You might also like
- S088954062100442XDocument11 pagesS088954062100442Xleoncio cabrera rojasNo ratings yet
- Jossjoralmaxillofacsurg20106812601269 PDFDocument10 pagesJossjoralmaxillofacsurg20106812601269 PDFSaurabh SatheNo ratings yet
- Skeletal and Dentoalveolar Changes After Miniscrew-Assisted Rapid Palatal Expansion in Young Adults A Cone-Beam Computed Tomography Study.Document11 pagesSkeletal and Dentoalveolar Changes After Miniscrew-Assisted Rapid Palatal Expansion in Young Adults A Cone-Beam Computed Tomography Study.Natan GussNo ratings yet
- Periodontal Plastic Surgery To Improve AestheticsDocument7 pagesPeriodontal Plastic Surgery To Improve AestheticsElizabet KalmykovaNo ratings yet
- Raffaini Bioss CollagenDocument7 pagesRaffaini Bioss CollagenÂngelo Rosso LlantadaNo ratings yet
- CBCT Article DiagnosticsDocument17 pagesCBCT Article DiagnosticsNajla Dar-OdehNo ratings yet
- Ortodoncia 2Document9 pagesOrtodoncia 2soisosoisNo ratings yet
- Jced 9 E1029Document6 pagesJced 9 E1029Ana Gabriela AlbuquerqueNo ratings yet
- JPM 12 00508 PDFDocument9 pagesJPM 12 00508 PDFMans TvNo ratings yet
- Dehiscence and Fenestration in Skeletal Class I, II, and III Malocclusions Assessed With Cone-Beam Computed TomographyDocument8 pagesDehiscence and Fenestration in Skeletal Class I, II, and III Malocclusions Assessed With Cone-Beam Computed TomographysujeetNo ratings yet
- Xác Định Nguyên Nhân Cắn Hở- Cắn SâuDocument8 pagesXác Định Nguyên Nhân Cắn Hở- Cắn Sâutâm nguyễnNo ratings yet
- ThicknessDocument10 pagesThicknessshyama pramodNo ratings yet
- Artigo Bad SplitDocument6 pagesArtigo Bad SplitCarolinaNo ratings yet
- JCM 09 00576Document9 pagesJCM 09 00576GABRIELA MOLANO MEZANo ratings yet
- 2021 Does The Timing of 1-Stage Palatoplasty With Radical Muscle Dissection Effect Long-Term Midface Growth A Single-Center Retrospective AnalysisDocument7 pages2021 Does The Timing of 1-Stage Palatoplasty With Radical Muscle Dissection Effect Long-Term Midface Growth A Single-Center Retrospective AnalysisDimitris RodriguezNo ratings yet
- Coronally Advanced Flap With and Without VerticalDocument13 pagesCoronally Advanced Flap With and Without VerticalLEONARDO ALBERTO CRESPIN ZEPEDANo ratings yet
- Fphys 12 630859Document8 pagesFphys 12 630859Catia Sofia A PNo ratings yet
- Prediction of Implant Loss and Marginal Bone Loss by Analysis of Dental Panoramic RadiographsDocument6 pagesPrediction of Implant Loss and Marginal Bone Loss by Analysis of Dental Panoramic RadiographsMuhammad RidwanNo ratings yet
- 12 2019 Ring VS Tent 2019Document10 pages12 2019 Ring VS Tent 2019feli.riam24No ratings yet
- A Multiple Tooth Tale: A Unique Case Report of 33 OdontomesDocument5 pagesA Multiple Tooth Tale: A Unique Case Report of 33 OdontomesIJAR JOURNALNo ratings yet
- Soft Tissue Cephalometric NormsDocument8 pagesSoft Tissue Cephalometric NormsClaudia Gamboa FerrerNo ratings yet
- Retrieve 4Document8 pagesRetrieve 4dreneanastriNo ratings yet
- Fotos OclusalesDocument6 pagesFotos OclusalesMarco Antonio García LunaNo ratings yet
