You might also like
- The SAGES Manual of Robotic SurgeryFrom EverandThe SAGES Manual of Robotic SurgeryAnkit D. PatelNo ratings yet
- Comprehensive Healthcare Simulation: Surgery and Surgical SubspecialtiesFrom EverandComprehensive Healthcare Simulation: Surgery and Surgical SubspecialtiesDimitrios StefanidisNo ratings yet
- Virtual SurgeryDocument20 pagesVirtual SurgeryMidhun MadhavanNo ratings yet
- Virtual Surgery 07012013125131 Virtual SurgeryDocument20 pagesVirtual Surgery 07012013125131 Virtual Surgeryjosemonj77No ratings yet
- Residency Training in Robotic Surgery The Role of SimulationDocument7 pagesResidency Training in Robotic Surgery The Role of SimulationGabrielly RobledilhoNo ratings yet
- Bjs 9711Document15 pagesBjs 9711Bintang MuslimahNo ratings yet
- Technical Seminar PPTDocument15 pagesTechnical Seminar PPTshashidharsykNo ratings yet
- Seminar Report On Virtual SurgeryDocument17 pagesSeminar Report On Virtual SurgeryAfrah RamsheedNo ratings yet
- Virtual SurgeryDocument22 pagesVirtual SurgeryMounika Surapaneni100% (1)
- Walliczek Dworschak2016Document10 pagesWalliczek Dworschak2016Eham AroraNo ratings yet
- Emergence of Three-Dimensional Video Microsurgery For Male InfertilityDocument2 pagesEmergence of Three-Dimensional Video Microsurgery For Male InfertilityZaliyaNo ratings yet
- Virtual Surgery ReportDocument6 pagesVirtual Surgery ReportNaveen Krishnan75% (4)
- The Use of Surgical Simulators To Reduce ErrorsDocument14 pagesThe Use of Surgical Simulators To Reduce ErrorsVasenkoMishaNo ratings yet
- Robotics in General Surgery: James Wall, MD, Venita Chandra, MD and Thomas Krummel, MDDocument18 pagesRobotics in General Surgery: James Wall, MD, Venita Chandra, MD and Thomas Krummel, MDRizwan AhmedNo ratings yet
- Jara 2020Document8 pagesJara 2020Ágoston János CsigiNo ratings yet
- CH 3Document21 pagesCH 3Mohamed AhmedNo ratings yet
- Simulation Improves Patient SafetyDocument5 pagesSimulation Improves Patient SafetyZeptalanNo ratings yet
- 10.1007/s00464 017 5634 6 PDFDocument11 pages10.1007/s00464 017 5634 6 PDFAnonymous wVUGfwWSYNo ratings yet
- Robotic-Assisted Surgery For Low Rectal Dissection: From Better Views To Better OutcomeDocument6 pagesRobotic-Assisted Surgery For Low Rectal Dissection: From Better Views To Better OutcomeMarwa MedNo ratings yet
- Vs ReportDocument20 pagesVs ReportSagar PawadiNo ratings yet
- Preliminary Design and Evaluation of A Remote Tele Mentoring System For Minimally Invasive SurgeryDocument12 pagesPreliminary Design and Evaluation of A Remote Tele Mentoring System For Minimally Invasive Surgeryjackie tesilloNo ratings yet
- Collaborative Robotics Toolkit CRTK Open Software Framework For Surgical Robotics Research-2Document8 pagesCollaborative Robotics Toolkit CRTK Open Software Framework For Surgical Robotics Research-2Varun KumarNo ratings yet
- 1 s2.0 S1931720414000749 MainDocument6 pages1 s2.0 S1931720414000749 MainFarzadNo ratings yet
- Adaptive Architecture Supports Context-Aware Collaborative Surgical SimulatorsDocument2 pagesAdaptive Architecture Supports Context-Aware Collaborative Surgical SimulatorsJhofran ArleyNo ratings yet
- Me326 Individual ProjectDocument5 pagesMe326 Individual Projectapi-582462159No ratings yet
- Latest Trends in Minimally Invasive SurgeryDocument4 pagesLatest Trends in Minimally Invasive SurgeryMc_Lopez_1761No ratings yet
