You might also like
- An Overview On Tirzepatide, Dual-Targeted Treatment For Diabetes and ObesityDocument6 pagesAn Overview On Tirzepatide, Dual-Targeted Treatment For Diabetes and ObesityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- NCM 106 Pharmacology Lec 1 and 2Document4 pagesNCM 106 Pharmacology Lec 1 and 2christyl necesitoNo ratings yet
- Nutrition During The Life CycleDocument17 pagesNutrition During The Life CycleAdriel Azhriah BawangNo ratings yet
- Ophthalmic PDFDocument48 pagesOphthalmic PDFMichael Andre CorosNo ratings yet
- The Fetus With Enhanced General Growth or Macrosomia Is Defined by A Birth Weight at or Above The 90th Percentile For Gestational AgeDocument1 pageThe Fetus With Enhanced General Growth or Macrosomia Is Defined by A Birth Weight at or Above The 90th Percentile For Gestational AgeNamRita PrasadNo ratings yet
- Buscopan Drug StudyDocument3 pagesBuscopan Drug StudyMarc BantilanNo ratings yet
- Anna Dabu M.D. University of Western Ontario June 2009Document18 pagesAnna Dabu M.D. University of Western Ontario June 2009Anna DabuNo ratings yet
- Infants and Toddlers FoodDocument4 pagesInfants and Toddlers FoodgersonjimNo ratings yet
- Antenatal Care Guidelines: Doctors of The WorldDocument16 pagesAntenatal Care Guidelines: Doctors of The WorldNadiah FtrNo ratings yet
- Some Issues To Consider While Prescribing Medications For : Pregnant and Lactating PatientsDocument25 pagesSome Issues To Consider While Prescribing Medications For : Pregnant and Lactating PatientsKishor Bajgain100% (1)
- Drug StudyDocument14 pagesDrug StudyAthena Irish LastimosaNo ratings yet
- Drug Study Folic AcidDocument14 pagesDrug Study Folic AcidBianca Marithè Rejano0% (1)
- Prot 9 Galactogogues EnglishDocument5 pagesProt 9 Galactogogues EnglishGary YuenNo ratings yet
- Galactagogues Info SheetDocument6 pagesGalactagogues Info SheetTatiana GutuNo ratings yet
- Bonus - C.P.E - Pregnancy and LactationDocument22 pagesBonus - C.P.E - Pregnancy and Lactationali mohammedNo ratings yet
- Drugs and X-Rays For Pregnant and Breastfeeding Women During Dental TreatmentDocument5 pagesDrugs and X-Rays For Pregnant and Breastfeeding Women During Dental TreatmentArief BudimanNo ratings yet
- Induksi LltasiDocument41 pagesInduksi LltasiDaisy CareNo ratings yet
- Pregnancy and Lactation AnswersDocument8 pagesPregnancy and Lactation AnswersAoiNo ratings yet
- Guideline On Anaesthesia and Sedation in Breastfeeding Women 2020 Guideline From The Association of AnaesthetistsDocument12 pagesGuideline On Anaesthesia and Sedation in Breastfeeding Women 2020 Guideline From The Association of Anaesthetistsantonio123valenciaNo ratings yet
- Herbals and BreastfeedingDocument8 pagesHerbals and BreastfeedingArshad SyahaliNo ratings yet
- Feeding Neonates With Surgical ProblemsDocument14 pagesFeeding Neonates With Surgical ProblemsEcaterina Galagan100% (1)
- Management MastitisDocument6 pagesManagement MastitisReza Hardian NatsirNo ratings yet
- Anaesthesia - 2020 - Mitchell - Guideline On Anaesthesia and Sedation in Breastfeeding Women 2020Document12 pagesAnaesthesia - 2020 - Mitchell - Guideline On Anaesthesia and Sedation in Breastfeeding Women 2020ANGELICANo ratings yet
- Contraceptives NewDocument23 pagesContraceptives NewOdiit StephenNo ratings yet
- Enteral Feeding GuidelinesDocument15 pagesEnteral Feeding GuidelinesAnonymous rDD9I2No ratings yet
- Infant Feeding Mastitis and Breast AbscessDocument8 pagesInfant Feeding Mastitis and Breast AbscessThắng NguyễnNo ratings yet
- Module Obsterics DrugsDocument5 pagesModule Obsterics Drugsjanina mykaNo ratings yet
- Common Problems of Breastfeeding and Weaning - UpToDateDocument40 pagesCommon Problems of Breastfeeding and Weaning - UpToDateWesley LiraniNo ratings yet
