You might also like
- UntitledDocument115 pagesUntitledİpek OMURNo ratings yet
- GIT-Pemicu 1: Rachelle Betsy - 405140052Document149 pagesGIT-Pemicu 1: Rachelle Betsy - 405140052Michelle Betsy AliantoNo ratings yet
- Department of Orthodontics and Dentofacial OrthopedicsDocument75 pagesDepartment of Orthodontics and Dentofacial OrthopedicssathyaNo ratings yet
- Anatomy and Physiology of Normal DeglutitionDocument49 pagesAnatomy and Physiology of Normal Deglutitionapi-295418186No ratings yet
- Problem 1 GITDocument177 pagesProblem 1 GITMudita DewiNo ratings yet
- Akash Tongue FinalDocument74 pagesAkash Tongue FinalSuraj kumar GuptaNo ratings yet
- Pemicu 1 GI GraceDocument146 pagesPemicu 1 GI Gracegrace liwantoNo ratings yet
- Pemicu 1 DessyDocument184 pagesPemicu 1 DessyDessy DsyNo ratings yet
- Head and Neck Anatomy Lecture # 5 Muscles of Facial Expression, Soft Palate and PharynxDocument42 pagesHead and Neck Anatomy Lecture # 5 Muscles of Facial Expression, Soft Palate and PharynxKyla MacDougallNo ratings yet
- SwallowingDocument44 pagesSwallowingq4cyfv8t8nNo ratings yet
- Oral CavityDocument20 pagesOral CavityadileidalaaNo ratings yet
- W2-8 Oral Region Lecture PDFDocument69 pagesW2-8 Oral Region Lecture PDFSAHIL AGARWALNo ratings yet
- Anatomy of The Oral CavityDocument56 pagesAnatomy of The Oral CavitySaidu TanimuNo ratings yet
- Tongue and Its MusculatureDocument89 pagesTongue and Its MusculaturedrsanketcNo ratings yet
- Swallowing 47Document48 pagesSwallowing 47Ju Ju WareeratNo ratings yet
- Anatomy 2nd-U-4 Digestive SystemDocument176 pagesAnatomy 2nd-U-4 Digestive Systemsinte beyuNo ratings yet
- TONGUEDocument63 pagesTONGUEAthulya LakshmananNo ratings yet
- TONGUE Seminar by MeDocument84 pagesTONGUE Seminar by MeArpita SankhwarNo ratings yet
- Oral Cavity Hard & Soft Palate: Dr. Bashir Ahmed ShaikhDocument19 pagesOral Cavity Hard & Soft Palate: Dr. Bashir Ahmed ShaikhHamza IqbalNo ratings yet
- Jena Marchese @signature - SpeechDocument5 pagesJena Marchese @signature - SpeechABELIZ DURANT MUNIZNo ratings yet
- Hard & Soft Palate Anatomy and InnervationDocument7 pagesHard & Soft Palate Anatomy and InnervationSahrish IqbalNo ratings yet
- Fernando Oral Cavity AnatomyDocument57 pagesFernando Oral Cavity AnatomyPatNo ratings yet
- Digestive Anatomy of AnimalsDocument336 pagesDigestive Anatomy of AnimalsTatenda MagejaNo ratings yet
- Anatomi Trias Mengisap, Menelan dan BernapasDocument74 pagesAnatomi Trias Mengisap, Menelan dan BernapasAnonymous KrEomRrNo ratings yet
- Dental Physiology: DR - Shawfekar Bte HJ Abdul HamidDocument77 pagesDental Physiology: DR - Shawfekar Bte HJ Abdul HamidplsssssNo ratings yet
- L. 10 The Oral CavityDocument79 pagesL. 10 The Oral CavityAsfoor gake1No ratings yet
- Accessory Organs of The Git - Gross AnatomyDocument172 pagesAccessory Organs of The Git - Gross AnatomyManisha RaoNo ratings yet
- Deglutition by WanidaDocument26 pagesDeglutition by Wanidaericjake_lim@yahoo.comNo ratings yet
- The Oral CavityDocument23 pagesThe Oral CavityHamzaNo ratings yet
- Tongue IDocument25 pagesTongue Igajendra ChoudharyNo ratings yet
- 1 - Dysphagia and StrokeDocument39 pages1 - Dysphagia and StrokeVeggy Septian Ellitha100% (1)
- Tongue IDocument25 pagesTongue IJohn SmithNo ratings yet
- Oral Cavity: Dr. Nino TebidzeDocument16 pagesOral Cavity: Dr. Nino TebidzeAbdimalik AliNo ratings yet
- Optimising Mealtimes Across The Lifespan - Lecture - Week 1 2024 1 Slide Per PageDocument45 pagesOptimising Mealtimes Across The Lifespan - Lecture - Week 1 2024 1 Slide Per Pagemalikmary51No ratings yet
