You might also like
- CASE STUDY Bronchial AsthmaDocument6 pagesCASE STUDY Bronchial AsthmaRichelle Sandriel C. de Castro86% (22)
- JMD PPH Critical Thinking Map-1Document1 pageJMD PPH Critical Thinking Map-1api-417952873No ratings yet
- Example Personal StatementsDocument22 pagesExample Personal Statementsstarblue265100% (1)
- Social Work MaterialDocument214 pagesSocial Work MaterialBala Tvn100% (2)
- The Good-Enough Sex Model For Couple Sexual SatisfactionDocument13 pagesThe Good-Enough Sex Model For Couple Sexual SatisfactionwernikNo ratings yet
- Individual CounselingDocument7 pagesIndividual CounselingCarla Dela CruzNo ratings yet
- PediatricDocument98 pagesPediatricNisreen Al-shareNo ratings yet
- Handout OB MidtermsDocument3 pagesHandout OB Midtermsaidan valin100% (7)
- Case Conference July 25 2017Document41 pagesCase Conference July 25 2017dhania patraNo ratings yet
- Congenital SyphilisDocument28 pagesCongenital SyphilisMeena Koushal100% (4)
- Neonatology and Puerperium HYDocument6 pagesNeonatology and Puerperium HYOccamsRazorNo ratings yet
- Viral ExanthemDocument18 pagesViral ExanthemRajesh Kumar AsunalaNo ratings yet
- Pediatrics: by DR - Mohammad Z. Abu Sheikha@Document101 pagesPediatrics: by DR - Mohammad Z. Abu Sheikha@صقر حوران100% (1)
- Pediatrics: by DR - Mohammad Z. Abu Sheikha@Document98 pagesPediatrics: by DR - Mohammad Z. Abu Sheikha@Mohamed AbbasNo ratings yet
- ميحرلا نمحرلا الله مسب Birth InjuryDocument45 pagesميحرلا نمحرلا الله مسب Birth InjuryhassanunderstandNo ratings yet
- Cerebral PalsyDocument9 pagesCerebral PalsyAngy100% (2)
- Omphalitis LectureDocument18 pagesOmphalitis LectureWonyenghitari George0% (1)
- PediaDocument43 pagesPediaRahaf Bin ManieNo ratings yet
- PROM ApproachDocument3 pagesPROM Approachعبد الله الحربيNo ratings yet
- Abnormalities of The Puerperium: Puerperal PyrexiaDocument28 pagesAbnormalities of The Puerperium: Puerperal Pyrexiadrravindermehetrey100% (2)
- 4485 16580 2 PBDocument4 pages4485 16580 2 PBishu sNo ratings yet
- Well and Goes To Party. Develops Coughing Fit and Goes Blue and Then Everything Is Okay. 36Document8 pagesWell and Goes To Party. Develops Coughing Fit and Goes Blue and Then Everything Is Okay. 36Dean HarrisonNo ratings yet
- OB 2 TermsDocument4 pagesOB 2 TermsDragana AbramovicNo ratings yet
- PWH - NotesDocument140 pagesPWH - NotesjNo ratings yet
- Neuro Lo Week 1 - 1 DraftDocument15 pagesNeuro Lo Week 1 - 1 DraftMarcellina AwingNo ratings yet
- Pediatrics NotesDocument100 pagesPediatrics Notessanflash100% (1)
- HY USMLE Review Part IVDocument31 pagesHY USMLE Review Part IVDr.2020100% (1)
- Pediatrics PearlsDocument74 pagesPediatrics PearlsuowhywxuuiragjadchNo ratings yet
- Chapter IIIDocument6 pagesChapter IIIJoshua SitorusNo ratings yet
- Neuro SGDocument29 pagesNeuro SGgew123No ratings yet
- Death Case Report Februari 25 2021 A 1 Year 6 Months Old Girl With Langerhans Cell Hystiocytosis and Its ComplicationDocument11 pagesDeath Case Report Februari 25 2021 A 1 Year 6 Months Old Girl With Langerhans Cell Hystiocytosis and Its ComplicationVianNo ratings yet
