You might also like
- Hypertensionaha 119 14057Document10 pagesHypertensionaha 119 14057drewantaNo ratings yet
- Standards and New Drugs in The Treatment of Heart FailureDocument14 pagesStandards and New Drugs in The Treatment of Heart FailureAshutosh SinghNo ratings yet
- ARNI Evidence and Perspectives in Cardiovascular DiseaseDocument12 pagesARNI Evidence and Perspectives in Cardiovascular Diseasefazlur risyad laochiNo ratings yet
- Encarnación MontalvoDocument9 pagesEncarnación MontalvoJhulissa arias cruzNo ratings yet
- Eplerenone and Atrial Fibrillation in Mild Systolic Heart FailureDocument6 pagesEplerenone and Atrial Fibrillation in Mild Systolic Heart FailureJim Dominguez RosalesNo ratings yet
- Dębska-Kozłowska2021 Article WhereAreWeIn2021WithHeartFailuDocument12 pagesDębska-Kozłowska2021 Article WhereAreWeIn2021WithHeartFailuSyifa Mahmud Syukran AkbarNo ratings yet
- Rhythm Control of Atrial Fibrillation in Heart FailureDocument9 pagesRhythm Control of Atrial Fibrillation in Heart FailureUCI CONTINGENCIANo ratings yet
- 4 Pilares de IccDocument10 pages4 Pilares de IccJorge MéndezNo ratings yet
- Reflecting On The Advancements of HFrEF Therapies Over The Last Two Decades and Predicting What Is Yet To ComeDocument8 pagesReflecting On The Advancements of HFrEF Therapies Over The Last Two Decades and Predicting What Is Yet To ComeAnonymous oQtve4oNo ratings yet
- The Role of Neprilysin Inhibitors in Cardiovascular DiseaseDocument6 pagesThe Role of Neprilysin Inhibitors in Cardiovascular DiseaseHarold Mateo Mojica UrregoNo ratings yet
- Medical Therapy of Heart Failure With Reduced Ejection Fraction-A Call For Comparative ResearchDocument7 pagesMedical Therapy of Heart Failure With Reduced Ejection Fraction-A Call For Comparative ResearchNimesh ModiNo ratings yet
- Tratamiento Icc FevpDocument17 pagesTratamiento Icc FevpGuissela Montoya LopezNo ratings yet
- Heart Failure With Reduced Ejection FractionDocument11 pagesHeart Failure With Reduced Ejection Fractionpricilia ardianiNo ratings yet
- Atm 06 23 461Document5 pagesAtm 06 23 461Mohammed shamiul ShahidNo ratings yet
- Progressive Right Ventricular Dysfunction in Patients With Pulmonary Arterial Hypertension Responding To TherapyDocument9 pagesProgressive Right Ventricular Dysfunction in Patients With Pulmonary Arterial Hypertension Responding To TherapyinaNo ratings yet
- Heart Failure With Preserved Ejection FractionDocument19 pagesHeart Failure With Preserved Ejection Fractioncosmin balanNo ratings yet
- Management of Hypertension inDocument12 pagesManagement of Hypertension inaxl___No ratings yet
- Presión Arterial Sistólica en Insuficiencia Cardíaca Con Fracción de Eyección Conservada Tratada Con Sacubitril-ValsartánDocument13 pagesPresión Arterial Sistólica en Insuficiencia Cardíaca Con Fracción de Eyección Conservada Tratada Con Sacubitril-ValsartánBrian Antonio Veramatos LopezNo ratings yet
- Management of Heart Failure With Preserved EjectionFraction A Review PDFDocument13 pagesManagement of Heart Failure With Preserved EjectionFraction A Review PDFGharbi StrongNo ratings yet
- Incidence, Predictors, and Outcome Associations of Dyskalemia in Heart Failure With Preserved, Mid-Range, and Reduced Ejection FractionDocument12 pagesIncidence, Predictors, and Outcome Associations of Dyskalemia in Heart Failure With Preserved, Mid-Range, and Reduced Ejection FractionputriNo ratings yet
