You might also like
- Answer SheetsDocument6 pagesAnswer Sheetsapple aguilinaNo ratings yet
- 1 Activity Sheet Bread and Pastry Production Grades 7-10Document3 pages1 Activity Sheet Bread and Pastry Production Grades 7-10Anne AlejandrinoNo ratings yet
- Apeh 9 - Answersheet NAME: - GRADE & SECTIONDocument2 pagesApeh 9 - Answersheet NAME: - GRADE & SECTIONElmer john de LeonNo ratings yet
- FILIPINO 8 Module 1&2Document2 pagesFILIPINO 8 Module 1&2Romeo AvancenaNo ratings yet
- Answer Sheet TLE 10 - Module 4Document2 pagesAnswer Sheet TLE 10 - Module 4Pedro GenosasNo ratings yet
- Ils q2 M 567 Answer SheetDocument4 pagesIls q2 M 567 Answer SheetMak BellenNo ratings yet
- What's More Direction: Write TRUE or FALSEDocument2 pagesWhat's More Direction: Write TRUE or FALSEEverly OballoNo ratings yet
- Answer SheetDocument5 pagesAnswer SheetangeliNo ratings yet
- PR 1 Week 1 WorksheetDocument1 pagePR 1 Week 1 WorksheetIsabela Russel VillapandoNo ratings yet
- Answer Sheet - 1ST Summative TestDocument4 pagesAnswer Sheet - 1ST Summative TestJovelynNo ratings yet
- ANSWER SHEET LS1 English Context CluesDocument6 pagesANSWER SHEET LS1 English Context CluesKarylcabigas CabigasNo ratings yet
- Self-Evaluation Form Form 7. Module 1. Test.: TASK Topic Max - Points Your Points Your %Document2 pagesSelf-Evaluation Form Form 7. Module 1. Test.: TASK Topic Max - Points Your Points Your %Katrina VasilenokaNo ratings yet
- Sci7 Wk3-4 Q2 Answer SheetDocument2 pagesSci7 Wk3-4 Q2 Answer SheetRav De VeneciaNo ratings yet
- Answersheet 7 Health Q1Document2 pagesAnswersheet 7 Health Q1Elmer john de LeonNo ratings yet
- Tle 6 Answer Sheet Module 5Document2 pagesTle 6 Answer Sheet Module 5EulogiaNo ratings yet
- English Department Answer Sheet in English 7 Module 5 Week 5Document2 pagesEnglish Department Answer Sheet in English 7 Module 5 Week 5Jennifer Gapuz GalletaNo ratings yet
- General BiologyDocument2 pagesGeneral BiologyJamilah BaruangNo ratings yet
- Science 9 - Quarter 1: LESSON 1: Activity 2: What A Bunch of Grapes!Document3 pagesScience 9 - Quarter 1: LESSON 1: Activity 2: What A Bunch of Grapes!Lynxia VrtcNo ratings yet
- Mphohlo Daily Take 5Document1 pageMphohlo Daily Take 5Lwandziso DlaminiNo ratings yet
- Learning Activity Sheets English 8Document4 pagesLearning Activity Sheets English 8denmar valdepenasNo ratings yet
- Activity Work SheetDocument2 pagesActivity Work SheetLoid AguhobNo ratings yet
- Answer Sheet For Week 2: English 7 - Quarter 1Document2 pagesAnswer Sheet For Week 2: English 7 - Quarter 1Sheena May DikitananNo ratings yet
- School Holiday Writing Practice: A Practice A Day, Keeps The E Away!Document8 pagesSchool Holiday Writing Practice: A Practice A Day, Keeps The E Away!goodsfa88No ratings yet
- 1827Document2 pages1827jeirasabucdalao6No ratings yet
- 4 Quarter - Earth Science 7: Answer Sheet Module 5: Solar EclipseDocument2 pages4 Quarter - Earth Science 7: Answer Sheet Module 5: Solar Eclipsevincent baltazarNo ratings yet
- Answer Sheet: Module 1: Week 1-2: Respiratory and Circulatory Systems Working With The Other Organ SystemsDocument3 pagesAnswer Sheet: Module 1: Week 1-2: Respiratory and Circulatory Systems Working With The Other Organ SystemsCristina AguinaldoNo ratings yet
- Brooke'S Point Central School Grade Iv-Answer Sheet Quarter 1 Week 3-Module 3Document4 pagesBrooke'S Point Central School Grade Iv-Answer Sheet Quarter 1 Week 3-Module 3ABBYLENNE MALONGNo ratings yet
- Name: Section:: Health Quarter 2 - Module Answer SheetDocument9 pagesName: Section:: Health Quarter 2 - Module Answer SheetKristine Joy Perez - CapiliNo ratings yet
- 1st Quarter Week 6 Answer SheetDocument3 pages1st Quarter Week 6 Answer SheetKrisna Laine MalazarteNo ratings yet
- Answer-Sheet-Q2-Week-3 BonifacioDocument3 pagesAnswer-Sheet-Q2-Week-3 BonifacioMhin MhinNo ratings yet
