call Up Letter SCS Bangalore For Nda (Men) 151 CourseDocument13 pagesCall Up Letter SCS Bangalore For Nda (Men) 151 CourseKamalNo ratings yet
- ChecklistDocument3 pagesChecklistnaveen kumarNo ratings yet
- The The of Further To: Extraordinary, 3Document13 pagesThe The of Further To: Extraordinary, 3Vishal KumarNo ratings yet
- Information SheetDocument1 pageInformation SheetVigneshNo ratings yet
- To The Postmaster : For Use of Post OfficeDocument2 pagesTo The Postmaster : For Use of Post OfficeSuvodip EtcNo ratings yet
- Diploma in Laryngology and OtologyDocument2 pagesDiploma in Laryngology and OtologyMuhammad Zaheer Anwar100% (2)
- ASF FINAL Form PDFDocument3 pagesASF FINAL Form PDFAbidNo ratings yet
- FINAL Form PDFDocument3 pagesFINAL Form PDFAbdur Rauf KhanNo ratings yet
- Form4 Provisional MMCDocument3 pagesForm4 Provisional MMCminci sensei100% (2)
- Claimant'S Statement: (Accident Benefit)Document4 pagesClaimant'S Statement: (Accident Benefit)Paolo MagarinNo ratings yet
- Admission: National Institute of Electronics & Information TechnologyDocument3 pagesAdmission: National Institute of Electronics & Information TechnologyUtkarsh AnandNo ratings yet
- FORM6Document2 pagesFORM6SujiNo ratings yet
- Application For Inclusion of Name in Electoral Roll For First Time Voter OR On Shifting From One Constituency To Another ConstituencyDocument14 pagesApplication For Inclusion of Name in Electoral Roll For First Time Voter OR On Shifting From One Constituency To Another ConstituencyASIMNo ratings yet
- Chargeman Rect AdvtDocument7 pagesChargeman Rect AdvtBhiyog YadavNo ratings yet
- CHANDIGARH ADMINISTRATION Job 4Document9 pagesCHANDIGARH ADMINISTRATION Job 4sunny KumarNo ratings yet
- Information Brochure 2023Document5 pagesInformation Brochure 2023sunny KumarNo ratings yet
- A Study On Organisational Culture and Its Impact On Employees Behaviour in Motion Education PVT LTDDocument17 pagesA Study On Organisational Culture and Its Impact On Employees Behaviour in Motion Education PVT LTDDivya Av100% (1)
- Advt 02 2023 Scientific Assistant B Examination Center Details For Shortlisted CandidatesDocument232 pagesAdvt 02 2023 Scientific Assistant B Examination Center Details For Shortlisted Candidatessunny KumarNo ratings yet
- 7 September Evening ShiftDocument52 pages7 September Evening Shiftsunny KumarNo ratings yet
- ListsechemicalDocument1 pageListsechemicalsunny KumarNo ratings yet
- Advt. No. 01 - 2022-FCI Category III ZONE-WISE RECRUITMENT OF NON-EXECUTIVES IN FCIDocument3 pagesAdvt. No. 01 - 2022-FCI Category III ZONE-WISE RECRUITMENT OF NON-EXECUTIVES IN FCIsunny KumarNo ratings yet
- DocumenturgentDocument44 pagesDocumenturgentsunny KumarNo ratings yet
- Army Ordnance Corps Recruitment Admit CardDocument2 pagesArmy Ordnance Corps Recruitment Admit Cardsunny KumarNo ratings yet
- CABS Electra: MODEL: CE-0303EML /CE-0304EMLDocument1 pageCABS Electra: MODEL: CE-0303EML /CE-0304EMLsunny KumarNo ratings yet
- Invites Applications For Short Service Commission Officers For For Various Entries - Jan 2024 (ST 24) CourseDocument2 pagesInvites Applications For Short Service Commission Officers For For Various Entries - Jan 2024 (ST 24) Coursesunny KumarNo ratings yet
- Advt. No. 01 - 2022-Fci Category III Zone-Wise Recruitment of Non-Executives in FciDocument3 pagesAdvt. No. 01 - 2022-Fci Category III Zone-Wise Recruitment of Non-Executives in Fcikiran rajNo ratings yet
- Analysis of Product and Services of Bank of BarodaDocument73 pagesAnalysis of Product and Services of Bank of BarodaJdeeNo ratings yet