You might also like
- Written Assignment Principles of Applied Rehabilitation - EditedDocument17 pagesWritten Assignment Principles of Applied Rehabilitation - EditedRuqaiyah RahmanNo ratings yet
- Spiritual Assessment in Social Work and Mental Health PracticeFrom EverandSpiritual Assessment in Social Work and Mental Health PracticeNo ratings yet
- Written Assignment Principles of Applied RehabilitationDocument17 pagesWritten Assignment Principles of Applied RehabilitationRuqaiyah RahmanNo ratings yet
- Hospitalization EditedDocument6 pagesHospitalization EditedmercyNo ratings yet
- Nurse Role To Imporve Lives of People With LDDocument11 pagesNurse Role To Imporve Lives of People With LDDave MangeshNo ratings yet
- Physiotherapists' Views, Perceived Knowledge, and Reported Use of Psychosocial Strategies in PracticeDocument16 pagesPhysiotherapists' Views, Perceived Knowledge, and Reported Use of Psychosocial Strategies in PracticeDoctor MemiNo ratings yet
- Older Adults and Integrated Health Settings: Opportunities and Challenges For Mental Health CounselorsDocument15 pagesOlder Adults and Integrated Health Settings: Opportunities and Challenges For Mental Health CounselorsGabriela SanchezNo ratings yet
- THE ROLE OF OCCUPATONAL THERAPY IN THE RECOVERY OF PATIENTS IN BUTABIKA HOSPITAL (AutoRecovered)Document41 pagesTHE ROLE OF OCCUPATONAL THERAPY IN THE RECOVERY OF PATIENTS IN BUTABIKA HOSPITAL (AutoRecovered)samuelNo ratings yet
- How Can We Improve Medical EducationDocument9 pagesHow Can We Improve Medical EducationJOMARI MANALONo ratings yet
- 4-Emotional Freedom Techniques (EFT) As A Practice For Supporting Chronic Disease Healthcare A Practitioners' PerspectiveDocument10 pages4-Emotional Freedom Techniques (EFT) As A Practice For Supporting Chronic Disease Healthcare A Practitioners' PerspectiveFria ZafriaNo ratings yet
- Intervenciones en Rehabilitación Psiquiátrica - RevisiónDocument17 pagesIntervenciones en Rehabilitación Psiquiátrica - RevisiónpsychforallNo ratings yet
- Document 2 - The Biopsychosocial Model of Mental HealthDocument3 pagesDocument 2 - The Biopsychosocial Model of Mental Healthjefel umarNo ratings yet
- Alligood and Tomey (2010) : in Addition To DevelopingDocument2 pagesAlligood and Tomey (2010) : in Addition To DevelopingSheen AponNo ratings yet
- NR527 Module 3 (Health Promotion)Document5 pagesNR527 Module 3 (Health Promotion)96rubadiri96No ratings yet
- RUNNING HEAD: Middle Range Theories 1 Middle Range Theory Utilization and Application Paper Group 1 (Names of Group Members)Document8 pagesRUNNING HEAD: Middle Range Theories 1 Middle Range Theory Utilization and Application Paper Group 1 (Names of Group Members)Sebastian Morris KiambaNo ratings yet
- Wampole 2020Document17 pagesWampole 2020rafaelcaloca1No ratings yet
- Lit ReviewDocument7 pagesLit ReviewNene onetwoNo ratings yet
- B. Occupational Therapy (Hons.) : Faculty of Health Sciences Universiti Teknologi MaraDocument3 pagesB. Occupational Therapy (Hons.) : Faculty of Health Sciences Universiti Teknologi MaraSiti Nur Hafidzoh OmarNo ratings yet
- Topic Title - Reflective EssayDocument12 pagesTopic Title - Reflective EssayBlessing N. Ikiseh (Bibieandrea)No ratings yet
- COMMUNITY HEALTH NURSING CONCEPTS Topic 2Document25 pagesCOMMUNITY HEALTH NURSING CONCEPTS Topic 2Ciedelle Honey Lou DimaligNo ratings yet
