You might also like
- Topnotch Lab Interpretation For MoonlightersDocument41 pagesTopnotch Lab Interpretation For Moonlightersmefav7778520No ratings yet
- Healing Your Chakras & Energy Body PDFDocument31 pagesHealing Your Chakras & Energy Body PDFvedashruti100% (2)
- Unit 5 Vital SignsDocument100 pagesUnit 5 Vital SignsWIKKI vinesNo ratings yet
- Microscopic Examination of Urine Part 1Document3 pagesMicroscopic Examination of Urine Part 1Sareene Joyce Pepito100% (1)
- Pleural Effusion: Dr.S.Sesha Sai (MD), Pulmonary MedicineDocument52 pagesPleural Effusion: Dr.S.Sesha Sai (MD), Pulmonary MedicinevaishnaviNo ratings yet
- Analysis of Urine and Other Body FluidsDocument9 pagesAnalysis of Urine and Other Body FluidsPajarillaga Franz Erick QuintoNo ratings yet
- Name: Abdirahman Sheikh Abdillahi Farah Faculty: Clinical Officers (CO8) Course: Pediatric Lecturer: DR Amin Assingment: Pleural EffusionDocument46 pagesName: Abdirahman Sheikh Abdillahi Farah Faculty: Clinical Officers (CO8) Course: Pediatric Lecturer: DR Amin Assingment: Pleural EffusionAbdirahman Abdillahi FarahNo ratings yet
- CSF & Body FluidDocument42 pagesCSF & Body FluidlopaNo ratings yet
- Do Not Copy Without Permission This Property Is Governed by Republic Act No. 386, Title II, Chapter 1, Article 429 of Property Law of The PhilippinesDocument11 pagesDo Not Copy Without Permission This Property Is Governed by Republic Act No. 386, Title II, Chapter 1, Article 429 of Property Law of The PhilippinesChrissa Mae Tumaliuan CatindoyNo ratings yet
- 2NF - Grand Case Presentation Written OutputDocument99 pages2NF - Grand Case Presentation Written OutputKyra Bianca R. Famacion100% (1)
- (Surg 3A) Spleen and Friends-Dr. Segismundo, Dr. Broqueza (Aisle Paler, Joseph Tolentino)Document15 pages(Surg 3A) Spleen and Friends-Dr. Segismundo, Dr. Broqueza (Aisle Paler, Joseph Tolentino)Aria Jean MostajoNo ratings yet
- Cytology of Body FluidDocument28 pagesCytology of Body FluidMalliga SundareshanNo ratings yet
- TROMBOSISDocument49 pagesTROMBOSISAgung WistaraNo ratings yet
- Cytology of Body FluidDocument68 pagesCytology of Body FluidZeeshan YousufNo ratings yet
- Comprehensive Assessment TestDocument185 pagesComprehensive Assessment TestEkatherina_de__266100% (1)
- Bio Mechanical Guidelines For Headgear ApplicationDocument21 pagesBio Mechanical Guidelines For Headgear ApplicationDeep Garg100% (2)
- Serous Fluid: FormationDocument4 pagesSerous Fluid: FormationemmanuelNo ratings yet
- Serous Fluid: Presented By: Pauline BautistaDocument13 pagesSerous Fluid: Presented By: Pauline BautistaPauline BautistaNo ratings yet
- Lecture Lesson 12. Serous, Duodenal, and Gastric FluidDocument4 pagesLecture Lesson 12. Serous, Duodenal, and Gastric FluidHANA LUNARIANo ratings yet
- Aubf Lec - Serous FluidDocument12 pagesAubf Lec - Serous FluidColene MoresNo ratings yet
- SerousDocument8 pagesSerouspekibelssNo ratings yet
- 3.pleural Effusions & PneumothoraxDocument134 pages3.pleural Effusions & PneumothoraxArleen MatincaNo ratings yet
- Efusi Pleura & EmpyemaDocument47 pagesEfusi Pleura & EmpyemaArumLaksmitaDewiNo ratings yet
- Serous Fluid AnalysisDocument4 pagesSerous Fluid AnalysisanonacadsNo ratings yet
- Pleural Effusion in ChildrenDocument54 pagesPleural Effusion in ChildrenDr Akshay P JadhavNo ratings yet
- Serous Physiology Pleural FluidDocument3 pagesSerous Physiology Pleural FluidGhina Ü MaderaNo ratings yet
