You might also like
- Virologic Failure in HIV: An Updated Clinician’s Guide to Assessment and ManagementFrom EverandVirologic Failure in HIV: An Updated Clinician’s Guide to Assessment and ManagementNo ratings yet
- Pedsos 1Document7 pagesPedsos 1RizalMarubobSilalahiNo ratings yet
- Notes For The Record Meuri EbolaDocument7 pagesNotes For The Record Meuri EbolaIgnacio MastroleoNo ratings yet
- Safety VaccinesDocument11 pagesSafety VaccinesRaju BaiNo ratings yet
- Wagner2022 Article EfficacyAndSafetyOfIntravenousDocument13 pagesWagner2022 Article EfficacyAndSafetyOfIntravenoustito reddyNo ratings yet
- Abaclinicaltrialofvaccine 181119065907Document34 pagesAbaclinicaltrialofvaccine 181119065907vũ đình dũngNo ratings yet
- Medication Errors in A Neonatal Unit: One of The Main Adverse EventsDocument7 pagesMedication Errors in A Neonatal Unit: One of The Main Adverse EventsarpinaNo ratings yet
- 1475-2875-8-272 (DHA-PQ Vs AL)Document8 pages1475-2875-8-272 (DHA-PQ Vs AL)Samuel UzonduNo ratings yet
- Introduction To Pharmacovigilance (PDFDrive)Document227 pagesIntroduction To Pharmacovigilance (PDFDrive)Supriya Ghanekar PhadkeNo ratings yet
- Prevalence, Risk Factors, and Optimized Management of Moderate To Severe Thirst in The Post Anesthesia Care UnitDocument10 pagesPrevalence, Risk Factors, and Optimized Management of Moderate To Severe Thirst in The Post Anesthesia Care Unitpooria shNo ratings yet
- Safety of Higher Doses of Ivermectin JAC 2020Document8 pagesSafety of Higher Doses of Ivermectin JAC 2020Amalia Ade DiamitaNo ratings yet
- Pharmacovigilance - Dr. Ganesh UchitDocument58 pagesPharmacovigilance - Dr. Ganesh UchitSshan ChaturvediNo ratings yet
- CLINICAL-PHARMACY ReviewerDocument21 pagesCLINICAL-PHARMACY ReviewerParamjit KaurNo ratings yet
- A Multicenter Point Prevalence Survey of Antibiotic Use in Haiti Juneaugust 2019 Findings and ImplicationsDocument2 pagesA Multicenter Point Prevalence Survey of Antibiotic Use in Haiti Juneaugust 2019 Findings and ImplicationsMentor Ali Ber LucienNo ratings yet
- Sistem PelaporanDocument21 pagesSistem PelaporanRifat SaufiNo ratings yet
- Monkeypox and Pregnancy - What Maternal-Fetal Medicine Subspecialists Need To KnowDocument7 pagesMonkeypox and Pregnancy - What Maternal-Fetal Medicine Subspecialists Need To KnowariniNo ratings yet
- Young Febrile Infants Step by Step EvaluationDocument2 pagesYoung Febrile Infants Step by Step Evaluationhossein kasiriNo ratings yet
- Introduction To Vaccine PharmacovigilanceDocument36 pagesIntroduction To Vaccine PharmacovigilanceAthira RaviNo ratings yet
- Module1 Measles&RubellaDocument52 pagesModule1 Measles&Rubellasakshi gNo ratings yet
- Philippine COVID-19 Living Clinical Practice Guidelines: Consensus IssuesDocument14 pagesPhilippine COVID-19 Living Clinical Practice Guidelines: Consensus IssuesppgpcsNo ratings yet
- Jurnal EED 3Document10 pagesJurnal EED 3Garsa GarnolNo ratings yet
- HiTEMP TrialDocument8 pagesHiTEMP TrialJorge BarriosNo ratings yet
- Summary of The Evidence For Ivermectin in COVID-19Document3 pagesSummary of The Evidence For Ivermectin in COVID-19Kent CheeNo ratings yet
- Fitzpatricks Dermatology 9th Edition 3124Document1 pageFitzpatricks Dermatology 9th Edition 3124DennisSujayaNo ratings yet
- Introduction To Post-Marketing Drug Safety Surveillance:: Pharmacovigilance in FDA/CDERDocument56 pagesIntroduction To Post-Marketing Drug Safety Surveillance:: Pharmacovigilance in FDA/CDERMuhammad RizaldiNo ratings yet
- Antimicrobial Therapy and Its Modification After Diagnostic Test InterpretationDocument29 pagesAntimicrobial Therapy and Its Modification After Diagnostic Test Interpretationeka kemala sariNo ratings yet