- Skeletal Effects of Monocortical and Bicortical Mini-Implant Anchorage On Maxillary Expansion Using Cone-Beam Computed Tomography in Young AdultsDocument11 pagesSkeletal Effects of Monocortical and Bicortical Mini-Implant Anchorage On Maxillary Expansion Using Cone-Beam Computed Tomography in Young AdultsmalifaragNo ratings yet
- Changes in Facial Form Relative To Progressive Atrophy of The Edentulous JawsDocument7 pagesChanges in Facial Form Relative To Progressive Atrophy of The Edentulous JawsshraddhaNo ratings yet
- Arraño 2020Document7 pagesArraño 2020Dome CárdenasNo ratings yet
- Artículo OrtopeidiaDocument9 pagesArtículo OrtopeidiaDEICY PATRICIA ORTIZ GUANGANo ratings yet
- Tomographic Evaluation of Infrazygomatic Crest ForDocument7 pagesTomographic Evaluation of Infrazygomatic Crest ForVishal SharmaNo ratings yet
- Alveolar Bone and Epithelial Attachment Status Following Two Different Closed-Eruption Surgical Techniques For Impacted Maxillary Central IncisorsDocument6 pagesAlveolar Bone and Epithelial Attachment Status Following Two Different Closed-Eruption Surgical Techniques For Impacted Maxillary Central IncisorsAndres CoboNo ratings yet
- Drughelp - Care 6.22Document10 pagesDrughelp - Care 6.22Joko RifaiNo ratings yet
- Skeletal Width Changes After Mini-Implant-Assisted Rapid Maxillary Expansion (MARME) in Young AdultsDocument6 pagesSkeletal Width Changes After Mini-Implant-Assisted Rapid Maxillary Expansion (MARME) in Young AdultsRolando Huaman BravoNo ratings yet
- Choi Et Al. - 2014 - Three-Dimensional Evaluation of Maxillary AnteriorDocument8 pagesChoi Et Al. - 2014 - Three-Dimensional Evaluation of Maxillary AnteriorPublicidad Digital CanariaNo ratings yet
- Preservation and Augmentation of Molar Extraction Sites Affected by Severe Bone Defect Due To Advanced Periodontitis A Prospective Clinical TrialDocument12 pagesPreservation and Augmentation of Molar Extraction Sites Affected by Severe Bone Defect Due To Advanced Periodontitis A Prospective Clinical TrialBagis Emre GulNo ratings yet
- Paper 1Document5 pagesPaper 1runit nangaliaNo ratings yet
- A Comparison of Treatment Results of Adult Deep-Bite Cases Treated With Lingual and Labial Fixed AppliancesDocument7 pagesA Comparison of Treatment Results of Adult Deep-Bite Cases Treated With Lingual and Labial Fixed AppliancesScribd AccountNo ratings yet
- Alveolar Bone Changes After Rapid Maxillary Expansion With Tooth-Born Appliances: A Systematic ReviewDocument8 pagesAlveolar Bone Changes After Rapid Maxillary Expansion With Tooth-Born Appliances: A Systematic ReviewBryant Omar Liriano MartínezNo ratings yet
- Buccal ShelfDocument10 pagesBuccal ShelfGarimaa SurekaNo ratings yet
- Case ReportDocument7 pagesCase ReportsintyaNo ratings yet
- Miroperforaciones PDFDocument6 pagesMiroperforaciones PDFceci hdeezNo ratings yet
- Jcedv 3 I 1 P 5Document5 pagesJcedv 3 I 1 P 5ERVINA TYAWARMANNo ratings yet
- Skeletal and Dentoalveolar Changes After Miniscrew-Assisted Rapid Palatal Expansion in Young Adults: A Cone-Beam Computed Tomography StudyDocument10 pagesSkeletal and Dentoalveolar Changes After Miniscrew-Assisted Rapid Palatal Expansion in Young Adults: A Cone-Beam Computed Tomography StudyzaidNo ratings yet