- TongueDocument52 pagesTongueNANDANA BOSENo ratings yet
- Physilogy of Mastication and DeglutitionDocument13 pagesPhysilogy of Mastication and Deglutitiondoctanmay100% (1)
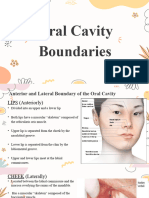
- Oral Cavity BoundariesDocument8 pagesOral Cavity BoundariesLean Edrielle BillonesNo ratings yet
- Digestive System Part 1Document38 pagesDigestive System Part 1mozajamil777No ratings yet
- Lecture PharynxDocument28 pagesLecture PharynxHoor AlnabhaniNo ratings yet
- Digestive System of The FrogDocument73 pagesDigestive System of The FrogNi Ki TaNo ratings yet
- BY Tim Anatomi FKG UPDM (B) DRG Theresia Suhartati PAK DR Andy Hidayat M.Biomed Drg. Pricillia Priska Sianita M.Kes.,Sp - OrtDocument34 pagesBY Tim Anatomi FKG UPDM (B) DRG Theresia Suhartati PAK DR Andy Hidayat M.Biomed Drg. Pricillia Priska Sianita M.Kes.,Sp - OrtFMLNo ratings yet
- MASTICATION, DEGLUTITION AND SPEECH: FUNCTIONS OF THE MASTICATORY SYSTEMDocument79 pagesMASTICATION, DEGLUTITION AND SPEECH: FUNCTIONS OF THE MASTICATORY SYSTEMsiddhi bhojakNo ratings yet
- 3 - Lecture 3 Swallowing BUEDocument30 pages3 - Lecture 3 Swallowing BUEibn.emaraNo ratings yet
- Digestive SystemDocument121 pagesDigestive SystemdearnibNo ratings yet
- Dzuhri Al Okta: 405140187 Pemicu 1 GIDocument29 pagesDzuhri Al Okta: 405140187 Pemicu 1 GIjesslynNo ratings yet
- The Digestive SystemDocument41 pagesThe Digestive Systemkrmgxc8p4fNo ratings yet
- Pemicu 1 GIT Aldi FDocument86 pagesPemicu 1 GIT Aldi Faldi firdausNo ratings yet
- Horizon of Tongue in Orthodontics: Presented by DR - Suvarna GowdaDocument106 pagesHorizon of Tongue in Orthodontics: Presented by DR - Suvarna Gowdasuchitra60% (5)
- Anatomical Landmarks of Mandible: DR Hiba HamidDocument29 pagesAnatomical Landmarks of Mandible: DR Hiba HamidDr.Sathyabhama A.VNo ratings yet
- GIT Anatomy Learning ObjectivesDocument5 pagesGIT Anatomy Learning ObjectivesangrypandasaredangerousNo ratings yet
- Lecture 64: Anatomy of Tongue: Dr. Mohammad Rehan AsadDocument20 pagesLecture 64: Anatomy of Tongue: Dr. Mohammad Rehan AsadRehan Asad0% (1)
- Speech and DeglutiotionDocument55 pagesSpeech and DeglutiotionNilesh B GadiyaNo ratings yet
- Tongue and Its Role in Pros Tho Don TicsDocument100 pagesTongue and Its Role in Pros Tho Don TicsDr Mohit Dhawan100% (18)
- EssaysDocument176 pagesEssaysppdzssx7ghNo ratings yet
- 14-Oral CavityDocument37 pages14-Oral CavitySajid AliNo ratings yet
- Oral CavityDocument65 pagesOral Cavityugwuokeprince4No ratings yet
- A Pediatric Dentist Guide To Orofacial Myology PDFDocument113 pagesA Pediatric Dentist Guide To Orofacial Myology PDFDavid Ochoa Jaramillo100% (2)
- Amirhossein Vaezi MS121 Oral CavityDocument27 pagesAmirhossein Vaezi MS121 Oral Cavityamirhossein vaeziNo ratings yet
- Pemicu BLOK GITDocument74 pagesPemicu BLOK GITNicyela JillienNo ratings yet
- (Medical Radiology) Olle Ekberg, Göran Nylander (Auth.), Olle Ekberg (Eds.) - Dysphagia - Diagnosis and Treatment-Springer-Verlag Berlin Heidelberg (2012)Document604 pages(Medical Radiology) Olle Ekberg, Göran Nylander (Auth.), Olle Ekberg (Eds.) - Dysphagia - Diagnosis and Treatment-Springer-Verlag Berlin Heidelberg (2012)Lucia Nicole Perez HerreraNo ratings yet
- Easy-to-Swallow, Easy-to-Chew PDFDocument259 pagesEasy-to-Swallow, Easy-to-Chew PDFChatterjee Nikita100% (2)
- (Lee Ann C. Golper) Medical Speech-Language Pathol (BookFi) PDFDocument427 pages(Lee Ann C. Golper) Medical Speech-Language Pathol (BookFi) PDFCamila Daza100% (2)
- 2.1 CASANA Parent's GuideDocument43 pages2.1 CASANA Parent's GuideAndreia TavaresNo ratings yet
