You might also like
- Definition of Drug-Resistant Epilepsy: A Reappraisal Based On Epilepsy TypesDocument6 pagesDefinition of Drug-Resistant Epilepsy: A Reappraisal Based On Epilepsy TypestsyrahmaniNo ratings yet
- 11-Exploring A Case For Education About Sexual and Gender Minorities in Postgraduate Emergency MeDocument11 pages11-Exploring A Case For Education About Sexual and Gender Minorities in Postgraduate Emergency MetsyrahmaniNo ratings yet
- Acute Manifestations of Neuromuscular DiseaseDocument10 pagesAcute Manifestations of Neuromuscular DiseasetsyrahmaniNo ratings yet
- Acute DizzinessDocument14 pagesAcute DizzinesstsyrahmaniNo ratings yet
- KXZ 319 Jyk JJRCbs 8 H P1 Q NW C4 Lu Z3 ZXJ3 T QIaa 6 H 5Document16 pagesKXZ 319 Jyk JJRCbs 8 H P1 Q NW C4 Lu Z3 ZXJ3 T QIaa 6 H 5tsyrahmaniNo ratings yet
- A Systematic Review of Pre-Interventional Predictors of Functional Outcome in Poor-Grade Aneurysmal Subarachnoid Hemorrhage.Document6 pagesA Systematic Review of Pre-Interventional Predictors of Functional Outcome in Poor-Grade Aneurysmal Subarachnoid Hemorrhage.tsyrahmaniNo ratings yet
- A Clinician's Approach To Peripheral NeuropathyDocument12 pagesA Clinician's Approach To Peripheral Neuropathytsyrahmani100% (1)
- RCT Appraisal Sheets 2005 English-2Document6 pagesRCT Appraisal Sheets 2005 English-2tsyrahmaniNo ratings yet
- MMC 3Document1 pageMMC 3tsyrahmaniNo ratings yet
- Critical Appraisal Checklist 2016-17Document1 pageCritical Appraisal Checklist 2016-17tsyrahmaniNo ratings yet
- MMC 2Document1 pageMMC 2tsyrahmaniNo ratings yet
- MMC 1Document1 pageMMC 1tsyrahmaniNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Loadmasters Customs Services V Glodel Brokerage - 639 SCRA 69Document14 pagesLoadmasters Customs Services V Glodel Brokerage - 639 SCRA 69Krista YntigNo ratings yet
- Karlos KarlinaDocument2 pagesKarlos KarlinaTip RendahNo ratings yet
- Level 11 Passage 1Document5 pagesLevel 11 Passage 1ngotrancheetahNo ratings yet
- Bow LsplanDocument4 pagesBow Lsplanapi-641176937No ratings yet
- Data Communication Computer Networks Notes BCA PDFDocument20 pagesData Communication Computer Networks Notes BCA PDFHemalatha S Chinnu100% (2)
- Environmental StandardsDocument14 pagesEnvironmental StandardsJaswant VermaNo ratings yet
- Confluence Ideathon 2021 X Serendipity Arts Foundation - Concept Document...Document9 pagesConfluence Ideathon 2021 X Serendipity Arts Foundation - Concept Document...sri balachandarNo ratings yet
- Joint Accounts On Forex DepositsDocument2 pagesJoint Accounts On Forex DepositsdailydoseoflawNo ratings yet
- Fig: Superscalar Architecture of PentiumDocument19 pagesFig: Superscalar Architecture of PentiumRathan NNo ratings yet
- Overall ProgramsDocument5 pagesOverall ProgramsLavanyaNo ratings yet
- Bài tậpDocument2 pagesBài tậpminhphuongnmh14No ratings yet
- 10 Xtralis Osid Brochure A4 LoresDocument4 pages10 Xtralis Osid Brochure A4 LoresSathyamoorthy KamakottiNo ratings yet
- Mitsubishi Spilt Type Air Conditioners Manual MSZ hr25vf MSZ hr35vf MSZ hr42vf MSZ hr50vfDocument21 pagesMitsubishi Spilt Type Air Conditioners Manual MSZ hr25vf MSZ hr35vf MSZ hr42vf MSZ hr50vfgerman tapiaNo ratings yet
- Form 4 PF WithdrawlDocument2 pagesForm 4 PF WithdrawlRajshree DubeyNo ratings yet
- The Theory of Stock Market EfficiencyDocument21 pagesThe Theory of Stock Market EfficiencyMario Andres Rubiano RojasNo ratings yet
- Report Project ManagementDocument36 pagesReport Project ManagementVarun Mathur100% (1)
- Outpatient Appointment Systems in Healthcare - A Review of Optimization StudiesDocument32 pagesOutpatient Appointment Systems in Healthcare - A Review of Optimization Studiesgabrieelcrazy100% (1)
- Norwegian School of EconomicsDocument2 pagesNorwegian School of EconomicsVimal AnbalaganNo ratings yet
- 2022, Altay Brusan, Aytac Durmaz, Git For Electronic Circuit Design - CAD and Version Control For Electrical EngineersDocument247 pages2022, Altay Brusan, Aytac Durmaz, Git For Electronic Circuit Design - CAD and Version Control For Electrical EngineersKoay FTNo ratings yet
- Unit-3 CAD CompletedDocument35 pagesUnit-3 CAD CompletedmuthupuviNo ratings yet
- Persuasive Speech Outline Draft 4Document4 pagesPersuasive Speech Outline Draft 4AlexisNo ratings yet
- Rsa536 16 26 10 2018Document13 pagesRsa536 16 26 10 2018samsungindian 2015No ratings yet
- Purged VCR LayoutDocument9 pagesPurged VCR LayoutjjprietojNo ratings yet
- Fufeng Development Agreement Conditions Task ListDocument17 pagesFufeng Development Agreement Conditions Task ListinforumdocsNo ratings yet
- Presentation 1Document1 pagePresentation 1Shahneela ShaileeNo ratings yet
- Multiple Access Techniques LectureDocument23 pagesMultiple Access Techniques LecturefatimamanzoorNo ratings yet
- Arduino - MotorKnobDocument4 pagesArduino - MotorKnobJavier Fernando Vásquez GómezNo ratings yet
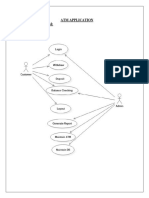
- Atm Application Use Case DiagramDocument58 pagesAtm Application Use Case DiagramS. Mohd TharikNo ratings yet
- Knowledge Work & Human CapitalDocument2 pagesKnowledge Work & Human Capitalchandnioptom100% (2)
- Net Present Value: For New Project ManagersDocument69 pagesNet Present Value: For New Project ManagersErlet Shaqe100% (1)