You might also like
- Management of Orbital FracturesDocument12 pagesManagement of Orbital FracturesMarisol Gallego DuqueNo ratings yet
- Conflict Resolution and Management Module 3 AssignmentDocument7 pagesConflict Resolution and Management Module 3 AssignmentZrii NaturalGreenWellnessNo ratings yet
- Managementofdistal Femurfracturesinadults: An Overview of OptionsDocument12 pagesManagementofdistal Femurfracturesinadults: An Overview of OptionsDoctor's BettaNo ratings yet
- Maxillofacial (Midface) FracturesDocument16 pagesMaxillofacial (Midface) FracturesYeraldin EspañaNo ratings yet
- Broota K D - Experimental Design in Behavioural Research - 3eDocument26 pagesBroota K D - Experimental Design in Behavioural Research - 3eRANJAN ROY67% (3)
- Legislation Register - ExampleDocument10 pagesLegislation Register - ExampleKingsley AhanonuNo ratings yet
- Orthodontic Camouflage in Skeletal Class III Malocclusion A Contemporary ReviewDocument5 pagesOrthodontic Camouflage in Skeletal Class III Malocclusion A Contemporary ReviewNatasha Ank100% (1)
- Probable Airway Etiology For Skeletal Class III Openbite Malocclusion With Posterior CrossbiteCamouflage Treatment With Extractions PDFDocument23 pagesProbable Airway Etiology For Skeletal Class III Openbite Malocclusion With Posterior CrossbiteCamouflage Treatment With Extractions PDFHoàng Đức TháiNo ratings yet
- Controversies in Maxillofacial Trauma PDFDocument9 pagesControversies in Maxillofacial Trauma PDFFabian Camelo OtorrinoNo ratings yet
- PHD Progress Report - FormatDocument3 pagesPHD Progress Report - FormatPraveen ParasarNo ratings yet
- Mindsets&Habits - Tej DosaDocument28 pagesMindsets&Habits - Tej DosaDylan Lopez100% (1)
- The 2 X 4 Appliance McKeown Sandler PDFDocument4 pagesThe 2 X 4 Appliance McKeown Sandler PDFAgia Tessa AndrianiNo ratings yet
- EPC10-11 Contact ListDocument11 pagesEPC10-11 Contact Listkhsaeed50% (2)
- Letters To The Editor: Distraction Osteogenesis For Patients With Severe Idiopathic Condylar ResorptionDocument2 pagesLetters To The Editor: Distraction Osteogenesis For Patients With Severe Idiopathic Condylar ResorptionDominikaSkórkaNo ratings yet
- "Unilateral Subcondylar Fracture Treated by Close Reduction: A CaseDocument3 pages"Unilateral Subcondylar Fracture Treated by Close Reduction: A CaseAlbertine JaneNo ratings yet
- Jurnal BM 4Document4 pagesJurnal BM 4Edward SuputroNo ratings yet
- Facial Asymmetry Due To Condylar Hyperplasia PDFDocument3 pagesFacial Asymmetry Due To Condylar Hyperplasia PDFIndah Hafniar HasibuanNo ratings yet
- Late Treatment of Malunited Mafar Fractures: Clinical ArticlesDocument15 pagesLate Treatment of Malunited Mafar Fractures: Clinical ArticlesnasimNo ratings yet
- Achondroplasia: Orocraniofacial Features and Orthodontic-Surgical Management Guidelines ProposalDocument6 pagesAchondroplasia: Orocraniofacial Features and Orthodontic-Surgical Management Guidelines Proposalchristian roblesNo ratings yet
- MutiLoc Nail Versus Philos Plate inDocument9 pagesMutiLoc Nail Versus Philos Plate inResi de Trauma OrtopediaNo ratings yet
- Management of Sub Condylar Fracture in 15 Yr Old Patient: Case ReportDocument6 pagesManagement of Sub Condylar Fracture in 15 Yr Old Patient: Case ReportIma ShofyaNo ratings yet
