You might also like
- The Role of Neprilysin Inhibitors in Cardiovascular DiseaseDocument6 pagesThe Role of Neprilysin Inhibitors in Cardiovascular DiseaseHarold Mateo Mojica UrregoNo ratings yet
- Heartjnl 2022 321497.fullDocument8 pagesHeartjnl 2022 321497.fullOncología CdsNo ratings yet
- Review of Clinical Studies On Angiotensin II Receptor Blockers and Risk of CancerDocument6 pagesReview of Clinical Studies On Angiotensin II Receptor Blockers and Risk of CancerRisa MuthmainahNo ratings yet
- MS ID HYPE201914057revised OCT 23 2019 Kjeldsen Et AlDocument33 pagesMS ID HYPE201914057revised OCT 23 2019 Kjeldsen Et AldrewantaNo ratings yet
- What Is The Current Best Drug Treatment For Hypertensive Heart Failure With Preserved Ejection Fraction Review of The Totality of EvidenceDocument14 pagesWhat Is The Current Best Drug Treatment For Hypertensive Heart Failure With Preserved Ejection Fraction Review of The Totality of EvidencefbonillaNo ratings yet
- 4 Pilares de IccDocument10 pages4 Pilares de IccJorge MéndezNo ratings yet
- FCVM 10 1263482Document10 pagesFCVM 10 1263482ReywersonNo ratings yet
- Tolvaptan For Volume Management in Heart FailureDocument13 pagesTolvaptan For Volume Management in Heart Failuredhimas satriaNo ratings yet
- JCVTR 11 79Document6 pagesJCVTR 11 79triNo ratings yet
- Ecr 12 1 40Document6 pagesEcr 12 1 40Ahmed MohammedNo ratings yet
- ESC Heart Failure - 2023 - Tang - Cost Utility Analysis of Add On Dapagliflozin in Heart Failure With Preserved or MildlyDocument10 pagesESC Heart Failure - 2023 - Tang - Cost Utility Analysis of Add On Dapagliflozin in Heart Failure With Preserved or MildlyGian CarloNo ratings yet
- Encarnación MontalvoDocument9 pagesEncarnación MontalvoJhulissa arias cruzNo ratings yet
- 361 2012 LaHayeDocument9 pages361 2012 LaHayeOscar PonceNo ratings yet
- Systematic Review and Network Meta-Analysis of Stroke Prevention Treatments in Patients With Atrial FibrillationDocument15 pagesSystematic Review and Network Meta-Analysis of Stroke Prevention Treatments in Patients With Atrial FibrillationAlicePastranaNo ratings yet
- SHIFT AHF TrialDocument7 pagesSHIFT AHF TrialNimesh ModiNo ratings yet
- Ejhf 2206Document10 pagesEjhf 2206Luis Fernando Morales JuradoNo ratings yet
- Addressing Major Unmet Needs in Patients With Systolic Heart Failure: The Role of IvabradineDocument9 pagesAddressing Major Unmet Needs in Patients With Systolic Heart Failure: The Role of IvabradineGhenade ElenaNo ratings yet
- Unanswered Questions During The Live EventDocument9 pagesUnanswered Questions During The Live Eventyash_acharya007No ratings yet
- VHRM 5 1043Document16 pagesVHRM 5 1043AldiKurosakiNo ratings yet
- J Jacbts 2021 10 018Document14 pagesJ Jacbts 2021 10 018Sara AlghamdiNo ratings yet
- Angiotensin Receptor-Neprilysin Inhibition (ARNI) in Heart FailureDocument18 pagesAngiotensin Receptor-Neprilysin Inhibition (ARNI) in Heart FailureJosé DiegoNo ratings yet
- Uji Klinis 5Document10 pagesUji Klinis 5Verliatesya TugasNo ratings yet
- Initiation, Continuation, Switching, and Withdrawal of Heart Failure Medical Therapies During HospitalizationDocument11 pagesInitiation, Continuation, Switching, and Withdrawal of Heart Failure Medical Therapies During HospitalizationAshutosh SinghNo ratings yet