- Determinants of Virological Failure Among Adults oDocument9 pagesDeterminants of Virological Failure Among Adults oDefinta AnisaNo ratings yet
- Vaccine Safety Survillance - Pharmaovigilance Method - Communication in PharmacovigilanceDocument16 pagesVaccine Safety Survillance - Pharmaovigilance Method - Communication in PharmacovigilancesaifNo ratings yet
- Antiviral Efficacy of Favipiravir Against Ebola Virus: A Translational Study in Cynomolgus MacaquesDocument21 pagesAntiviral Efficacy of Favipiravir Against Ebola Virus: A Translational Study in Cynomolgus MacaquesFiona ValenciaNo ratings yet
- Immunizaton During PregnancyDocument6 pagesImmunizaton During PregnancyMohamed SulimanNo ratings yet
- Aborto Septico 2020Document5 pagesAborto Septico 2020Adrian Pardo VillegasNo ratings yet
- Covigilance Question BankDocument44 pagesCovigilance Question BankDrx Rinku KunduNo ratings yet
- 2015 - Laboratory Based Nationwide SurveillanceDocument12 pages2015 - Laboratory Based Nationwide SurveillanceYulia HandayaniNo ratings yet
- International Immunopharmacology: Meta-Analysis of Randomized Controlled TrialsDocument9 pagesInternational Immunopharmacology: Meta-Analysis of Randomized Controlled TrialsPujiNo ratings yet
- Timing of Administration of Prophylactic Antibiotics For Caesarean Section: A Systematic Review and Meta-AnalysisDocument9 pagesTiming of Administration of Prophylactic Antibiotics For Caesarean Section: A Systematic Review and Meta-AnalysissriNo ratings yet
- Effectiveness of Investments in Leadership and Management Capacity in Thecontext of National Epi ProgramsDocument2 pagesEffectiveness of Investments in Leadership and Management Capacity in Thecontext of National Epi ProgramsZheefNo ratings yet
- FLCCC Summary of The Evidence of Ivermectin in COVID 19Document3 pagesFLCCC Summary of The Evidence of Ivermectin in COVID 19Muhamad ZaidNo ratings yet
- Wu 2015Document7 pagesWu 2015Noel Saúl Argüello SánchezNo ratings yet
- Materi 2 AMR KPRADocument53 pagesMateri 2 AMR KPRArizkiameliahexshaNo ratings yet
- World Health Organization (WHO) - 2014 - Potential Ebola Therapies and Vaccines Interim GuDocument31 pagesWorld Health Organization (WHO) - 2014 - Potential Ebola Therapies and Vaccines Interim GuIgnacio MastroleoNo ratings yet
- Pharmacovigilance: FROMDocument46 pagesPharmacovigilance: FROMmeyhal17No ratings yet
- Patient Safety in The NICUDocument10 pagesPatient Safety in The NICUINGRID YISEL IDROBO AGREDONo ratings yet
- Mooc Phi Lab enDocument18 pagesMooc Phi Lab enAL Babaran CanceranNo ratings yet
- Rubin2013 ImunisasiDocument57 pagesRubin2013 ImunisasiIma SoniaNo ratings yet
- bbLab3ABO DSp11Document18 pagesbbLab3ABO DSp11Ibrahim HashimNo ratings yet
- Carcinogenicity Assessment of Biologics: June 13, 2013Document41 pagesCarcinogenicity Assessment of Biologics: June 13, 2013claudedNo ratings yet
- Patient Centred Surveillance of Drug Resistant PathogensDocument19 pagesPatient Centred Surveillance of Drug Resistant PathogensHanna alexanderNo ratings yet
- What Is The Role of Technology in Improving Patient Safety? A French, German and UK Healthcare Professional PerspectiveDocument6 pagesWhat Is The Role of Technology in Improving Patient Safety? A French, German and UK Healthcare Professional PerspectiveTricia Jane OpinaldoNo ratings yet
- Study On Emergence of MDR Pathogen and Its Microbiological StudyDocument9 pagesStudy On Emergence of MDR Pathogen and Its Microbiological StudyIJAR JOURNALNo ratings yet
- ZZZZZZZZZZZZZZDocument8 pagesZZZZZZZZZZZZZZchloramphenicolNo ratings yet
- Research Sites July 14 2020Document23 pagesResearch Sites July 14 2020Crist VillarNo ratings yet
- Dear Author: Annotate PDFDocument14 pagesDear Author: Annotate PDFLinh PhamNo ratings yet