- Dolor Lumbar en Estudiantes Del Area de SaludDocument15 pagesDolor Lumbar en Estudiantes Del Area de Saludhansel nainNo ratings yet
- Community Health Nursing Approaches ExplainedDocument22 pagesCommunity Health Nursing Approaches Explainedkles insgkk100% (1)
- Analysis of Pender's Health Promotion Model: Context and Content of The TheoryDocument9 pagesAnalysis of Pender's Health Promotion Model: Context and Content of The TheoryAsih Siti SundariNo ratings yet
- Approaches to Rehabilitation ModelsDocument11 pagesApproaches to Rehabilitation ModelsBijal ShahNo ratings yet
- Health Psychology VS Biomedical KnowledgeDocument17 pagesHealth Psychology VS Biomedical KnowledgeVenice LaufeysonNo ratings yet
- Main Article For Publication-Biopsychosocial-SpiritualDocument12 pagesMain Article For Publication-Biopsychosocial-SpiritualSuantak D VaipheiNo ratings yet
- Patient Self-Management Discussion PaperDocument13 pagesPatient Self-Management Discussion PaperDefi DestyawenyNo ratings yet
- Resilience and Mental Health NursingDocument15 pagesResilience and Mental Health NursingDWNo ratings yet
- Narganes Matias Arguello 1909319 Hs2135 ScriptDocument11 pagesNarganes Matias Arguello 1909319 Hs2135 ScriptMatías ArgüelloNo ratings yet
- Mental Health Literacy - Help Seeking Behaviour - UK CoachesDocument14 pagesMental Health Literacy - Help Seeking Behaviour - UK CoachesKumala WindyaNo ratings yet
- Systems Research and Behavioral Science - 2020 - Tramonti - Systems thinking and the biopsychosocial approach A multilevelDocument16 pagesSystems Research and Behavioral Science - 2020 - Tramonti - Systems thinking and the biopsychosocial approach A multilevelMarta MatosNo ratings yet
- Nola PenderDocument9 pagesNola PenderSheen Apon100% (2)
- Nursing Holistic Care ApproachDocument13 pagesNursing Holistic Care ApproachBrian MisungaNo ratings yet
- What Is Occupational Therapy PaperDocument12 pagesWhat Is Occupational Therapy Paperangelalvarezk6No ratings yet
- Healing Environment Self-Reflection PaperDocument9 pagesHealing Environment Self-Reflection Paperapi-336005635No ratings yet
- The Role of Psychologists in Health Care DeliveryDocument8 pagesThe Role of Psychologists in Health Care DeliveryRain RivertonNo ratings yet
- Proposed 2Document4 pagesProposed 2Isaac AffamNo ratings yet
- Special7 Paper 07Document18 pagesSpecial7 Paper 07Mc KeteqmanNo ratings yet
- Research Papers Health Promotion ModelDocument6 pagesResearch Papers Health Promotion Modelafnkyarofeepzh100% (1)
- 5HW047 - Holistic Approaches To Healthcare - Assignment LayoutDocument15 pages5HW047 - Holistic Approaches To Healthcare - Assignment LayoutVicky RobiNo ratings yet
- Person Centered Care Literature ReviewDocument4 pagesPerson Centered Care Literature Reviewafdtaeczo100% (1)
- Introduction to Health and Social Care ProfessionalsDocument16 pagesIntroduction to Health and Social Care ProfessionalsojogoddyNo ratings yet
- Basic Concepts in NursingDocument13 pagesBasic Concepts in Nursingbleuspirit2011No ratings yet
- Health Psychology Case StudyDocument18 pagesHealth Psychology Case StudyVenice LaufeysonNo ratings yet
- Definition of Biomedical Model of HealthDocument4 pagesDefinition of Biomedical Model of Healthتالیہ مرادNo ratings yet
- Psikolojik İlk Yardım Amaçları, Uygulanışı, Hassas Gruplar Ve Uyulması Gereken Etik KurallarDocument13 pagesPsikolojik İlk Yardım Amaçları, Uygulanışı, Hassas Gruplar Ve Uyulması Gereken Etik KurallarCeren ÖZERNo ratings yet
