You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (843)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Quality of Work Life A Study of Jammu UnDocument6 pagesQuality of Work Life A Study of Jammu UnSamah AlshamiNo ratings yet
- العرب و الروم و اللاتين فى الحرب الصليبية الاولى - د.جوزيف نسيم يوسف ، دار النهضة العربية 1981مDocument420 pagesالعرب و الروم و اللاتين فى الحرب الصليبية الاولى - د.جوزيف نسيم يوسف ، دار النهضة العربية 1981مSamah AlshamiNo ratings yet
- PPI1626A01 Total & Direct Bilirubin Rev ADocument2 pagesPPI1626A01 Total & Direct Bilirubin Rev ASamah AlshamiNo ratings yet
- Neonatal and Paediatric Containers For Blood CollectionDocument5 pagesNeonatal and Paediatric Containers For Blood CollectionSamah AlshamiNo ratings yet
- Samah Y. AlShami Food MicrobiologyDocument2 pagesSamah Y. AlShami Food MicrobiologySamah AlshamiNo ratings yet
- Histopathology and Pathogenesis of VascularDocument62 pagesHistopathology and Pathogenesis of VascularSamah AlshamiNo ratings yet
- محاضرة نظري 7 19Document12 pagesمحاضرة نظري 7 19Samah AlshamiNo ratings yet
- Part2 OncologyDocument39 pagesPart2 OncologySamah AlshamiNo ratings yet
- Introduction To VirologyDocument18 pagesIntroduction To VirologySamah AlshamiNo ratings yet
- The Future Ahead Amalia Ulman 2014 Last EditDocument15 pagesThe Future Ahead Amalia Ulman 2014 Last EditSebastian Marquez AdameNo ratings yet
- Recta Ratio Agibilium in A Medical Context The Role of Virtue in The Physician Patient RelationshipDocument5 pagesRecta Ratio Agibilium in A Medical Context The Role of Virtue in The Physician Patient RelationshipIvonneNo ratings yet
- 597 9 Continuous ImprovementDocument3 pages597 9 Continuous ImprovementIsmail SultanNo ratings yet
- Dengue Management in Primary CareDocument61 pagesDengue Management in Primary CareDaniel RajNo ratings yet
- Unit 7 - Exercise 16 & 17 - 070 - Iffah Muthiah FirmanDocument3 pagesUnit 7 - Exercise 16 & 17 - 070 - Iffah Muthiah FirmanRisalNo ratings yet
- Villamar, Rolando Pmls ManualDocument19 pagesVillamar, Rolando Pmls ManualVILLAMAR, Rolando Jr. V.No ratings yet
- SEAFDEC/AQD Institutional Repository (SAIR) : This Document Is Downloaded At: 2013-07-02 07:11:51 CSTDocument53 pagesSEAFDEC/AQD Institutional Repository (SAIR) : This Document Is Downloaded At: 2013-07-02 07:11:51 CSTKarl KiwisNo ratings yet
- Nelson Science Perspectives 10 - Full Evaluation BookDocument628 pagesNelson Science Perspectives 10 - Full Evaluation Bookacchow7No ratings yet
- Lesson 4Document27 pagesLesson 4Hector CandidoNo ratings yet
- Physiologic Changes in Aging Affecting Various SystemsDocument27 pagesPhysiologic Changes in Aging Affecting Various SystemsMina75% (4)
- OTITIS MEDIA - Nov - 2020Document109 pagesOTITIS MEDIA - Nov - 2020NicNo ratings yet
- Pop (Aa)Document37 pagesPop (Aa)James BondNo ratings yet
- Rachel Ellick Daily Diaries CombinedDocument8 pagesRachel Ellick Daily Diaries CombinedjonsokolowNo ratings yet
- Week 3 Active Recreation SportsDocument22 pagesWeek 3 Active Recreation SportsRyzza Mae BautistaNo ratings yet
- 33460-Msds Mama LemonDocument6 pages33460-Msds Mama LemonISS Medikaloka ManadoNo ratings yet
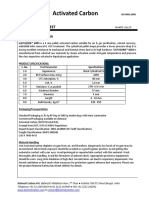
- Activated Carbon: Technical DatasheetDocument2 pagesActivated Carbon: Technical DatasheetManikandan SWMSNo ratings yet
- Nice Nurses Healthcare CenterDocument45 pagesNice Nurses Healthcare CenterDe Guzman John Erick AdelanteNo ratings yet
- Goa Factories Rules 1985Document392 pagesGoa Factories Rules 1985jacobpm2010No ratings yet
- U2-Kreuter EtalDocument19 pagesU2-Kreuter EtalLauritoNo ratings yet
- Factors Affecting Poultry Meat Yields PDFDocument19 pagesFactors Affecting Poultry Meat Yields PDFRona BautistaNo ratings yet
- Addis Ababa University Thesis On Civil EngineeringDocument6 pagesAddis Ababa University Thesis On Civil Engineeringsheritorizsaltlakecity100% (2)
- Venn Diagrams ExerciseDocument5 pagesVenn Diagrams ExerciseSharksNo ratings yet
- Health and Safety in TheatreDocument1 pageHealth and Safety in Theatreapi-693461954No ratings yet
- 6 Certificate Course in Clinical Nutrition 01012019Document17 pages6 Certificate Course in Clinical Nutrition 01012019Ryzhon Dragon0% (1)
- Jason Prall Ultimate Gut Repair BlueprintDocument7 pagesJason Prall Ultimate Gut Repair BlueprintioanaNo ratings yet
- Implement The Zero Garbage System at Domestic LevelDocument5 pagesImplement The Zero Garbage System at Domestic Levelsamar karemoreNo ratings yet
- Management of Adult Patients Supported With.1Document10 pagesManagement of Adult Patients Supported With.1Freddy Shanner Chávez VásquezNo ratings yet
- AaaaaDocument10 pagesAaaaaRobert AquinoNo ratings yet
- Diabetes Among HIV-Infected Patients On Antiretroviral Therapy at Mulago National Referral Hospital in Central UgandaDocument6 pagesDiabetes Among HIV-Infected Patients On Antiretroviral Therapy at Mulago National Referral Hospital in Central Ugandassentongo JohnmaryNo ratings yet
- Sexuality and Sexual HealthDocument60 pagesSexuality and Sexual HealthMonika shankarNo ratings yet