- Alveolar Bone Loss Around Incisors in Surgical Skeletal Class III PatientsDocument7 pagesAlveolar Bone Loss Around Incisors in Surgical Skeletal Class III PatientsFatema SammanyNo ratings yet
- Evaluation of Marginal Alveolar Bone in The Anterior Mandible With Pretreatment and Posttreatment Computed Tomography in Nonextraction PatientsDocument10 pagesEvaluation of Marginal Alveolar Bone in The Anterior Mandible With Pretreatment and Posttreatment Computed Tomography in Nonextraction PatientsSoe San KyawNo ratings yet
- MSE 10.1016@j.ajodo.2016.10.025Document11 pagesMSE 10.1016@j.ajodo.2016.10.025Neycer Catpo NuncevayNo ratings yet
- Three-Dimensional Evaluation of Dentofacial Transverse Widths in Adults With Different Sagittal Facial Patterns PDFDocument10 pagesThree-Dimensional Evaluation of Dentofacial Transverse Widths in Adults With Different Sagittal Facial Patterns PDFSoe San KyawNo ratings yet
- Clin Oral Invest Btcp Type 1 Col ConesDocument10 pagesClin Oral Invest Btcp Type 1 Col ConesPathivada LumbiniNo ratings yet
- Split Technique 3Document13 pagesSplit Technique 3Alejandro RuizNo ratings yet
- Fuhrmann 2002Document6 pagesFuhrmann 2002DentalErNo ratings yet
- Journal Pre-Proof: Oral Surg Oral Med Oral Pathol Oral RadiolDocument23 pagesJournal Pre-Proof: Oral Surg Oral Med Oral Pathol Oral Radiolabhishekjha0082No ratings yet
- Lai 2012Document10 pagesLai 2012ARMADNo ratings yet
- PEMF - IMF Mand. FractureDocument10 pagesPEMF - IMF Mand. FractureMáté TóthNo ratings yet
- Medicina 57 00874Document12 pagesMedicina 57 00874Shweta ShirsatNo ratings yet
- Miner2012parte 1Document8 pagesMiner2012parte 1bricevargas023No ratings yet
- Impaction of Maxillary Canines and Its Effect On The Position of Adjacent Teeth and Canine Development: A Cone-Beam Computed Tomography StudyDocument13 pagesImpaction of Maxillary Canines and Its Effect On The Position of Adjacent Teeth and Canine Development: A Cone-Beam Computed Tomography StudyeltonNo ratings yet
- Jawline Contouring AlfaroDocument5 pagesJawline Contouring AlfaroÂngelo Rosso LlantadaNo ratings yet
- Comparison of Alveolar Bone Loss Around Incisors in Normal Occlusion Samples and Surgical Skeletal Class III PatientsDocument8 pagesComparison of Alveolar Bone Loss Around Incisors in Normal Occlusion Samples and Surgical Skeletal Class III PatientsCindy Cendekiawati AnizarNo ratings yet
- Alhammadi 2019Document9 pagesAlhammadi 2019Dela MedinaNo ratings yet
- Sonneveld 2018Document5 pagesSonneveld 2018James Alexander Toruño GordonNo ratings yet
- 1 s2.0 S0889540622006473 MainDocument12 pages1 s2.0 S0889540622006473 MainRicky WongNo ratings yet
- Peri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentFrom EverandPeri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentNo ratings yet
- Copy Resit APLC MiniAssignmentDocument5 pagesCopy Resit APLC MiniAssignmentChong yaoNo ratings yet
- Sample QuestionsDocument70 pagesSample QuestionsBushra MaryamNo ratings yet
- Geometric Sculpture From 72 PencilsDocument5 pagesGeometric Sculpture From 72 PencilsHugo Iván Gonzalez CruzNo ratings yet