- CKD 7Document3 pagesCKD 7Dimas ReggaeNo ratings yet
- Pharmacological Therapy For Rate and Rhythm Control For Atrial Fibrillation in 2017Document8 pagesPharmacological Therapy For Rate and Rhythm Control For Atrial Fibrillation in 2017UCI CONTINGENCIANo ratings yet
- Medical Tribune October 2014 RGDocument35 pagesMedical Tribune October 2014 RGSiti RohmatillahNo ratings yet
- Standards and New Drugs in The Treatment of Heart FailureDocument14 pagesStandards and New Drugs in The Treatment of Heart FailureAshutosh SinghNo ratings yet
- Management of Heart Failure With Reduced Ejection FractionDocument73 pagesManagement of Heart Failure With Reduced Ejection FractionGurmeet SinghNo ratings yet
- Effect of Beraprost On Pulmonary Hypertension DueDocument6 pagesEffect of Beraprost On Pulmonary Hypertension DueBabebos 95No ratings yet
- Clinical Outcomes Related To Background Diuretic Use and New Diuretic Initiation in Patients With HfrefDocument13 pagesClinical Outcomes Related To Background Diuretic Use and New Diuretic Initiation in Patients With HfrefImaNo ratings yet
- Metoprolol vs. Diltiazem in The Acute Management of Atrial Fibrillation in Patients With Heart Failure With Reduced Ejection FractionDocument5 pagesMetoprolol vs. Diltiazem in The Acute Management of Atrial Fibrillation in Patients With Heart Failure With Reduced Ejection FractionGenevieve LawrenceNo ratings yet
- Ivabradinee UyeDocument8 pagesIvabradinee UyeAzmia TabahNo ratings yet
- 1 s20 S2213177918308576 Main - 230211 - 121322Document9 pages1 s20 S2213177918308576 Main - 230211 - 121322tyaswarantariNo ratings yet
- NEJM 2017 Comentario Braunwald2017Document2 pagesNEJM 2017 Comentario Braunwald2017Francisca Javiera Yáñez VidalNo ratings yet
- Evidence-Based Medical Treatment of Peripheral Arterial Disease: A Rapid ReviewDocument14 pagesEvidence-Based Medical Treatment of Peripheral Arterial Disease: A Rapid ReviewLeo OoNo ratings yet
- Reflecting On The Advancements of HFrEF Therapies Over The Last Two Decades and Predicting What Is Yet To ComeDocument8 pagesReflecting On The Advancements of HFrEF Therapies Over The Last Two Decades and Predicting What Is Yet To ComeAnonymous oQtve4oNo ratings yet
- J Jacc 2022 08 737Document13 pagesJ Jacc 2022 08 737kevin ortegaNo ratings yet
- tmp998 TMPDocument9 pagestmp998 TMPFrontiersNo ratings yet
- Ejhf 2206Document10 pagesEjhf 2206khangha.ptNo ratings yet
- Consenso IccDocument15 pagesConsenso IccMaida Martinez AngelesNo ratings yet
- DVT TreatmentDocument24 pagesDVT TreatmentphoechoexNo ratings yet
- Pi Is 0002934313004427Document1 pagePi Is 0002934313004427Anonymous ghWpCy51ONo ratings yet
- Dębska-Kozłowska2021 Article WhereAreWeIn2021WithHeartFailuDocument12 pagesDębska-Kozłowska2021 Article WhereAreWeIn2021WithHeartFailuSyifa Mahmud Syukran AkbarNo ratings yet
- CVAPreventionAfib PDFDocument11 pagesCVAPreventionAfib PDFAnonymous 3iIYuiwNo ratings yet
- Hearts 03 00012Document8 pagesHearts 03 00012Hayleen GarciaNo ratings yet
- Adherence Tradeoff To Multiple Preventive Therapies and All-Cause Mortality After Acute Myocardial InfarctionDocument12 pagesAdherence Tradeoff To Multiple Preventive Therapies and All-Cause Mortality After Acute Myocardial InfarctionRoberto López MataNo ratings yet