- Heart Failure with Normal Ejection FractionDocument19 pagesHeart Failure with Normal Ejection FractionFarhan HasbiNo ratings yet
- Capuano 2015Document5 pagesCapuano 2015bpNo ratings yet
- 1 s2.0 S1936878X17306174 MainDocument9 pages1 s2.0 S1936878X17306174 MainSalma Noor AlmasNo ratings yet
- Aldosterone Antagonists and Outcomes in Real-World Older Patients With Heart Failure and Preserved Ejection FractionDocument8 pagesAldosterone Antagonists and Outcomes in Real-World Older Patients With Heart Failure and Preserved Ejection FractionBryan NguyenNo ratings yet
- Cardiorenal Syndrome: SciencedirectDocument10 pagesCardiorenal Syndrome: SciencedirectDwiFitriaAnggrainiNo ratings yet
- Assessment of Operability of Patients With Pulmonary Arterial Hypertension Associated With Congenital Heart DiseaseDocument8 pagesAssessment of Operability of Patients With Pulmonary Arterial Hypertension Associated With Congenital Heart DiseaseWulan AviantoroNo ratings yet
- The Effect of Cilostazol On Right Heart FunctionDocument43 pagesThe Effect of Cilostazol On Right Heart FunctionGunawan YogaNo ratings yet
- English JournalDocument8 pagesEnglish JournalDebby CinthyaNo ratings yet
- Severe Pulmonary Arterial Hypertension - Stratification of Medical Therapies, Mechanical Support, and Lung TransplantationDocument11 pagesSevere Pulmonary Arterial Hypertension - Stratification of Medical Therapies, Mechanical Support, and Lung Transplantationjose lopeNo ratings yet
- Hyperkalemia_and_Renin-Angiotensin-Aldosterone_SysDocument3 pagesHyperkalemia_and_Renin-Angiotensin-Aldosterone_SysDarwina DawoodNo ratings yet
- Falla Cardiaca Con Fraccion de Eyeccion ConservadaDocument44 pagesFalla Cardiaca Con Fraccion de Eyeccion ConservadaDiego Andrés Mejía VascoNo ratings yet
- Inotrópicos en ICC Avanzada DRUGS 2011 PDFDocument11 pagesInotrópicos en ICC Avanzada DRUGS 2011 PDFCsr ArsNo ratings yet
- Positive Effects of Aggressive Vasodilator Treatment of Well-Treated Essential Hypertensive PatientsDocument7 pagesPositive Effects of Aggressive Vasodilator Treatment of Well-Treated Essential Hypertensive PatientsmuzaqinNo ratings yet
- Heart Failure With Preserved Ejection Fraction (Hfpef) : A Basic and Clinical PerspectiveDocument5 pagesHeart Failure With Preserved Ejection Fraction (Hfpef) : A Basic and Clinical PerspectiveOngky AristianNo ratings yet
- 1414 431X BJMBR 53 7 E9646Document16 pages1414 431X BJMBR 53 7 E9646leidyalexserraoNo ratings yet
- Prevalencia de La Enfermedad Ateroesclerotica Renal JH 2009Document8 pagesPrevalencia de La Enfermedad Ateroesclerotica Renal JH 2009Diego Andrés Mejía VascoNo ratings yet
- Fibrliación Auricular en Falla Cardiaca, Qué Debemos de Hacer ESC 2015Document11 pagesFibrliación Auricular en Falla Cardiaca, Qué Debemos de Hacer ESC 2015alanRV12No ratings yet
- Pre-Capilar, Combinada y Post-Capilar HTP (JACC 2016)Document11 pagesPre-Capilar, Combinada y Post-Capilar HTP (JACC 2016)Claudio Castro TrujilloNo ratings yet
- fcvm-09-876755Document8 pagesfcvm-09-876755Faradiba MaricarNo ratings yet
- Chronic Heart Failure ASHPDocument20 pagesChronic Heart Failure ASHPFaizan Mazhar100% (1)