- Pediatrics Nursing DisordersDocument9 pagesPediatrics Nursing DisordersAli IgnacioNo ratings yet
- Neonatal SepsisDocument38 pagesNeonatal SepsisJavier Saad100% (1)
- Neuro Form 1Document2 pagesNeuro Form 1skylar0% (1)
- Abdul Hakeem Hady.: Done byDocument29 pagesAbdul Hakeem Hady.: Done byعمر احمد شاكرNo ratings yet
- NRS Review Notes - Pedia 2Document8 pagesNRS Review Notes - Pedia 2Mariecar GarazaNo ratings yet
- Nclex Notes 1Document17 pagesNclex Notes 1itokumo100% (2)
- Notes in Pediatrics. 2 Ed. 2001/02 Senior & Junior Peds RotationsDocument18 pagesNotes in Pediatrics. 2 Ed. 2001/02 Senior & Junior Peds Rotationsopis08100% (1)
- Pediatrics Study GuideDocument22 pagesPediatrics Study GuideElizabeth McKee100% (1)
- Pediatrics Clerkship Shelf ReviewDocument78 pagesPediatrics Clerkship Shelf Reviewlcaskidsn12s100% (1)
- Hayats ResponsesDocument18 pagesHayats Responsesyacineone01No ratings yet
- Obstructed Labor: Basliel E. (MD)Document12 pagesObstructed Labor: Basliel E. (MD)Asteway MesfinNo ratings yet
- Newborn History TakingDocument9 pagesNewborn History TakingpriyankasekarNo ratings yet
- Informant: Grandmother (70 %) Reliability General DataDocument8 pagesInformant: Grandmother (70 %) Reliability General Dataemely p. tangoNo ratings yet
- NewbornDocument3 pagesNewbornimnashNo ratings yet
- High Yield - Bacteriology ChartsDocument9 pagesHigh Yield - Bacteriology ChartsAmirsalar EslamiNo ratings yet
- Pediatrics NCM 109Document26 pagesPediatrics NCM 109Gezabelle SalveNo ratings yet
- Feb 19. CA 2 - 1681737641118Document9 pagesFeb 19. CA 2 - 1681737641118HANNAH BANGKILINGNo ratings yet
- ECLAMPSIA EditedDocument47 pagesECLAMPSIA EditedKharisma Gita Kartika sariNo ratings yet
- Neonatal NotesDocument34 pagesNeonatal Notesgridchan100% (2)
- Abortion (Miscarrage)Document46 pagesAbortion (Miscarrage)escalatorNo ratings yet
- Placenta Previa Case StudyDocument7 pagesPlacenta Previa Case StudyKing NavsunNo ratings yet
- Pregnancy Induced HypertensionDocument4 pagesPregnancy Induced HypertensioncfgrtwifhNo ratings yet
- 2 Nursing Care of The Pregnant Client Gestational ConditionDocument120 pages2 Nursing Care of The Pregnant Client Gestational ConditionjustinjareddNo ratings yet
- Obs WrittenDocument21 pagesObs WrittenHeno FayizNo ratings yet
- Week 13 - Vid Lec 1-3 Sir GerryDocument10 pagesWeek 13 - Vid Lec 1-3 Sir Gerryjmmacar19No ratings yet
- Physiology for General Surgical Sciences Examination (GSSE)From EverandPhysiology for General Surgical Sciences Examination (GSSE)S. Ali MirjaliliNo ratings yet
- Guide to Pediatric Urology and Surgery in Clinical PracticeFrom EverandGuide to Pediatric Urology and Surgery in Clinical PracticeNo ratings yet
- Dermatology Notes for Medical StudentsFrom EverandDermatology Notes for Medical StudentsRating: 4 out of 5 stars4/5 (5)
- Pedia PE GuideDocument9 pagesPedia PE GuideCarlos NiñoNo ratings yet
- Lumbar Tap - Procedure, Indications, Contraindications - Analysis of Normal CSF ResultsDocument4 pagesLumbar Tap - Procedure, Indications, Contraindications - Analysis of Normal CSF ResultsCarlos NiñoNo ratings yet