- Medical FormDocument4 pagesMedical FormSujata DeviNo ratings yet
- Urinary Elimination: Lesson 5eDocument33 pagesUrinary Elimination: Lesson 5eMikhaela Andree MarianoNo ratings yet
- Hormonal Control of Metabolism During ExerciseDocument32 pagesHormonal Control of Metabolism During ExerciseamirNo ratings yet
- Common Gym Equipments: 1. Name: Treadmill DescriptionDocument12 pagesCommon Gym Equipments: 1. Name: Treadmill DescriptiongtNo ratings yet
- Vocabulaire Corps Humain AnglaisDocument2 pagesVocabulaire Corps Humain AnglaisMiguenson AlfredNo ratings yet
- Spinal Cord InjuriesDocument109 pagesSpinal Cord InjuriesGurinder GillNo ratings yet
- Neuro LQ MidtermsDocument47 pagesNeuro LQ MidtermsMariane GumbanNo ratings yet
- Muscles of The BackDocument7 pagesMuscles of The BackDon RaulNo ratings yet
- Marching FundamentalsDocument12 pagesMarching FundamentalsAdhika Nandiwardhana DianastyaNo ratings yet
- Bates Ch 17 Neuro Study GuideDocument11 pagesBates Ch 17 Neuro Study GuidekandeeNo ratings yet
- U.S. Marine Close Combat Fighting Handbo - The United States Marine Corps PDFDocument1,750 pagesU.S. Marine Close Combat Fighting Handbo - The United States Marine Corps PDFJosé Rafael Córdova Rangel100% (3)
- Lumbosacral PlexusDocument41 pagesLumbosacral PlexusJanelle MadayagNo ratings yet
- Postural HygieneDocument10 pagesPostural Hygienethemasterofanaldestruction33No ratings yet
- Development of Occlusion in Primary and Permanent DentitionDocument18 pagesDevelopment of Occlusion in Primary and Permanent DentitionAshis BiswasNo ratings yet
- Throwers Ten Exercise ProgramDocument5 pagesThrowers Ten Exercise ProgramAdmirNo ratings yet
- Mendonca Derick Fronto-Orbital Advancement RevisitedDocument9 pagesMendonca Derick Fronto-Orbital Advancement Revisitedraden chandrajaya listiandokoNo ratings yet
- Basic Anatomy & Physiology Study QuestionsDocument10 pagesBasic Anatomy & Physiology Study QuestionsHema JothyNo ratings yet
- Orlhns Sse Purpose:: Type ADocument8 pagesOrlhns Sse Purpose:: Type AnandhinisankaranNo ratings yet
- SalivaDocument42 pagesSalivaAtharva KambleNo ratings yet
- Case:Volkmann Ischemic Contracture: DR Nrupathunga K KDocument34 pagesCase:Volkmann Ischemic Contracture: DR Nrupathunga K KNish 44No ratings yet
- Occlusion Principles for Partial DenturesDocument12 pagesOcclusion Principles for Partial DenturesEsmail AhmedNo ratings yet
- Prostho Set 1 ADocument15 pagesProstho Set 1 ABinayak UpadhyayaNo ratings yet
- Una Comparación Biomecánica de Diferentes Métodos de Entrenamiento de Bateo de Béisbol.Document11 pagesUna Comparación Biomecánica de Diferentes Métodos de Entrenamiento de Bateo de Béisbol.jhonattan sandovalNo ratings yet
- 2.08 Brachial Region (Arm) - Compartments, Muscles, Nerves, and VesselsDocument3 pages2.08 Brachial Region (Arm) - Compartments, Muscles, Nerves, and VesselsDi CanNo ratings yet
- Rp0807 - Perform Splinting Techniques Learning ObjectivesDocument7 pagesRp0807 - Perform Splinting Techniques Learning ObjectivesMuhammad ZubairNo ratings yet
- Saromm FormDocument5 pagesSaromm FormCharlene KalawNo ratings yet
- Headgear and Its MechanicsDocument10 pagesHeadgear and Its MechanicsDharaniNo ratings yet
- Visual PathwayDocument1 pageVisual PathwayJohn CoxNo ratings yet
- Special Senses Pathway: Visual, Auditory & VestibularDocument56 pagesSpecial Senses Pathway: Visual, Auditory & Vestibularmyka brilliant cristobalNo ratings yet
- Kriya Shareera (Paper-II) (RS4&RS5)Document16 pagesKriya Shareera (Paper-II) (RS4&RS5)Light King ChaudharyNo ratings yet