- Pulmonary Hypertension Associated With Left-Sided Heart DiseaseDocument13 pagesPulmonary Hypertension Associated With Left-Sided Heart DiseaseIvanes IgorNo ratings yet
- ICCFEP, TX Farmacologico No Farmacologico, 2021Document20 pagesICCFEP, TX Farmacologico No Farmacologico, 2021GeovannaHGNo ratings yet
- Heart Failure Management Guide for AnesthesiologistsDocument19 pagesHeart Failure Management Guide for Anesthesiologistsbaiq_permataNo ratings yet
- Managing Patients With Heart Failure: Margaret T. Bowers, DNP, FNP-BCDocument9 pagesManaging Patients With Heart Failure: Margaret T. Bowers, DNP, FNP-BCratiharumNo ratings yet
- Pulmonary Artery Hypertension: A Review of Pathophysiology, Symptoms, and Treatment (PAHDocument21 pagesPulmonary Artery Hypertension: A Review of Pathophysiology, Symptoms, and Treatment (PAHAzizi Abd RahmanNo ratings yet
- Heart Failure: Dr. Andika Sitepu, SPJPDocument48 pagesHeart Failure: Dr. Andika Sitepu, SPJPWi KuNo ratings yet
- 1349-7235-61-0851Document5 pages1349-7235-61-0851Faradiba MaricarNo ratings yet
- AcceptedDocument25 pagesAcceptedANISA RIFKA RIDHONo ratings yet
- JCVTR 11 79Document6 pagesJCVTR 11 79triNo ratings yet
- Pulmonary Hypertension in The Context of Heart Failure With Preserved Ejection FractionDocument15 pagesPulmonary Hypertension in The Context of Heart Failure With Preserved Ejection FractionTom BiusoNo ratings yet
- Dose Response of ACE Inhibitors: Implications of The SECURE TrialDocument5 pagesDose Response of ACE Inhibitors: Implications of The SECURE TrialHeryanti PusparisaNo ratings yet
- Vieillard-Baron2018 Article DiagnosticWorkupEtiologiesAndMDocument17 pagesVieillard-Baron2018 Article DiagnosticWorkupEtiologiesAndMFranciscoNo ratings yet
- Right Heart Failure A Narrative Review For Emergency CliniciansDocument8 pagesRight Heart Failure A Narrative Review For Emergency ClinicianssunhaolanNo ratings yet
- AF KardiomiopatiDocument5 pagesAF KardiomiopatiannisNo ratings yet
- Clinical and Research Considerations For Patients With Hypertensive Acute Heart FailureDocument10 pagesClinical and Research Considerations For Patients With Hypertensive Acute Heart FailureEvediciNo ratings yet
- HyhyDocument8 pagesHyhyAkram KastiranNo ratings yet
- Acute Heart FailureDocument24 pagesAcute Heart FailureTeddy MauriceNo ratings yet
- Algorithm For Therapeutic Management of Acute Heart Failure SyndromesDocument5 pagesAlgorithm For Therapeutic Management of Acute Heart Failure SyndromesaegonblackNo ratings yet
- CardioDocument10 pagesCardiobursy_esNo ratings yet
- 1-s2.0-S001948321500944X-mainDocument7 pages1-s2.0-S001948321500944X-maindrewantaNo ratings yet
- AF Supplementary Data ESC 2020Document38 pagesAF Supplementary Data ESC 2020drewantaNo ratings yet
- CICM First Part Syllabus 2017 - FINAL 10 07 2017Document33 pagesCICM First Part Syllabus 2017 - FINAL 10 07 2017drewantaNo ratings yet
- JurDocument6 pagesJurGus De JanardhanaNo ratings yet
- Nihms 644431Document40 pagesNihms 644431drewantaNo ratings yet
- Circinterventions 119 008530Document12 pagesCircinterventions 119 008530drewantaNo ratings yet
- BARCDocument22 pagesBARCYulian 53No ratings yet
- PIIS091450871930084XDocument7 pagesPIIS091450871930084XdrewantaNo ratings yet
- CHD Know The Facts 2019Document13 pagesCHD Know The Facts 2019drewantaNo ratings yet