- Orbitalfractures: Kris S. Moe,, Andrew H. Murr,, Sara Tullis WesterDocument15 pagesOrbitalfractures: Kris S. Moe,, Andrew H. Murr,, Sara Tullis Westerstoia_sebiNo ratings yet
- Pédiatrie Elbow Trauma: An Orthopaedic Perspective On The Importance of Radiographie InterpretationDocument10 pagesPédiatrie Elbow Trauma: An Orthopaedic Perspective On The Importance of Radiographie InterpretationtripodegrandeNo ratings yet
- Sonego 2014Document6 pagesSonego 2014Isabella WilkeNo ratings yet
- Osteosarcoma CondroblasticoDocument5 pagesOsteosarcoma CondroblasticoFrancis SortoNo ratings yet
- Impact of Virtual Planning On Surgical Reposition of The Premaxilla Using An Endonasal Approach and Simultaneous AlveoloplastyDocument4 pagesImpact of Virtual Planning On Surgical Reposition of The Premaxilla Using An Endonasal Approach and Simultaneous Alveoloplastymirah indrianiNo ratings yet
- Intramedullary Nailing of Pediatric Femoral Shaft FractureDocument10 pagesIntramedullary Nailing of Pediatric Femoral Shaft FractureJayNo ratings yet
- Surgical Outcome of Blowout Fractures of Floor of Orbit A Case Series Of5 Patients 2155 9570 1000518Document5 pagesSurgical Outcome of Blowout Fractures of Floor of Orbit A Case Series Of5 Patients 2155 9570 1000518Luqman HakimNo ratings yet
- Temporo Mandibular Joint AnkylosisDocument5 pagesTemporo Mandibular Joint AnkylosisCah YaniNo ratings yet
- Kasus 1 RKG 5 Euginia YosephineDocument5 pagesKasus 1 RKG 5 Euginia YosephineEuginia YosephineNo ratings yet
- Capsular Contracture and Genetic Profile of Ica.56Document20 pagesCapsular Contracture and Genetic Profile of Ica.56alinutza_childNo ratings yet
- Orthodontic Treatmentafter High Condylectomyin Patientswith Unilateral Condylar HyperplasiaDocument9 pagesOrthodontic Treatmentafter High Condylectomyin Patientswith Unilateral Condylar HyperplasiaOrtodoncia UNAL 2020No ratings yet
- Congenital Isolated Aplasia of Lower Lateral Cartilage and Reconstruction Using Dorsal Hump MaterialDocument3 pagesCongenital Isolated Aplasia of Lower Lateral Cartilage and Reconstruction Using Dorsal Hump MaterialDiego A. Cuadros TorresNo ratings yet
- Reversed ArthroplastyDocument12 pagesReversed ArthroplastyRoger WatersNo ratings yet
- Babhulkar 2017Document11 pagesBabhulkar 2017OyT Velez SarfieldNo ratings yet
- Idiopathic Condylar Resorption: Diagnosis, Treatment Protocol, and OutcomesDocument11 pagesIdiopathic Condylar Resorption: Diagnosis, Treatment Protocol, and OutcomesCatherine NocuaNo ratings yet
- Optimizando La EsteticaDocument19 pagesOptimizando La EsteticaGiovanna ChamonNo ratings yet
- Open Bite 2Document11 pagesOpen Bite 2Hồ TiênNo ratings yet
- Investigation of Free-Flap Transfer Reconstruction in Elderly Patients and Oral Intake FunctionDocument3 pagesInvestigation of Free-Flap Transfer Reconstruction in Elderly Patients and Oral Intake Functioncusom34No ratings yet
- Fratura de Maxila EdentulaDocument4 pagesFratura de Maxila EdentulajosfranNo ratings yet
- Tope Precondileo Como Tratamiento de Luxación CrónicaDocument6 pagesTope Precondileo Como Tratamiento de Luxación CrónicaJose Ramiro Castillo AlemanNo ratings yet
- Sten Quist 2016Document5 pagesSten Quist 2016Fernanda AhumadaNo ratings yet