- SGD For NCD and Disease Occurrence: MD1-1 Group 4Document4 pagesSGD For NCD and Disease Occurrence: MD1-1 Group 4Carlos NiñoNo ratings yet
- PHYSIO Prelims SamplexDocument11 pagesPHYSIO Prelims SamplexCarlos NiñoNo ratings yet
- Hypertensive DietDocument6 pagesHypertensive DietCarlos NiñoNo ratings yet
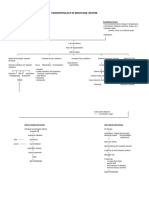
- Pathophysiology of Bronchial AsthmaDocument2 pagesPathophysiology of Bronchial AsthmaCarlos NiñoNo ratings yet
- Severe Headache: Clinical Manifestations: LOC, GCS 3, Anisocoric Pupils, Very Minimal Eyelid Movements To CornealDocument1 pageSevere Headache: Clinical Manifestations: LOC, GCS 3, Anisocoric Pupils, Very Minimal Eyelid Movements To CornealCarlos NiñoNo ratings yet
- Innate Immune Response: Defensins - Most Abundant Antimicrobial Peptides That Kill Bacteria (G+ andDocument5 pagesInnate Immune Response: Defensins - Most Abundant Antimicrobial Peptides That Kill Bacteria (G+ andCarlos NiñoNo ratings yet
- Pharmacology Long Exam 1 2 Yr - 2 Sem 2016: ND NDDocument2 pagesPharmacology Long Exam 1 2 Yr - 2 Sem 2016: ND NDCarlos NiñoNo ratings yet
- RespiDocument3 pagesRespiCarlos NiñoNo ratings yet
- Hypoglycemic Effect of Catharantus Roseus (Tsitsirika) Against Albino RabbitsDocument2 pagesHypoglycemic Effect of Catharantus Roseus (Tsitsirika) Against Albino RabbitsCarlos NiñoNo ratings yet
- Hypoglycemic Effect of Catharantus Roseus (Tsitsirika) Against Albino RabbitsDocument2 pagesHypoglycemic Effect of Catharantus Roseus (Tsitsirika) Against Albino RabbitsCarlos NiñoNo ratings yet
- Gross Anats Presem ReviewDocument14 pagesGross Anats Presem ReviewCarlos NiñoNo ratings yet
- Le Ga 1Document15 pagesLe Ga 1Carlos NiñoNo ratings yet
- Biochem3 Amino AcidsDocument3 pagesBiochem3 Amino AcidsCarlos NiñoNo ratings yet
- Syllabi For Basic PharmacologyDocument1 pageSyllabi For Basic PharmacologyCarlos NiñoNo ratings yet
- Officinale) Which Exhibited Its Anti-Angiogenic Property by Decreasing The CAMDocument2 pagesOfficinale) Which Exhibited Its Anti-Angiogenic Property by Decreasing The CAMCarlos NiñoNo ratings yet
- Pharmacology Long Exam 1 2 Yr - 2 Sem 2016: ND NDDocument2 pagesPharmacology Long Exam 1 2 Yr - 2 Sem 2016: ND NDCarlos NiñoNo ratings yet
- Officinale) Which Exhibited Its Anti-Angiogenic Property by Decreasing The CAMDocument2 pagesOfficinale) Which Exhibited Its Anti-Angiogenic Property by Decreasing The CAMCarlos NiñoNo ratings yet
- Hypertensive DietDocument6 pagesHypertensive DietCarlos NiñoNo ratings yet
- Carlos D. Achondo Jr. 2MD-1Document4 pagesCarlos D. Achondo Jr. 2MD-1Carlos NiñoNo ratings yet
- Histo Path PUDDocument1 pageHisto Path PUDCarlos NiñoNo ratings yet
- Higher Cortical FunctionsDocument2 pagesHigher Cortical FunctionsCarlos NiñoNo ratings yet
- Glasgow Coma ScaleDocument2 pagesGlasgow Coma Scalejean thereseNo ratings yet
- Gross Anats Presem ReviewDocument14 pagesGross Anats Presem ReviewCarlos NiñoNo ratings yet
- Histo CardioDocument12 pagesHisto CardioCarlos NiñoNo ratings yet
- In Schools Needed Say CampaignersDocument11 pagesIn Schools Needed Say CampaignersCarlos NiñoNo ratings yet