- Heart Failure With Reduced Ejection FractionDocument11 pagesHeart Failure With Reduced Ejection Fractionpricilia ardianiNo ratings yet
- Calcium Channel Blockers and HypertensionDocument10 pagesCalcium Channel Blockers and HypertensionIvan Alquijay MazateNo ratings yet
- 10 1016@j Amjcard 2017 02 037Document7 pages10 1016@j Amjcard 2017 02 037Mila RevalinaNo ratings yet
- DVT and PE Anticoagulation RecommendationsDocument6 pagesDVT and PE Anticoagulation Recommendationsகோகுல் தங்கவேல்No ratings yet
- Medicine: Cardioprotective Effect of Histamine H2 Antagonists in Congestive Heart FailureDocument10 pagesMedicine: Cardioprotective Effect of Histamine H2 Antagonists in Congestive Heart Failureerni pabateNo ratings yet
- Effectiveness and Safety of Direct Oral Anticoagulants in The Secondary Stroke Prevention of Elderly PatientsDocument9 pagesEffectiveness and Safety of Direct Oral Anticoagulants in The Secondary Stroke Prevention of Elderly PatientsLiam HudnikNo ratings yet
- 904 FullDocument7 pages904 FullMohamad MostafaNo ratings yet
- 1 s2.0 S0019483223000433 MainDocument6 pages1 s2.0 S0019483223000433 MainLuluil MunirohNo ratings yet
- British J Pharmacology - 2021 - DignamDocument27 pagesBritish J Pharmacology - 2021 - DignamLinda Silvana SariNo ratings yet
- Betablockers Sitched First LineDocument3 pagesBetablockers Sitched First LineOliverVasconcelosNo ratings yet
- The Future of Cardiovascular BiomedicineDocument16 pagesThe Future of Cardiovascular BiomedicineBryan NguyenNo ratings yet
- ARNI Evidence and Perspectives in Cardiovascular DiseaseDocument12 pagesARNI Evidence and Perspectives in Cardiovascular Diseasefazlur risyad laochiNo ratings yet
- Heart Rate Reduction With Ivabradine and Health Related Quality of Life in Patients With Chronic Heart Failure: Results From The SHIFT StudyDocument10 pagesHeart Rate Reduction With Ivabradine and Health Related Quality of Life in Patients With Chronic Heart Failure: Results From The SHIFT StudyNimesh ModiNo ratings yet
- SHIFT AHF TrialDocument7 pagesSHIFT AHF TrialNimesh ModiNo ratings yet
- Children 08 00322 v2Document16 pagesChildren 08 00322 v2Nimesh ModiNo ratings yet
- Safety and tolerability of bilastine in childrenDocument6 pagesSafety and tolerability of bilastine in childrenNimesh ModiNo ratings yet
- Journal of Drugs in DermatologyDocument10 pagesJournal of Drugs in DermatologyNimesh ModiNo ratings yet
- Clin Transl Allergy (2019)Document7 pagesClin Transl Allergy (2019)Nimesh ModiNo ratings yet
- European Journal of Pediatrics (2020)Document5 pagesEuropean Journal of Pediatrics (2020)Nimesh ModiNo ratings yet
- Journal of Drugs in DermatologyDocument10 pagesJournal of Drugs in DermatologyNimesh ModiNo ratings yet
- Safety and tolerability of bilastine in childrenDocument6 pagesSafety and tolerability of bilastine in childrenNimesh ModiNo ratings yet
- Fesh S A0001171549 1Document7 pagesFesh S A0001171549 1ismuNo ratings yet
- How To Attract Love and Powerful Soul ConnectionsDocument5 pagesHow To Attract Love and Powerful Soul Connectionskinzaali71916No ratings yet