- Do Not Copy Penalties Apply: Safety of Topical Dermatologic Medications in PregnancyDocument5 pagesDo Not Copy Penalties Apply: Safety of Topical Dermatologic Medications in Pregnancypipim septianaNo ratings yet
- Network PNguidleines FINALmay 2017Document17 pagesNetwork PNguidleines FINALmay 2017NguyễnĐứcThiệnNo ratings yet
- Algoritmos Gastroenterología PediátricaDocument3 pagesAlgoritmos Gastroenterología PediátricaVMoraNo ratings yet
- Controversies in Breastfeeding: Riccardo DavanzoDocument8 pagesControversies in Breastfeeding: Riccardo DavanzoFarah RkNo ratings yet
- 2015 Article 440Document5 pages2015 Article 440M TarmiziNo ratings yet
- Family Planning Methods Contraceptive Implants: Who Can Use Implantable Contraception?Document5 pagesFamily Planning Methods Contraceptive Implants: Who Can Use Implantable Contraception?Cindy MaslagNo ratings yet
- PregnancyfactsheetDocument2 pagesPregnancyfactsheetrekadarkoNo ratings yet
- Patient Information LeafInsertDocument7 pagesPatient Information LeafInsertNousheenNo ratings yet
- NCP - Diabetes Mellitus Prepregnancy/GestationalDocument13 pagesNCP - Diabetes Mellitus Prepregnancy/GestationalClaudine Christophe100% (1)
- FFPRHC Guidance (July 2004) Contraceptive Choices For Breastfeeding WomenDocument9 pagesFFPRHC Guidance (July 2004) Contraceptive Choices For Breastfeeding Womenastuti susantiNo ratings yet
- Balancingtheuseof Medicationswhile Maintainingbreastfeeding: Palika Datta,, Teresa Baker,, Thomas W. HaleDocument16 pagesBalancingtheuseof Medicationswhile Maintainingbreastfeeding: Palika Datta,, Teresa Baker,, Thomas W. HaleNicole Eugenia Retamal CanalesNo ratings yet
- Induction of LaborDocument19 pagesInduction of LaborMomshie Felaih Binasoy Dela CruzNo ratings yet
- Arbour2013 HypoplasiaDocument5 pagesArbour2013 HypoplasiaCarolina GomezNo ratings yet
- ABM Clinical Protocol #15: Analgesia and Anesthesia For The Breastfeeding MotherDocument7 pagesABM Clinical Protocol #15: Analgesia and Anesthesia For The Breastfeeding MotherWida Ratna SariNo ratings yet
- Intended Learning Objectives: Unit 3: Drugs Affecting The Body System Week 1: Reproductive System Cardiovascular SystemDocument27 pagesIntended Learning Objectives: Unit 3: Drugs Affecting The Body System Week 1: Reproductive System Cardiovascular SystemThrecia RotaNo ratings yet
- Gyn AsDocument2 pagesGyn AsJamal kenasaNo ratings yet
- Managing Nausea and Vomiting of PregnancyDocument2 pagesManaging Nausea and Vomiting of PregnancyAnna LiachenkoNo ratings yet
- Meto DompeDocument6 pagesMeto DomperizkaNo ratings yet
- Hyperstimulation Management SBUHB 2022 Final CElisDocument7 pagesHyperstimulation Management SBUHB 2022 Final CElisantidius johnNo ratings yet
- Amanda Henderson, RN, BSN, BS, IBCLDocument12 pagesAmanda Henderson, RN, BSN, BS, IBCLnanik16No ratings yet
- How Long After Taking Plan B Can I Resume BreastfeedingDocument4 pagesHow Long After Taking Plan B Can I Resume Breastfeedingc2s6kh72100% (1)
- Lipincott Answer KeyDocument3 pagesLipincott Answer KeyKelly Queenie AndresNo ratings yet
- Pregnant or Lactating PatientsDocument1 pagePregnant or Lactating PatientsVicentiu PredescuNo ratings yet
- Acog Practice Bulletin Summary: Pregestational Diabetes MellitusDocument3 pagesAcog Practice Bulletin Summary: Pregestational Diabetes MellitusMaría Fernanda Palma AcostaNo ratings yet
- Pregnancy Breast-Feeding and Drugs Used in Dentistry JADA 2...Document14 pagesPregnancy Breast-Feeding and Drugs Used in Dentistry JADA 2...Sam YousryNo ratings yet
- My Sls Breast Complications in PureperiumDocument20 pagesMy Sls Breast Complications in Pureperiummarina_shawky100% (1)
- Pregnancy, Breast-Feeding and Drugs Used in Dentistry: PracticeDocument14 pagesPregnancy, Breast-Feeding and Drugs Used in Dentistry: PracticeIslam FathiNo ratings yet