- A Development of Assistant Surgical Robot System Based On Surgical Operation by Wire and Hands On Throttle and Stick 2016Document19 pagesA Development of Assistant Surgical Robot System Based On Surgical Operation by Wire and Hands On Throttle and Stick 2016Andualem TadesseNo ratings yet
- Trainpdt EVT0905 Featured Inno 01 Us PiDocument3 pagesTrainpdt EVT0905 Featured Inno 01 Us PiSandeep KumarNo ratings yet
- Virtual Reality Simulation To Enhance Laparoscopic Salpingectomy SkillsDocument7 pagesVirtual Reality Simulation To Enhance Laparoscopic Salpingectomy SkillsHanna 123No ratings yet
- Augmented Reality To Improve Surgical Simulation Lessons Learned Towards The Design of A Hybrid Laparoscopic Simulator For CholecystectomyDocument14 pagesAugmented Reality To Improve Surgical Simulation Lessons Learned Towards The Design of A Hybrid Laparoscopic Simulator For CholecystectomyJohn DoeNo ratings yet
- VR simulation for CPR trainingDocument17 pagesVR simulation for CPR trainingomamah.almousaNo ratings yet
- Augmented-Reality-Based-Visual-Haptic-Modeling-For 2021 Virtual-Reality - inDocument13 pagesAugmented-Reality-Based-Visual-Haptic-Modeling-For 2021 Virtual-Reality - inapi-688059491No ratings yet
- Icu 58 297 PDFDocument2 pagesIcu 58 297 PDFNeil GriggNo ratings yet
- 2023-PEg TRAnsfer Workflow Recognition Challenge Report - Do Multimodal Data Improve RecognitionDocument18 pages2023-PEg TRAnsfer Workflow Recognition Challenge Report - Do Multimodal Data Improve RecognitionlancerhlyNo ratings yet
- New Microsoft Office Word Document1Document46 pagesNew Microsoft Office Word Document1rajaishaNo ratings yet
- Assignment 4 SolutionDocument6 pagesAssignment 4 SolutionAya SulaqNo ratings yet
- Viglialoro 2018Document14 pagesViglialoro 2018vishalmate10No ratings yet
- REMOTE SURGERY: TELESURGERY OVER LONG DISTANCESDocument6 pagesREMOTE SURGERY: TELESURGERY OVER LONG DISTANCESramananbmeNo ratings yet
- Robotic Surgery A Current Perspective: ObjectiveDocument7 pagesRobotic Surgery A Current Perspective: ObjectiveirismgallNo ratings yet
- Robotics in Colorectal Surgery: Telemonitoring and TeleroboticsDocument10 pagesRobotics in Colorectal Surgery: Telemonitoring and TeleroboticsprivedNo ratings yet
- Surgeons Strive Hard To Break The Da Vinci CodeDocument3 pagesSurgeons Strive Hard To Break The Da Vinci CodeasdasddsaNo ratings yet
- Korzeniowski 2016Document13 pagesKorzeniowski 2016KhalilSemlaliNo ratings yet
- Survey on impact of Robotics on HealthcareDocument8 pagesSurvey on impact of Robotics on Healthcareharsh3112aNo ratings yet
- Robotic Nurse Duties in The Urology Operative Room: 11 Years of ExperienceDocument8 pagesRobotic Nurse Duties in The Urology Operative Room: 11 Years of ExperienceLaura CursaruNo ratings yet
- Computer Vision in The Surgical Operating Room: Review ArticleDocument7 pagesComputer Vision in The Surgical Operating Room: Review Articlelabril.torresmNo ratings yet
- Robo SurgeryDocument9 pagesRobo Surgeryrwong1231No ratings yet
- Coles, Meglan, John - 2010 - The Role of Haptics in Medical Training Simulators A Survey of The State-Of-The-ArtDocument18 pagesColes, Meglan, John - 2010 - The Role of Haptics in Medical Training Simulators A Survey of The State-Of-The-ArtNigel W. JohnNo ratings yet
- Robotic SurgeryDocument11 pagesRobotic SurgerySam AlatawiNo ratings yet
- Enhanced Recovery Simulation in Colorectal Surgery: Design of Virtual Online PatientsDocument9 pagesEnhanced Recovery Simulation in Colorectal Surgery: Design of Virtual Online PatientsjohanisNo ratings yet