- Entrepreneurship Macro Environment ForcesDocument26 pagesEntrepreneurship Macro Environment ForcesSivaNo ratings yet
- 60d068822a861e19f4179ec9 - 11. Consensus - Local Cerberus - CompressedDocument1 page60d068822a861e19f4179ec9 - 11. Consensus - Local Cerberus - Compressedhombre pocilgaNo ratings yet
- Alaina W - Food Project ReflectionDocument1 pageAlaina W - Food Project Reflectionapi-438601399No ratings yet
- SaponificationDocument2 pagesSaponificationK.SaravananNo ratings yet
- Golden Dawn 2 9 The Moon BreathDocument4 pagesGolden Dawn 2 9 The Moon BreathF_RCNo ratings yet
- Measurement of Level in A Tank Using Capacitive Type Level ProbeDocument13 pagesMeasurement of Level in A Tank Using Capacitive Type Level ProbeChandra Sekar100% (1)
- David Lawrence CVDocument32 pagesDavid Lawrence CVM.Awais AkhterNo ratings yet
- To Begin: MantraDocument9 pagesTo Begin: MantraashissahooNo ratings yet
- Akbh PSK (V), TRBH As Y: AdhimokṣADocument8 pagesAkbh PSK (V), TRBH As Y: AdhimokṣA张晓亮No ratings yet
- Logicroof V-RP enDocument1 pageLogicroof V-RP enCristina DogariNo ratings yet
- Rational Use of AntibioticsDocument35 pagesRational Use of AntibioticsRahul SharmaNo ratings yet
- What Is A Supply ChainDocument20 pagesWhat Is A Supply ChainThanh Binh Tran NguyenNo ratings yet
- Israel Is The MessIahDocument288 pagesIsrael Is The MessIahTeerayoot NoidaNo ratings yet
- Medical Terminology TermsDocument28 pagesMedical Terminology TermsNikka Moreen DagdagNo ratings yet
- Effect of Water Immersion On Mechanical Properties of Polyurethane ...Document8 pagesEffect of Water Immersion On Mechanical Properties of Polyurethane ...konshoeNo ratings yet
- Tugas Bahasa Inggris-1Document8 pagesTugas Bahasa Inggris-1Nur KomariyahNo ratings yet
- Shangqiu Jinpeng Industrial Co., LTD.: Widely Used Waste Rubber Pyrolysis Equipment (XY-7)Document2 pagesShangqiu Jinpeng Industrial Co., LTD.: Widely Used Waste Rubber Pyrolysis Equipment (XY-7)Salma FarooqNo ratings yet
- Labcelldivision ErikagutierrezDocument10 pagesLabcelldivision Erikagutierrezapi-336047220No ratings yet
- Vitamin and Mineral Contents of Gongronema Latifolium LeavesDocument3 pagesVitamin and Mineral Contents of Gongronema Latifolium LeavesFrida Febriani IsnanisafitriNo ratings yet
- Mvf404 Mhn-Seh2000w 956 b4 SiDocument2 pagesMvf404 Mhn-Seh2000w 956 b4 SiluisneiralopezNo ratings yet
- BARACARBDocument2 pagesBARACARBYudha Satria50% (2)
- Flow Forming PresentatiionDocument24 pagesFlow Forming PresentatiionSrinivas Ds100% (1)
- Beneficiation of Cassiterite From Primary Tin OresDocument11 pagesBeneficiation of Cassiterite From Primary Tin OresSULMAGNo ratings yet
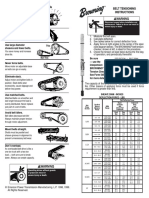
- Browning Belt Tension GaugeDocument2 pagesBrowning Belt Tension GaugeJasperken2xNo ratings yet
- Solitaire Premier - Presentation (Small File)Document18 pagesSolitaire Premier - Presentation (Small File)Shrikant BadheNo ratings yet
- Tcgbutopia G8Document216 pagesTcgbutopia G8faffsNo ratings yet
- B+G+2 Boq - (367-625)Document116 pagesB+G+2 Boq - (367-625)Amy Fitzpatrick100% (3)
- Resume Curt JerromeDocument5 pagesResume Curt JerromeAashish MuraliNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (15)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)