- Piero Cascone 2017Document6 pagesPiero Cascone 2017João Paulo DutraNo ratings yet
- Nils Worsaae1994Document8 pagesNils Worsaae1994João Paulo DutraNo ratings yet
- Branchial Arch SyndromesDocument7 pagesBranchial Arch SyndromesVita Dental PachucaNo ratings yet
- Reconstruction of Mandible by Free Fibular Flap: Original ArticleDocument5 pagesReconstruction of Mandible by Free Fibular Flap: Original ArticleSani Solihatul FitriNo ratings yet
- Preseptal Transconjunctival Approach in Orbital Rim FractureDocument4 pagesPreseptal Transconjunctival Approach in Orbital Rim FracturevonnyNo ratings yet
- Intraoral Distraction Osteogenesis To Lengthen The Ascending Ramus. Experience With Seven Patients Jansma Bierman BeckingDocument6 pagesIntraoral Distraction Osteogenesis To Lengthen The Ascending Ramus. Experience With Seven Patients Jansma Bierman BeckingAdrian StanNo ratings yet
- Vertical Splitting of The Mandibular Body As An Alternative To Inferior Alveolar Nerve LateralizationDocument7 pagesVertical Splitting of The Mandibular Body As An Alternative To Inferior Alveolar Nerve Lateralizationr1comfupchNo ratings yet
- Ask Us : Readers' ForumDocument1 pageAsk Us : Readers' ForumakNo ratings yet
- Malata 2006Document7 pagesMalata 2006Female calmNo ratings yet
- Iwanaga 2017Document5 pagesIwanaga 2017zj7n2rhtb4No ratings yet
- 217 222CicatricialEctropionDocument7 pages217 222CicatricialEctropionRania ENo ratings yet
- Humeral Non UnionDocument12 pagesHumeral Non Unionmmqk122No ratings yet
- Tibial Derotational Osteotomies in Two Neuromuscular PopulationsDocument6 pagesTibial Derotational Osteotomies in Two Neuromuscular PopulationsJuan Agustin Valcarce LeonNo ratings yet
- V M A B D D I P AC R: Ertical Andibular Lveolar ONE Istraction and Ental Mplant Lacement: ASE EportDocument5 pagesV M A B D D I P AC R: Ertical Andibular Lveolar ONE Istraction and Ental Mplant Lacement: ASE EportDr. Jalisson VicenteNo ratings yet
- Maxillofacial Reconstruction 2013Document237 pagesMaxillofacial Reconstruction 2013Mohammed Qasim Al-WataryNo ratings yet
- Wurgaft R, Rappoport K, Soler C, Ponce C, Flores-Mir CDocument16 pagesWurgaft R, Rappoport K, Soler C, Ponce C, Flores-Mir CCatalina Soler LioiNo ratings yet
- New Treatment Modality For Maxillary Hypoplasia in Cleft PatientsDocument9 pagesNew Treatment Modality For Maxillary Hypoplasia in Cleft PatientsKaranPadhaNo ratings yet
- Berlin Et Al (2023) Multidisciplinary Approach For Autotransplantation and Restoration of A Maxillary PremolarDocument7 pagesBerlin Et Al (2023) Multidisciplinary Approach For Autotransplantation and Restoration of A Maxillary PremolarISAI FLORES PÉREZNo ratings yet
- Ghan em 2005Document5 pagesGhan em 2005asfwegereNo ratings yet
- JR Rani GamawatiDocument20 pagesJR Rani GamawatiRani GamawatiNo ratings yet
- 1 s2.0 S1808869422001355 MainDocument1 page1 s2.0 S1808869422001355 MainHussein AhmedNo ratings yet
- Peng 2012Document7 pagesPeng 2012abhishekjha0082No ratings yet
- 1 s2.0 S0901502715013521 MainDocument7 pages1 s2.0 S0901502715013521 MainGabriellaMariaNo ratings yet
- Operative Brachial Plexus Surgery: Clinical Evaluation and Management StrategiesFrom EverandOperative Brachial Plexus Surgery: Clinical Evaluation and Management StrategiesAlexander Y. ShinNo ratings yet