- Health and Wellness Thesis StatementDocument7 pagesHealth and Wellness Thesis Statementafbteuawc100% (2)
- Participation Motives, Health Awareness, and Physical Well-beingDocument90 pagesParticipation Motives, Health Awareness, and Physical Well-beingMalaica NinaNo ratings yet
- Baer, R., Crane, C., Miller, E., Kuyken, W. (2019) - Doing No Harm in Mindfulness-Based Programs Conceptual Issues and Empirical Findings.Document14 pagesBaer, R., Crane, C., Miller, E., Kuyken, W. (2019) - Doing No Harm in Mindfulness-Based Programs Conceptual Issues and Empirical Findings.kbmatekNo ratings yet
- Health Promotion Planning: An Educational and Environmental ApproachDocument1 pageHealth Promotion Planning: An Educational and Environmental Approachjihan rahmadany100% (1)
- Person Centred Care Literature ReviewDocument8 pagesPerson Centred Care Literature Reviewnidokyjynuv2100% (1)
- Week 4 NewDocument7 pagesWeek 4 NewMN KhanNo ratings yet
- Order ID 3515930Document6 pagesOrder ID 3515930Nick Ole-GichuruNo ratings yet
- 1 s2.0 S2590109523000058 MainDocument9 pages1 s2.0 S2590109523000058 MainJonathan IbañezNo ratings yet
- Nu707 m4 - Models and Theories of Nursing Goals and FunctionsDocument5 pagesNu707 m4 - Models and Theories of Nursing Goals and Functionsapi-577441503No ratings yet
- Out 175Document7 pagesOut 175Anonymous 75TDy2yNo ratings yet
- Conceptual FrameworkDocument5 pagesConceptual FrameworkhoneyNo ratings yet
- Psychosocial Rehabilitation WordDocument11 pagesPsychosocial Rehabilitation WordPutri Kadashi UtamiNo ratings yet
- Smoking and Alcohol Counselingv2.1Document18 pagesSmoking and Alcohol Counselingv2.1Angelo HuligangaNo ratings yet
- Defining Community in Social Sciences (40Document13 pagesDefining Community in Social Sciences (40Aivan Luke PaloyoNo ratings yet
- 6 Min English Bucket ListsDocument5 pages6 Min English Bucket ListssNo ratings yet
- Rate List - IGIMS PDFDocument47 pagesRate List - IGIMS PDFShashank SoniNo ratings yet
- Vocabulary UNIT - 3 - : - Free Times - GRAMMAR: - Can/Can T For Ability, Like + Verb/nounDocument4 pagesVocabulary UNIT - 3 - : - Free Times - GRAMMAR: - Can/Can T For Ability, Like + Verb/nounRicardo JimenezNo ratings yet
- CharittyDocument2 pagesCharittyGeorge EduardNo ratings yet
- Definitions: The Social Determinants of Health. SummaryDocument4 pagesDefinitions: The Social Determinants of Health. SummaryS VaibhavNo ratings yet
- Summary, Conclusion, Implications and RecommendationDocument6 pagesSummary, Conclusion, Implications and RecommendationJubert IlosoNo ratings yet
- Biological, Chemical and Radiological Terrorism - Emergency Preparedness and Response For The Primary Care Physician - Springer (PDFDrive)Document270 pagesBiological, Chemical and Radiological Terrorism - Emergency Preparedness and Response For The Primary Care Physician - Springer (PDFDrive)Manuel MartinezNo ratings yet
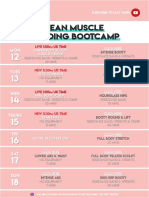
- 26 - LEAN Weekly Guide - On - October 12Document15 pages26 - LEAN Weekly Guide - On - October 12Andrea CsillaNo ratings yet
- (Journal of Neurosurgery - Spine) Radiographic and Clinical Evaluation of Free-Hand Placement of C-2 Pedicle ScrewsDocument8 pages(Journal of Neurosurgery - Spine) Radiographic and Clinical Evaluation of Free-Hand Placement of C-2 Pedicle ScrewsVeronica Mtz ZNo ratings yet