- Absentee Report Grade 10-St - Paul The Apostle Absentee Report Grade 10-St - Paul The ApostleDocument2 pagesAbsentee Report Grade 10-St - Paul The Apostle Absentee Report Grade 10-St - Paul The ApostleMary Joy Corpuz PiamonteNo ratings yet
- Learner's Learning Log Week 6Document10 pagesLearner's Learning Log Week 6Reggie AbañoNo ratings yet
- School Holiday Writing Practice: A Practice A Day, Keeps The E Away!Document8 pagesSchool Holiday Writing Practice: A Practice A Day, Keeps The E Away!Ct QihahNo ratings yet
- Quarter 2 Module 5Document4 pagesQuarter 2 Module 5Glenda Manalo Coching50% (2)
- Answer SheetDocument1 pageAnswer SheetZachary B. AndersonNo ratings yet
- PE AND HEALTH - QUIZ NO 2 4thDocument2 pagesPE AND HEALTH - QUIZ NO 2 4thMelben ResurreccionNo ratings yet
- Answer Sheet in Tle 7 Food Fish Processing EditedDocument4 pagesAnswer Sheet in Tle 7 Food Fish Processing EditedNildwen UrbiztondoNo ratings yet
- Smaw As 1Document6 pagesSmaw As 1MAY ANN CATIPONNo ratings yet
- Apeh 9 - Answersheet NAME: - GRADE & SECTIONDocument2 pagesApeh 9 - Answersheet NAME: - GRADE & SECTIONElmer john de LeonNo ratings yet
- Week 4 ANSWER SHEET REVISEDDocument4 pagesWeek 4 ANSWER SHEET REVISEDKenji ToleroNo ratings yet
- Laboratory Checklist in Bread and Pastry: Pedro Guevara Memorial National High SchoolDocument4 pagesLaboratory Checklist in Bread and Pastry: Pedro Guevara Memorial National High SchoolJohnmathew LastimosaNo ratings yet
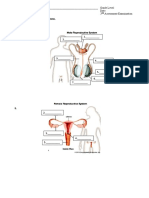
- Reproductive SystemDocument1 pageReproductive SystemKathleen Ann NarismaNo ratings yet
- WinterSpelling 1Document10 pagesWinterSpelling 1Citra Dwi JuniarNo ratings yet
- As Q2M5Document4 pagesAs Q2M5Glenda Manalo CochingNo ratings yet
- Lesson 1: Identifying The Different Sources of Information: What I KnowDocument4 pagesLesson 1: Identifying The Different Sources of Information: What I KnowGerome ZamoraNo ratings yet
- SCIENCE 8 Answer SheetDocument2 pagesSCIENCE 8 Answer SheetAndrewdKiatKiatNo ratings yet
- Complete Module UTSDocument112 pagesComplete Module UTSRafael ChuaNo ratings yet
- Robert Abiol-Grade 12 Contemporary Arts-Answer SheetsDocument6 pagesRobert Abiol-Grade 12 Contemporary Arts-Answer SheetsRobert KaneNo ratings yet
- ABM Module 4Document2 pagesABM Module 4Jessarine Rose Ocay CastillonNo ratings yet
- End of Year OrganiserDocument12 pagesEnd of Year Organiserandrea.maitaNo ratings yet
- Mind Map /step ForwardDocument6 pagesMind Map /step ForwardRodrigo PeñaNo ratings yet
- Answer Sheet Eng 9Document1 pageAnswer Sheet Eng 9Nate WagaNo ratings yet
- Answer Sheet Week 7Document4 pagesAnswer Sheet Week 7Joyahj Yahj MysticaNo ratings yet
- First Grading Period Name: - Section: - Second Grading Period Name: - SectionDocument2 pagesFirst Grading Period Name: - Section: - Second Grading Period Name: - SectionSofia Añes BaloisNo ratings yet
- Answer Sheet Template - AndrewDocument193 pagesAnswer Sheet Template - AndrewArthur BenecarioNo ratings yet
- FILIPINO 8 Module 5&6Document2 pagesFILIPINO 8 Module 5&6Romeo AvancenaNo ratings yet
- Biome Self EvaluationDocument2 pagesBiome Self Evaluationapi-339858812No ratings yet
- Earth and Life Science: Answer SheetDocument8 pagesEarth and Life Science: Answer SheetGaspar Jr CantereNo ratings yet
- Contemporary Philippine Arts From The Region: Answer SheetDocument1 pageContemporary Philippine Arts From The Region: Answer Sheetbernadette albino100% (2)
- Answersheet 7 M&a Q1Document4 pagesAnswersheet 7 M&a Q1Elmer john de LeonNo ratings yet
- What Color Is ItDocument1 pageWhat Color Is ItJonathan McCarthyNo ratings yet
- Find The Words WorksheetDocument1 pageFind The Words WorksheetJonathan McCarthyNo ratings yet
- What Do They Do WorksheetDocument1 pageWhat Do They Do WorksheetJonathan McCarthyNo ratings yet
- Fireplace Menu UpdateDocument2 pagesFireplace Menu UpdateJonathan McCarthyNo ratings yet
- Demo Material 210708Document38 pagesDemo Material 210708Jonathan McCarthyNo ratings yet
- Fireplace Menu UpdateDocument2 pagesFireplace Menu UpdateJonathan McCarthyNo ratings yet