- Office of The Mayor: Republic of The Philippines Province of La Union Municipality of Caba Tel. # (072) 607-03-12Document3 pagesOffice of The Mayor: Republic of The Philippines Province of La Union Municipality of Caba Tel. # (072) 607-03-12Sunshine MaglayaNo ratings yet
- Unisonic Technologies Co., LTD: 9A, 700V N-CHANNEL Power MosfetDocument4 pagesUnisonic Technologies Co., LTD: 9A, 700V N-CHANNEL Power MosfetJoshi Joseph JoyNo ratings yet
- GCSE Mathematics 1MA1 Problem-Solving Questions 1: Higher TierDocument21 pagesGCSE Mathematics 1MA1 Problem-Solving Questions 1: Higher TierMorena PotenzaNo ratings yet
- UNIT 3 - Journal EntryDocument5 pagesUNIT 3 - Journal EntrySOFI ULLISKYNo ratings yet
- Appendix A. Code Generators For BCH CodesDocument28 pagesAppendix A. Code Generators For BCH CodesBereket TarikuNo ratings yet
- Spring 2018 Graduate Course Descriptions - 0Document25 pagesSpring 2018 Graduate Course Descriptions - 0IvanNo ratings yet
- This Is The New TitleDocument7 pagesThis Is The New TitleMUSÑGI MICAELA LEIGH SUZONNo ratings yet
- Shs SLM-CNF Melc5Document26 pagesShs SLM-CNF Melc5Jean RamosNo ratings yet
- Fuel Consumption SpreadsheetDocument63 pagesFuel Consumption SpreadsheetcaptulccNo ratings yet
- The Cement Industry in EthiopiaDocument7 pagesThe Cement Industry in EthiopiaTesfaye Azanie1No ratings yet
- Interpersonal Communication Book 15th Edition Devito Test BankDocument19 pagesInterpersonal Communication Book 15th Edition Devito Test Bankgwynethalvaf2qroa100% (32)
- Iso 3745 2012 en PDFDocument11 pagesIso 3745 2012 en PDFMARIO ALBERTO MANILLA CORDOBANo ratings yet
- Game Art 1A GART5111: Tasks and ICEDocument3 pagesGame Art 1A GART5111: Tasks and ICEKobus LombardNo ratings yet
- Full Report-Oil Skimmer Cum Metal Chip CollectorDocument55 pagesFull Report-Oil Skimmer Cum Metal Chip Collectorrajkumar100% (1)
- BD Solutions PDFDocument31 pagesBD Solutions PDFLoya Yang100% (3)
- Teaching StandardsDocument21 pagesTeaching Standardsapi-557400513No ratings yet
- Lab 06: Arrays & Functions Objective(s) :: ExercisesDocument4 pagesLab 06: Arrays & Functions Objective(s) :: ExercisesAhsan Ali GopangNo ratings yet
- Uganda The National Slum Upgrading Strategy and Action Plan 2008Document62 pagesUganda The National Slum Upgrading Strategy and Action Plan 2008Maiga Ayub HusseinNo ratings yet
- First Periodical Test in Science 7 2022 2023Document4 pagesFirst Periodical Test in Science 7 2022 2023Ma. Elizabeth CusiNo ratings yet
- Springer Reassessing European Impressions of Indian AstronomyDocument7 pagesSpringer Reassessing European Impressions of Indian AstronomyAnkur KakkarNo ratings yet
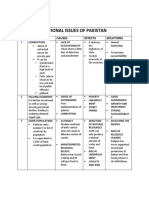
- National and International IssuesDocument5 pagesNational and International IssuesHaroon Karim BalochNo ratings yet
- Umbar - Performance Task 6Document4 pagesUmbar - Performance Task 6Bella CiaoNo ratings yet
- T-Test For Correlated Samples: Sherry V. Mecida, LPT, MATCCDocument6 pagesT-Test For Correlated Samples: Sherry V. Mecida, LPT, MATCCReno PhillipNo ratings yet
- Inventions - Model Inquiry Pedagogy AT1 - Zara BorgDocument27 pagesInventions - Model Inquiry Pedagogy AT1 - Zara BorgZara BorgNo ratings yet