- Anaesthesia For Robotic SurgeryDocument5 pagesAnaesthesia For Robotic Surgerysangamitraachu100% (1)
- Training in Uniportal VATS LobectomyDocument7 pagesTraining in Uniportal VATS LobectomyAlin Ionut BurlacuNo ratings yet
- RoboticSurgery An Evolution in PracticeDocument3 pagesRoboticSurgery An Evolution in PracticeJoão Lourenço0% (1)
- "Reality Is Merely An Illusion, Although A Very Persistent One." - Albert Einstein (German Born American Physicist)Document28 pages"Reality Is Merely An Illusion, Although A Very Persistent One." - Albert Einstein (German Born American Physicist)Nitin KumarNo ratings yet
- Urologic Robots and Future Directions: Dan Stoianovici, PHDDocument10 pagesUrologic Robots and Future Directions: Dan Stoianovici, PHDavinashjhamechxNo ratings yet
- Adhami2000 Chapter PlanningAndSimulationOfRoboticDocument10 pagesAdhami2000 Chapter PlanningAndSimulationOfRoboticYessica RosasNo ratings yet
- Robot Assisted Surgery1Document18 pagesRobot Assisted Surgery1Mahesh JoshiNo ratings yet
- Bhandari 2019Document7 pagesBhandari 2019Ágoston János CsigiNo ratings yet
- Review of DL in Minimally Invasive SurgeryDocument21 pagesReview of DL in Minimally Invasive SurgeryJoel JacobNo ratings yet
- Indoor Navigation Strategies for Aerial Autonomous SystemsFrom EverandIndoor Navigation Strategies for Aerial Autonomous SystemsRating: 5 out of 5 stars5/5 (2)
- Bariatric Robotic Surgery: A Comprehensive GuideFrom EverandBariatric Robotic Surgery: A Comprehensive GuideCarlos Eduardo DomeneNo ratings yet
- Hernia-To-Neck Ratio Is Associated With Emergent Ventral Hernia Repair - PubMedDocument1 pageHernia-To-Neck Ratio Is Associated With Emergent Ventral Hernia Repair - PubMedEham AroraNo ratings yet
- Al-Mansour2021 Validation of A Simple Technique of Volumetric Analysis of Complex Hernias Without 3D ReconstructionDocument7 pagesAl-Mansour2021 Validation of A Simple Technique of Volumetric Analysis of Complex Hernias Without 3D ReconstructionEham AroraNo ratings yet
- Fafaj2021 Tanaka Score ReliabilityDocument6 pagesFafaj2021 Tanaka Score ReliabilityEham AroraNo ratings yet
- Mommers2017 Impact of Hernia Volume On Pulmonary Complications in Complex Hernia RepairsDocument6 pagesMommers2017 Impact of Hernia Volume On Pulmonary Complications in Complex Hernia RepairsEham AroraNo ratings yet
- Hassan2022 Novel Machine Learning Approach For The Prediction of Hernia Recurrence, Surgical Complication, and 30-Day Readmission After Abdominal Wall ReconstructionDocument10 pagesHassan2022 Novel Machine Learning Approach For The Prediction of Hernia Recurrence, Surgical Complication, and 30-Day Readmission After Abdominal Wall ReconstructionEham AroraNo ratings yet
- Objective Assessment of Technical Surgical SkillsDocument17 pagesObjective Assessment of Technical Surgical SkillsEham AroraNo ratings yet
- The Effect of Different Training Exercises On The Performance Outcome On The Da Vinci Skills SimulatorDocument9 pagesThe Effect of Different Training Exercises On The Performance Outcome On The Da Vinci Skills SimulatorEham AroraNo ratings yet
- Walliczek Dworschak2016Document10 pagesWalliczek Dworschak2016Eham AroraNo ratings yet
- Objective Structured Assessment of Technical Skill (OSATS) For Surgical ResidentsDocument6 pagesObjective Structured Assessment of Technical Skill (OSATS) For Surgical ResidentsEham AroraNo ratings yet
- User Guide For Speedlink: Hearing Instrument Programming InterfaceDocument26 pagesUser Guide For Speedlink: Hearing Instrument Programming InterfaceMarcio Lobo SelvagemNo ratings yet