- Session 3 Creating A Positive Workplace For Employee Mental Health FINALDocument27 pagesSession 3 Creating A Positive Workplace For Employee Mental Health FINALMYRA GONZALESNo ratings yet
- 6 Day Supermodel Slimdown Plan Brazil Butt LiftDocument6 pages6 Day Supermodel Slimdown Plan Brazil Butt LiftAlina Trofim100% (2)
- Team 1's Quantitative ApproachesDocument46 pagesTeam 1's Quantitative ApproachesDIANA ALLISON QUINONES JAUREGUINo ratings yet
- Turn Table - LLT-750Document29 pagesTurn Table - LLT-750Sadashiva sahooNo ratings yet
- TFN-Theoretical Foundation in Nursing Reflection Paper: The Core Care Values of A Beginning HOLYNAMIAN Servant Leader Student NurseDocument2 pagesTFN-Theoretical Foundation in Nursing Reflection Paper: The Core Care Values of A Beginning HOLYNAMIAN Servant Leader Student NurseDanica Rose PalacaNo ratings yet
- 2.12 ICS Forms ICS 206Document3 pages2.12 ICS Forms ICS 206mdrrmo sinait100% (1)
- Business, Government & Society: Definitions Relationships ModelsDocument20 pagesBusiness, Government & Society: Definitions Relationships ModelsNajabat Ali RanaNo ratings yet
- HRM Practices in RMG Industry in Bangladesh: NexusDocument28 pagesHRM Practices in RMG Industry in Bangladesh: NexusFahimNo ratings yet
- Re Beacon Conference MeetingDocument11 pagesRe Beacon Conference MeetingjohnsherwieNo ratings yet
- QED Achieves 1 Million Safe ManhoursDocument2 pagesQED Achieves 1 Million Safe ManhoursBernabe AlmirolNo ratings yet
- Pulmonary Tuberculosis - Curitana BSN 2bDocument10 pagesPulmonary Tuberculosis - Curitana BSN 2bDrex CuritanaNo ratings yet
- Case Report OperkulektomiDocument6 pagesCase Report OperkulektomiYuliya Zalma Noor AzizahNo ratings yet
- Ipratropium Salbutamol (DUAVENT)Document2 pagesIpratropium Salbutamol (DUAVENT)Kristine Young100% (2)
- Creating Effective Teams Week 11 LessonDocument4 pagesCreating Effective Teams Week 11 LessonEll VNo ratings yet
- Neural Network and Social NetworkDocument18 pagesNeural Network and Social NetworkMariannZinampanNo ratings yet
- ReportDocument1 pageReportAaRvi RvNo ratings yet
- Retype PDFDocument18 pagesRetype PDFrubel39islamNo ratings yet
- Guide Sports and Games - Around The WorldDocument29 pagesGuide Sports and Games - Around The WorldJoseph VEGANo ratings yet
- Temporal Lobe Memory & Psychiatric SymptomsDocument13 pagesTemporal Lobe Memory & Psychiatric SymptomsSami MdNo ratings yet
- Save Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryFrom EverandSave Me from Myself: How I Found God, Quit Korn, Kicked Drugs, and Lived to Tell My StoryNo ratings yet
- Healing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildFrom EverandHealing Your Aloneness: Finding Love and Wholeness Through Your Inner ChildRating: 3.5 out of 5 stars3.5/5 (9)
- The Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsFrom EverandThe Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsNo ratings yet
- Stop Drinking Now: The original Easyway methodFrom EverandStop Drinking Now: The original Easyway methodRating: 5 out of 5 stars5/5 (28)
- Easyway Express: Stop Smoking and Quit E-CigarettesFrom EverandEasyway Express: Stop Smoking and Quit E-CigarettesRating: 5 out of 5 stars5/5 (15)
- Breaking Addiction: A 7-Step Handbook for Ending Any AddictionFrom EverandBreaking Addiction: A 7-Step Handbook for Ending Any AddictionRating: 4.5 out of 5 stars4.5/5 (2)
- The Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionFrom EverandThe Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionRating: 5 out of 5 stars5/5 (63)