- Unit 3 PharmacovigilanceDocument16 pagesUnit 3 Pharmacovigilancerakesh meherNo ratings yet
- Risk Factors For Ventilator-Associated Events - Liu 2019Document6 pagesRisk Factors For Ventilator-Associated Events - Liu 2019Maxi BoniniNo ratings yet
- MLT 107 Chapter 3 5 Infection Cont and QADocument29 pagesMLT 107 Chapter 3 5 Infection Cont and QACristina CunhaNo ratings yet
- List of AbbreviationsDocument30 pagesList of AbbreviationsKomang ParmawatiNo ratings yet
- PharmacovilgilanceDocument60 pagesPharmacovilgilanceMohanad Al-BayatiNo ratings yet
- Pi Is 0161642016307357Document11 pagesPi Is 0161642016307357mono1144No ratings yet
- P0581 548 Risk Factors of Severity of Dengue.639Document1 pageP0581 548 Risk Factors of Severity of Dengue.639Hendri HariyantoNo ratings yet
- Antimicrobial Stewardship in NICU - Mulya Rahma Karyanti-1Document53 pagesAntimicrobial Stewardship in NICU - Mulya Rahma Karyanti-1Enny AndrianiNo ratings yet
- Tube Filling Machine LayoutDocument1 pageTube Filling Machine LayoutBashirNo ratings yet
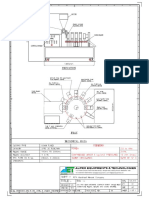
- GA Drawing For Toothpast Mfg. PLNTDocument1 pageGA Drawing For Toothpast Mfg. PLNTBashirNo ratings yet
- Our Nigerian Products 10Document4 pagesOur Nigerian Products 10BashirNo ratings yet
- Marshaal Herat - Ointment Plant 300 Kgs. & Tube Filling MachineDocument11 pagesMarshaal Herat - Ointment Plant 300 Kgs. & Tube Filling MachineBashirNo ratings yet
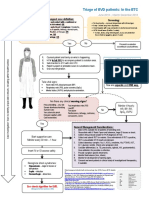
- WHO MOOC Clinical-management-Of-Ebola Poster Triage-Algorithm enDocument1 pageWHO MOOC Clinical-management-Of-Ebola Poster Triage-Algorithm enBashirNo ratings yet
- Introduction LetterDocument1 pageIntroduction LetterBashirNo ratings yet
- KPM Major CLient ListDocument4 pagesKPM Major CLient ListBashirNo ratings yet
- Resume 144615235Document1 pageResume 144615235BashirNo ratings yet
- Medical BotDocument1 pageMedical BotBashirNo ratings yet
- Envelope - Answer Key The Ebola Wars General Edition Answers PDF 5879456 Smithkeelin1234 Gmail ComDocument10 pagesEnvelope - Answer Key The Ebola Wars General Edition Answers PDF 5879456 Smithkeelin1234 Gmail ComKeelin smithNo ratings yet
- Donini, Marusic - 2019 - Current State-Of-The-Art in Plant-Based Antibody Production Systems PDFDocument12 pagesDonini, Marusic - 2019 - Current State-Of-The-Art in Plant-Based Antibody Production Systems PDFAndrei TatomirNo ratings yet
- Annotated BibliographyDocument3 pagesAnnotated BibliographypeterhjeonNo ratings yet
- Forbes - November 3 2014 USADocument126 pagesForbes - November 3 2014 USAalx_ppscuNo ratings yet
- State of Preparation: SLC States and The Ebola VirusDocument8 pagesState of Preparation: SLC States and The Ebola VirusThe Council of State GovernmentsNo ratings yet
- Breakthrough Treatments For Ebola Virus Disease, But No Access-What Went Wrong, and How Can We Do Better?Document6 pagesBreakthrough Treatments For Ebola Virus Disease, But No Access-What Went Wrong, and How Can We Do Better?Stavya DubeyNo ratings yet
- WBI03 01 Que 20181024Document12 pagesWBI03 01 Que 20181024Aleema AsgharNo ratings yet
- Ebola Virus Disease: A Review On Epidemiology, Symptoms, Treatment and PathogenesisDocument8 pagesEbola Virus Disease: A Review On Epidemiology, Symptoms, Treatment and PathogenesisAuliaZahraNo ratings yet
- Ethical EbolaDocument12 pagesEthical EbolaFrancis MaldonadoNo ratings yet
- The Ebola WarsDocument21 pagesThe Ebola WarsIndra DwinataNo ratings yet
- 08-30-14 EditionDocument36 pages08-30-14 EditionSan Mateo Daily JournalNo ratings yet
- CDC Ebola Key Messages 10-30 14finalDocument24 pagesCDC Ebola Key Messages 10-30 14finalapi-232950579No ratings yet