- CSR Activities by TATADocument13 pagesCSR Activities by TATAMegha VaruNo ratings yet
- Small TalkDocument2 pagesSmall TalkHerdeiro DicaprioNo ratings yet
- 2022 Arihant Political Science MCQs Term-1 Sample PapersDocument192 pages2022 Arihant Political Science MCQs Term-1 Sample PapersImran Arshad100% (4)
- Laboratory Result Report: Requested Test Result Units Reference Value Method ImmunologyDocument1 pageLaboratory Result Report: Requested Test Result Units Reference Value Method ImmunologyYaya ZakariaNo ratings yet
- Life-Long Learning Characteristics Self-Assessment: Behavioral IndicatorsDocument2 pagesLife-Long Learning Characteristics Self-Assessment: Behavioral Indicatorsapi-534534107No ratings yet
- HSMAI PHG - New Rules To Be Market ReadyDocument28 pagesHSMAI PHG - New Rules To Be Market ReadyAnna ShortNo ratings yet
- Absorption, Distribution, Metabolism, Excretion and Mechanisms of Action of AflatoxinsDocument3 pagesAbsorption, Distribution, Metabolism, Excretion and Mechanisms of Action of AflatoxinsMaya Innaka ArhayuNo ratings yet
- Weld-On 4 MsdsDocument2 pagesWeld-On 4 MsdsJosué CubilloNo ratings yet
- Cut-Off Points For Admission Under The Government Sponsorship Scheme For The Academic Year 2015/2016.Document4 pagesCut-Off Points For Admission Under The Government Sponsorship Scheme For The Academic Year 2015/2016.The Campus Times100% (1)
- Hypo - RT PC TrialDocument37 pagesHypo - RT PC TrialnitinNo ratings yet
- Nerve Injuries: Radial Nerve, Median Nerve and Ulnar NerveDocument26 pagesNerve Injuries: Radial Nerve, Median Nerve and Ulnar NerveaisiyaahNo ratings yet
- Identifikasi Dan Prevalensi Nematoda Saluran Pencernaan Kuda Lokal (Equus Caballus) Di Kecamatan Moyo Hilir SumbawaDocument7 pagesIdentifikasi Dan Prevalensi Nematoda Saluran Pencernaan Kuda Lokal (Equus Caballus) Di Kecamatan Moyo Hilir SumbawaBeebli PuchaNo ratings yet
- The Miracle of ChocolateDocument10 pagesThe Miracle of ChocolateAmanda YasminNo ratings yet
- 12 2012 TriclabendazoleDocument16 pages12 2012 Triclabendazolenia suwartiningsihNo ratings yet
- Blood TypingDocument11 pagesBlood Typingprakash gusainNo ratings yet
- IELTS 1 Test IntroDocument1 pageIELTS 1 Test IntromichaelNo ratings yet
- Laminar AirflowDocument15 pagesLaminar AirflowKamran AshrafNo ratings yet
- Junal 1Document6 pagesJunal 1indadzi arsyNo ratings yet
- Book StickerDocument4 pagesBook Stickerilanabiela90No ratings yet
- Bakery Business PlanDocument31 pagesBakery Business PlanRohit Gupta93% (14)
- H. Pylori IgA ELISA Package InsertDocument2 pagesH. Pylori IgA ELISA Package Inserttalha saleemNo ratings yet
- Annual Report of NHRC (2016-17)Document240 pagesAnnual Report of NHRC (2016-17)Shruti Nagvanshi100% (1)
- Playlist AssignmentDocument7 pagesPlaylist AssignmentTimothy Matthew JohnstoneNo ratings yet
- Culture Negative IsDocument29 pagesCulture Negative IsvinobapsNo ratings yet
- Bertam ProfileDocument8 pagesBertam ProfilesadassanNo ratings yet
- Villegas Lucero 1Document8 pagesVillegas Lucero 1api-213921706No ratings yet
- Points To Be DiscussedDocument4 pagesPoints To Be DiscussedShalini ShekharNo ratings yet