- 1571-1635319494618-Unit 04 Leadership and ManagementDocument48 pages1571-1635319494618-Unit 04 Leadership and ManagementdevindiNo ratings yet
- Sia Mock+Test 1 Csat Updated CompressedDocument216 pagesSia Mock+Test 1 Csat Updated Compressedpooja bhatiNo ratings yet
- Abstract Photo CompositionDocument2 pagesAbstract Photo Compositionapi-260853196No ratings yet
- English Extra Conversation Club International Women's DayDocument2 pagesEnglish Extra Conversation Club International Women's Dayevagloria11No ratings yet
- Managing Post COVID SyndromeDocument4 pagesManaging Post COVID SyndromeReddy VaniNo ratings yet
- Edmonson - Pageantry Overture - AnalysisDocument3 pagesEdmonson - Pageantry Overture - Analysisapi-426112870No ratings yet
- Millennium Separation ReportDocument3 pagesMillennium Separation ReportAlexandra AkeNo ratings yet
- C11 Strategy DevelopmentDocument30 pagesC11 Strategy DevelopmentPARTI KEADILAN RAKYAT NIBONG TEBALNo ratings yet
- Lesson 4Document13 pagesLesson 4Annie Mury SantiagoNo ratings yet
- Mad LabDocument66 pagesMad LabBalamurugan MNo ratings yet
- Reversing a String in 8086 Micro Project ReportDocument4 pagesReversing a String in 8086 Micro Project ReportOm IngleNo ratings yet
- Reference - Unit-V PDFDocument128 pagesReference - Unit-V PDFRamesh BalakrishnanNo ratings yet
- Chanel SWOT AnalysisDocument5 pagesChanel SWOT AnalysisJeish KimNo ratings yet
- Daily Assessment RecordDocument4 pagesDaily Assessment Recordapi-342236522100% (2)
- Organic Facial Remedies Versus Inorganic Facial RemediesDocument13 pagesOrganic Facial Remedies Versus Inorganic Facial Remediesapi-271179911No ratings yet
- Final Annotated BibiliographyDocument4 pagesFinal Annotated Bibiliographyapi-491166748No ratings yet
- Philippine Police Report Suicide InvestigationDocument2 pagesPhilippine Police Report Suicide InvestigationPAUL ALDANA82% (34)
- Serendipity - A Sociological NoteDocument2 pagesSerendipity - A Sociological NoteAmlan BaruahNo ratings yet
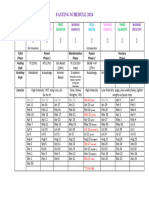
- Moon Fast Schedule 2024Document1 pageMoon Fast Schedule 2024mimiemendoza18No ratings yet
- Presepsi Khalayak Terhadap Program Acara Televise Reality Show "Jika Aku Menjadi" Di Trans TVDocument128 pagesPresepsi Khalayak Terhadap Program Acara Televise Reality Show "Jika Aku Menjadi" Di Trans TVAngga DianNo ratings yet
- 2 5 Marking ScheduleDocument6 pages2 5 Marking Scheduleapi-218511741No ratings yet
- British Isles Composition GuideDocument4 pagesBritish Isles Composition GuidesonmatanalizNo ratings yet
- Bal - 2011 - The New HRM in The 21st Century - A Strategic ViewDocument15 pagesBal - 2011 - The New HRM in The 21st Century - A Strategic ViewJoaquínMartínezMiñoNo ratings yet
- SMEs, Trade Finance and New TechnologyDocument34 pagesSMEs, Trade Finance and New TechnologyADBI EventsNo ratings yet
- Building Primitive Traps & SnaresDocument101 pagesBuilding Primitive Traps & SnaresJoseph Madr90% (10)
- Administracion Una Perspectiva Global Y Empresarial Resumen Por CapitulosDocument7 pagesAdministracion Una Perspectiva Global Y Empresarial Resumen Por Capitulosafmqqaepfaqbah100% (1)
- Staining TechniquesDocument31 pagesStaining TechniquesKhadija JaraNo ratings yet