- 3083 Final JPTCP (562+to+566)Document5 pages3083 Final JPTCP (562+to+566)MegaNo ratings yet
- Tanner StagingDocument42 pagesTanner StagingDivyanshi KomalNo ratings yet
- SjshagavDocument6 pagesSjshagavindah ayu lestariNo ratings yet
- ReflujoDocument11 pagesReflujoERICKA PORTOCARRERONo ratings yet
- Contraception For Women With Medical ProblemsDocument2 pagesContraception For Women With Medical Problemskhawla moukhtariNo ratings yet
- Unit IV Drugs Used in PregnancyDocument32 pagesUnit IV Drugs Used in PregnancySuvinder singh PannuNo ratings yet
- Prostin E2 Vaginal Tablets - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)Document5 pagesProstin E2 Vaginal Tablets - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)NousheenNo ratings yet
- Gamma-Hydroxybutyric Acid: Controlled Drug SubstancesDocument5 pagesGamma-Hydroxybutyric Acid: Controlled Drug SubstancesAngelica Charisse BuliganNo ratings yet
- OtcdrugDocument2 pagesOtcdrugDaffodil PearlNo ratings yet
- Children's Medicines: Bell, Edward ADocument5 pagesChildren's Medicines: Bell, Edward AJonathanNo ratings yet
- Jurnal Acne 2Document11 pagesJurnal Acne 2Sa'adahNo ratings yet
- Day 3Document2 pagesDay 3bhavik poshiyaNo ratings yet
- Azoles As Non-Nucleoside Reverse Transcriptase Inhibitors (Nnrtis) : Mini ReviewDocument6 pagesAzoles As Non-Nucleoside Reverse Transcriptase Inhibitors (Nnrtis) : Mini ReviewvinayNo ratings yet
- Acetaminophen Chart PDFDocument2 pagesAcetaminophen Chart PDFHp SlateNo ratings yet
- I43Be) Utaj 3A Flekot 1.: 3E14PehDocument8 pagesI43Be) Utaj 3A Flekot 1.: 3E14PehSuzana Panova-CvetkovskaNo ratings yet
- Evaluation of Price Disparity Among Generic Medicines in IndiaDocument3 pagesEvaluation of Price Disparity Among Generic Medicines in Indiadada patilNo ratings yet
- ADC 2023 Landscape Review Part 1 The Drug LandscapeDocument16 pagesADC 2023 Landscape Review Part 1 The Drug LandscapeErick CoNo ratings yet
- Epidiolex Legislative Fact Sheet 11-7-18Document2 pagesEpidiolex Legislative Fact Sheet 11-7-18MvrlkrNo ratings yet
- Prinsipal Kode Produk Nama ProdukDocument38 pagesPrinsipal Kode Produk Nama ProdukEko SuhariyadiNo ratings yet
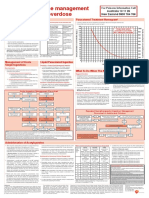
- Paracetamol OD Poster 2016 VersionDocument1 pageParacetamol OD Poster 2016 Versionmuhamed bwamkuuNo ratings yet
- Drugs Affecting PlateletsDocument1 pageDrugs Affecting PlateletsDiana CentaurusNo ratings yet
- Narkotik PsikotropikDocument3 pagesNarkotik PsikotropikThesa HudanaNo ratings yet
- Caroline M. Apovian - Body Weight Considerations in The Management of Type 2 DiabetesDocument15 pagesCaroline M. Apovian - Body Weight Considerations in The Management of Type 2 DiabetesFarid RakhmanNo ratings yet
- Pharmaceutical Market Europe - June 2020Document50 pagesPharmaceutical Market Europe - June 2020Areg GhazaryanNo ratings yet
- Plugin SwcsofrdDocument3 pagesPlugin SwcsofrdUlziisuren NamkhaidavaaNo ratings yet
- PVCR AssessmentDocument19 pagesPVCR AssessmentNikitha SreeNo ratings yet
- Covid Vaccine Reaserch ProjectDocument10 pagesCovid Vaccine Reaserch ProjectEmily KajlaNo ratings yet
- AmherstDocument9 pagesAmherstJeanNo ratings yet
- Modified Release Per Oral Dosage FormDocument43 pagesModified Release Per Oral Dosage FormNurRohmanNo ratings yet
- Substance: Marquis Mecke Mandelin Folin Froehde LiebermannDocument1 pageSubstance: Marquis Mecke Mandelin Folin Froehde LiebermannJhayNo ratings yet
- CCS Drug Infusions v5.0Document95 pagesCCS Drug Infusions v5.0tynNo ratings yet
- Delta 8 LabDocument1 pageDelta 8 LabcarlosbuiquiNo ratings yet
- Drug Study - CefotaximeDocument5 pagesDrug Study - CefotaximeAngel laurestaNo ratings yet
- Fentanyl Fact Sheet 508c 1Document2 pagesFentanyl Fact Sheet 508c 1api-160935984No ratings yet