- Jaha 120 021765Document13 pagesJaha 120 021765drewantaNo ratings yet
- Cardiac Rehab Improves Physical Capacity and Anxiety After AF AblationDocument10 pagesCardiac Rehab Improves Physical Capacity and Anxiety After AF AblationdrewantaNo ratings yet
- F 1592 CMT Benefits of ACE Inhibitors in Diabetes - PDF 2188Document11 pagesF 1592 CMT Benefits of ACE Inhibitors in Diabetes - PDF 2188haiderNo ratings yet
- Prostethic Valve & PregnancyDocument11 pagesProstethic Valve & PregnancyShienna Marie SalvioNo ratings yet
- Mechanical Prosthetic Valve Thrombus in A Term Pregnant Woman Presenting As Acute Heart Failure: Case Report and Review of LiteratureDocument5 pagesMechanical Prosthetic Valve Thrombus in A Term Pregnant Woman Presenting As Acute Heart Failure: Case Report and Review of LiteraturedrewantaNo ratings yet
- COVID-19 Pandemic Is Associated WithDocument6 pagesCOVID-19 Pandemic Is Associated WithdrewantaNo ratings yet
- A Scoring System To Predict TheDocument8 pagesA Scoring System To Predict ThedrewantaNo ratings yet
- Gomes Neto2019Document11 pagesGomes Neto2019drewantaNo ratings yet
- Adoption of The Transradial Approach For Percutaneous CoronaryDocument7 pagesAdoption of The Transradial Approach For Percutaneous CoronarydrewantaNo ratings yet
- Tascini 2019Document5 pagesTascini 2019drewantaNo ratings yet
- Research Open Access: Dai Et Al. Lipids in Health and Disease (2019) 18:210Document8 pagesResearch Open Access: Dai Et Al. Lipids in Health and Disease (2019) 18:210drewantaNo ratings yet
- 10 1016@j Ijcard 2020 01 010Document6 pages10 1016@j Ijcard 2020 01 010drewantaNo ratings yet
- Association of Preoperative Mixed Venous Oxygen Saturation With Postoperative Segmental Pulmonary Hypertension in Pulmonary Atresia With Ventricular Septal Defect and Major Aortopulmonary CollateralsDocument8 pagesAssociation of Preoperative Mixed Venous Oxygen Saturation With Postoperative Segmental Pulmonary Hypertension in Pulmonary Atresia With Ventricular Septal Defect and Major Aortopulmonary CollateralsdrewantaNo ratings yet
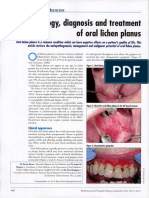
- A e T I o L o G Y, D I A G N o S I S A N D T R e A T M e N T o F o R A L L I C H e N P L A N U SDocument6 pagesA e T I o L o G Y, D I A G N o S I S A N D T R e A T M e N T o F o R A L L I C H e N P L A N U SdrewantaNo ratings yet
- BffsDocument60 pagesBffsdrewantaNo ratings yet
- ECG Diagnosis: Type I Atrial FlutterDocument1 pageECG Diagnosis: Type I Atrial FlutterdrewantaNo ratings yet
- Estimation of At-Risk and Salvaged Myocardium at Myocardial Perfusion SPECT 1 Month After InfarctionDocument8 pagesEstimation of At-Risk and Salvaged Myocardium at Myocardial Perfusion SPECT 1 Month After InfarctiondrewantaNo ratings yet
- Citation 51924507Document1 pageCitation 51924507drewantaNo ratings yet
- Steps To Take After Receiving Offer LetterDocument5 pagesSteps To Take After Receiving Offer LetterNal ChowdhuryNo ratings yet
- Role of Community Health Nurse in Disaster ManagementDocument3 pagesRole of Community Health Nurse in Disaster ManagementyselleamNo ratings yet
- Colibacillosis in Poultry A Disease Overview and TDocument14 pagesColibacillosis in Poultry A Disease Overview and TMonik TanNo ratings yet
- 14th Forum Program Rundown Final v2Document2 pages14th Forum Program Rundown Final v2Ray Li Shing KitNo ratings yet