- 16V2000 Detroit W5Document2 pages16V2000 Detroit W5Rendy Chavez LesmanaNo ratings yet
- DS3 QueuesDocument38 pagesDS3 QueuesHabib ur rehmanNo ratings yet
- Project Managemen 2 PDFDocument14 pagesProject Managemen 2 PDFMisha RanaNo ratings yet
- Journal of Energy StorageDocument14 pagesJournal of Energy StorageLuis Antonio CNo ratings yet
- SET UP EQMOD SOFTWARE FOR ASTROPHOTOGRAPHYDocument5 pagesSET UP EQMOD SOFTWARE FOR ASTROPHOTOGRAPHYMechtatel HrenovNo ratings yet
- RSP Robinson R44 Quick Start Guide BETA1.1Document14 pagesRSP Robinson R44 Quick Start Guide BETA1.1CristianoVelosodeQueirozNo ratings yet
- Memorandum: From: TJC and Associates, Inc. Date: March, 2014 Subject: Seismic Anchorage Submittals ChecklistDocument2 pagesMemorandum: From: TJC and Associates, Inc. Date: March, 2014 Subject: Seismic Anchorage Submittals ChecklistponjoveNo ratings yet
- Induction Cooker Circuit DesignDocument39 pagesInduction Cooker Circuit DesignMr. Pushparaj Ghodke74% (31)
- Colas Rail Brochure CORPORATE v4 0Document28 pagesColas Rail Brochure CORPORATE v4 0mostafa shoshaNo ratings yet
- All Motor, &electrical Equipment in StorDocument8 pagesAll Motor, &electrical Equipment in StorMd. Saddam HossainNo ratings yet
- SRX SFP 10ge Dac 1MDocument7 pagesSRX SFP 10ge Dac 1MAssem SamirNo ratings yet
- 6 - StringsDocument19 pages6 - Stringsaljazi mNo ratings yet
- SG110CXPV Grid-Connected Inverter User ManualDocument101 pagesSG110CXPV Grid-Connected Inverter User ManualAizat AlongNo ratings yet
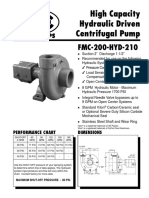
- FMC 200 Hyd 210Document2 pagesFMC 200 Hyd 210Ruben SaccoNo ratings yet
- CCIE SPv4 Topology DiagramsDocument17 pagesCCIE SPv4 Topology DiagramsTilak RoyNo ratings yet
- Lecture - Week - 3 - Software MetricsDocument29 pagesLecture - Week - 3 - Software MetricsManlNo ratings yet
- Mrs J's Resource Creations ©Document7 pagesMrs J's Resource Creations ©syddysNo ratings yet
- Service Bulletin: Fuel Injection PumpDocument15 pagesService Bulletin: Fuel Injection PumpKrunoslavNo ratings yet
- + - OSDI2020-FIRM - An Intelligent Fine-Grained Resource Management Framework For SLO-Oriented MicroservicesDocument22 pages+ - OSDI2020-FIRM - An Intelligent Fine-Grained Resource Management Framework For SLO-Oriented MicroservicesBENKEMCHI OussamaNo ratings yet
- 9Document36 pages9vscolegit shoppeNo ratings yet
- Networks Pre Connection Attacks PDFDocument15 pagesNetworks Pre Connection Attacks PDFaniket kasturiNo ratings yet
- Luanshya Technical College SCADA Scan IntervalDocument5 pagesLuanshya Technical College SCADA Scan IntervalAlfred K ChilufyaNo ratings yet
- Prediction of Stock Price Based On Hidden Markov Model and Nearest Neighbour AlgorithmDocument31 pagesPrediction of Stock Price Based On Hidden Markov Model and Nearest Neighbour AlgorithmFirman AkbarNo ratings yet
- Data Mining 1-3Document29 pagesData Mining 1-3Singer JerowNo ratings yet
- MTB 500i W R TXM Technical ManualDocument26 pagesMTB 500i W R TXM Technical ManualSaranyoo CHOOTIMASNo ratings yet
- Ryobi 18 Volt Impact Wrench Model Number P261 Repair SheetDocument4 pagesRyobi 18 Volt Impact Wrench Model Number P261 Repair SheetRicardo Ran Pos100% (1)
- CMT1Document10 pagesCMT1Dongneu Nguyen100% (1)
- Lesson Plan in Random VariableDocument10 pagesLesson Plan in Random VariableJeson N. RondinaNo ratings yet
- Control Valves PDFDocument21 pagesControl Valves PDFRiyadh DaoudiNo ratings yet