- Allen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductFrom EverandAllen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductRating: 5 out of 5 stars5/5 (31)
- Alcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousFrom EverandAlcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousRating: 5 out of 5 stars5/5 (22)
- Allen Carr's Easy Way to Quit Smoking Without Willpower: The best-selling quit smoking method updated for the 21st centuryFrom EverandAllen Carr's Easy Way to Quit Smoking Without Willpower: The best-selling quit smoking method updated for the 21st centuryRating: 5 out of 5 stars5/5 (47)
- Breathing Under Water: Spirituality and the Twelve StepsFrom EverandBreathing Under Water: Spirituality and the Twelve StepsRating: 4.5 out of 5 stars4.5/5 (41)
- Allen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerFrom EverandAllen Carr's Quit Drinking Without Willpower: Be a happy nondrinkerRating: 5 out of 5 stars5/5 (8)
- Drunk-ish: A Memoir of Loving and Leaving AlcoholFrom EverandDrunk-ish: A Memoir of Loving and Leaving AlcoholRating: 4 out of 5 stars4/5 (6)
- Stop Smoking with Allen Carr: Includes 70 minute audio epilogue read by AllenFrom EverandStop Smoking with Allen Carr: Includes 70 minute audio epilogue read by AllenRating: 5 out of 5 stars5/5 (61)
- Twelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingFrom EverandTwelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingRating: 5 out of 5 stars5/5 (11)
- Smart Phone Dumb Phone: Free Yourself from Digital AddictionFrom EverandSmart Phone Dumb Phone: Free Yourself from Digital AddictionRating: 5 out of 5 stars5/5 (11)
- Sober Curious: The Blissful Sleep, Greater Focus, Limitless Presence, and Deep Connection Awaiting Us All on the Other Side of AlcoholFrom EverandSober Curious: The Blissful Sleep, Greater Focus, Limitless Presence, and Deep Connection Awaiting Us All on the Other Side of AlcoholRating: 4.5 out of 5 stars4.5/5 (127)
- Total Dopamine Detox in 7 Easy Steps: Become the Master of Your Brain to Quit Your Phone Addiction, Porn Addiction, or Manage Your ADHDFrom EverandTotal Dopamine Detox in 7 Easy Steps: Become the Master of Your Brain to Quit Your Phone Addiction, Porn Addiction, or Manage Your ADHDRating: 4 out of 5 stars4/5 (8)
- Psilocybin Mushrooms: A Practical Guide to the Types and Magic Effects of Psychedelic MushroomsFrom EverandPsilocybin Mushrooms: A Practical Guide to the Types and Magic Effects of Psychedelic MushroomsRating: 4 out of 5 stars4/5 (14)
- The Kindness Method: Change Your Habits for Good Using Self-Compassion and UnderstandingFrom EverandThe Kindness Method: Change Your Habits for Good Using Self-Compassion and UnderstandingRating: 5 out of 5 stars5/5 (10)
- The Art of Self-Therapy: How to Grow, Gain Self-Awareness, and Understand Your EmotionsFrom EverandThe Art of Self-Therapy: How to Grow, Gain Self-Awareness, and Understand Your EmotionsRating: 5 out of 5 stars5/5 (1)
- Self-Love Affirmations For Deep Sleep: Raise self-worth Build confidence, Heal your wounded heart, Reprogram your subconscious mind, 8-hour sleep cycle, know your value, effortless healingsFrom EverandSelf-Love Affirmations For Deep Sleep: Raise self-worth Build confidence, Heal your wounded heart, Reprogram your subconscious mind, 8-hour sleep cycle, know your value, effortless healingsRating: 4.5 out of 5 stars4.5/5 (6)