- CoronarografieDocument72 pagesCoronarografieLaurentiu AndreiNo ratings yet
- Diagnostic and Statistical Manual of Mental DisordersDocument16 pagesDiagnostic and Statistical Manual of Mental DisordersKen MurrayNo ratings yet
- Epidermal Permeability Barrier Defects and Barrier Repair Therapy in Atopic DermatitisDocument12 pagesEpidermal Permeability Barrier Defects and Barrier Repair Therapy in Atopic DermatitisMisaeldpdNo ratings yet
- AAO - External Disease and CorneaDocument19 pagesAAO - External Disease and CorneaJohn Paul VillaflorNo ratings yet
- Liu2011 PDFDocument6 pagesLiu2011 PDFAnonymous cUzAJWocPCNo ratings yet
- Protect Yourself and Others: Get the COVID-19 Vaccine (39Document4 pagesProtect Yourself and Others: Get the COVID-19 Vaccine (39Shane Patrick PanilagNo ratings yet
- Baystate Med CTR Rapid Response Team Recordwith SBARDocument3 pagesBaystate Med CTR Rapid Response Team Recordwith SBARDanishyana DhiwaneoNo ratings yet
- 5.22 Mission Letter To NC AGDocument4 pages5.22 Mission Letter To NC AGMitchell BlackNo ratings yet
- Discuss Thoracic IncisionsDocument47 pagesDiscuss Thoracic IncisionsSucipto HartonoNo ratings yet
- Media Medika IndonesianaDocument8 pagesMedia Medika IndonesianaMuhammad Hamzah AsadullahNo ratings yet
- Memory Reconsolidation Applied - Calm Your Past To Live Your FutureDocument177 pagesMemory Reconsolidation Applied - Calm Your Past To Live Your Futureiskieh100% (7)
- Ent Bhalni AnswerDocument120 pagesEnt Bhalni Answerpatilysh1No ratings yet
- Aluminum Conditioner DX 503Document7 pagesAluminum Conditioner DX 503Mark Evan SalutinNo ratings yet
- Cold Chain Distribution Issues at Indo-Euro PharmaDocument19 pagesCold Chain Distribution Issues at Indo-Euro Pharmaely100% (2)
- SMK Taman Tuanku Jaafar Biology Form 4 Exam 2020Document11 pagesSMK Taman Tuanku Jaafar Biology Form 4 Exam 2020Haslinda SheikhNo ratings yet
- PTB Case-StudyDocument64 pagesPTB Case-StudyBeverly DatuNo ratings yet
- Applications of Calcium and Its Supplement Derived From Marine OrganismsDocument8 pagesApplications of Calcium and Its Supplement Derived From Marine OrganismsDewi SariNo ratings yet
- LILLE FRANCE Trip Report-MajaliwaDocument4 pagesLILLE FRANCE Trip Report-MajaliwaMajaliwa TungarazaNo ratings yet
- A Study On "Corporate Social Responsibility": Bachelor of Business Management (2011-2014)Document65 pagesA Study On "Corporate Social Responsibility": Bachelor of Business Management (2011-2014)MubeenNo ratings yet
- LEAK REPAIR PROGRAMSDocument2 pagesLEAK REPAIR PROGRAMSPradip GuptaNo ratings yet
- Renal MCQ 4Document10 pagesRenal MCQ 4AzizNo ratings yet
- Anatomy and Physiology of Adrenal GlandDocument26 pagesAnatomy and Physiology of Adrenal GlandYAMINIPRIYANNo ratings yet
- Recat Medical BoardDocument5 pagesRecat Medical BoardNavara Naveen kumarNo ratings yet
- Drug Education, Prevention and ControlDocument18 pagesDrug Education, Prevention and ControlMaurene MendozaNo ratings yet
- Mrunal Emotional Intelligence:Meaning, Benefits, Models, Case StudiesDocument8 pagesMrunal Emotional Intelligence:Meaning, Benefits, Models, Case StudiesPrateek BayalNo ratings yet
- Actue Management of Pneumonia in Adults PatienitDocument8 pagesActue Management of Pneumonia in Adults Patienitxiomara torresNo ratings yet