- First Page PDFDocument1 pageFirst Page PDFItzel HazNo ratings yet
- 1.pleural EffusionDocument14 pages1.pleural Effusionram krishnaNo ratings yet
- Hema 2 - Prelim Topic 3 - Platelet Disorders and Laboratory TestsDocument8 pagesHema 2 - Prelim Topic 3 - Platelet Disorders and Laboratory TestsLowenstein JenzenNo ratings yet
- Body Fluids Tsilioni SlidesDocument31 pagesBody Fluids Tsilioni SlidesShaira Jane AlcantaraNo ratings yet
- Diseases - of - PleuraDocument110 pagesDiseases - of - PleuraMohamed HefnyNo ratings yet
- AUBF Serous FluidDocument7 pagesAUBF Serous FluidRichelyn Grace B. VenusNo ratings yet
- Pleural Effusion: Putu AndrikaDocument32 pagesPleural Effusion: Putu Andrikadr.Dewi ShintaherNo ratings yet
- Serous Fluid MLTDocument5 pagesSerous Fluid MLTwailjsNo ratings yet
- Serous Fluid: FunctionDocument23 pagesSerous Fluid: FunctionMarl EstradaNo ratings yet
- 1.clinicolab Diagnosis PleuPeritEFFUSIONS016Document23 pages1.clinicolab Diagnosis PleuPeritEFFUSIONS016Elena CărăvanNo ratings yet
- 2013 GuthMay8 SplenectomyDocument24 pages2013 GuthMay8 SplenectomyKNo ratings yet
- Body Fluids1Document93 pagesBody Fluids1Aliyah Tofani PawelloiNo ratings yet
- 4 Pleural, Pericardial, and Peritoneal FluidDocument25 pages4 Pleural, Pericardial, and Peritoneal FluidnanxtoyahNo ratings yet
- SEROUS-FLUID NotesDocument5 pagesSEROUS-FLUID NotesSpongebob SquarepantsNo ratings yet
- Chronic Lymphocytic Leukemia 2023Document23 pagesChronic Lymphocytic Leukemia 2023FavourNo ratings yet
- Pleural Effusion2Document42 pagesPleural Effusion2malaiya_anuragNo ratings yet
- Cat HyperlymphocytoseDocument40 pagesCat HyperlymphocytoseDésiré Pengdéwendé OUEDRAOGONo ratings yet
- Pakar Note ANALISIS CAIRAN PLEURA & - PERICARD, BGA MADE EASYDocument8 pagesPakar Note ANALISIS CAIRAN PLEURA & - PERICARD, BGA MADE EASYLa Ode Muhammadin MatahanaNo ratings yet
- Aubf Lec Week 15Document7 pagesAubf Lec Week 15Joanne RemolloNo ratings yet
- Meningitis MicrobiologyDocument74 pagesMeningitis MicrobiologyJyoti YadavNo ratings yet
- The Specialist: Consultation WithDocument8 pagesThe Specialist: Consultation WithsarabisimonaNo ratings yet
- Platelet DisordersDocument9 pagesPlatelet DisordersSophia Gail ChingNo ratings yet
- 2007 Nov 07 CompleteDocument62 pages2007 Nov 07 CompleteKay BristolNo ratings yet
- Pleural Effusion: ObjectivesDocument14 pagesPleural Effusion: ObjectivesRashmaNo ratings yet
- Fluid:serum Protein Fluid: Serum LDDocument3 pagesFluid:serum Protein Fluid: Serum LDFiverNo ratings yet
- Lo Week 5-1Document13 pagesLo Week 5-1Martien Silviandy SetiawanNo ratings yet
- Penyakit Pleura (DrIlyas)Document60 pagesPenyakit Pleura (DrIlyas)Rey AlwiwikhNo ratings yet
- Hem OncDocument26 pagesHem OncJim XieNo ratings yet
- UW Peds CorrectionsDocument40 pagesUW Peds Correctionszara_emmeNo ratings yet
- Chapter 13 Serous FluidDocument6 pagesChapter 13 Serous FluidDIVINE GRACE FLORITA PEPITONo ratings yet
- Bleeding Disorders: - Edna U. Robles, RN Man St. Luke's College of NursingDocument52 pagesBleeding Disorders: - Edna U. Robles, RN Man St. Luke's College of Nursingfleur harrisonNo ratings yet
- Approach To Pleural Diseases2Document153 pagesApproach To Pleural Diseases2Shanza AmaanNo ratings yet
- Hema - PointersDocument5 pagesHema - PointersLUALHATI VILLASNo ratings yet
- Synovial Fluid RetypedDocument37 pagesSynovial Fluid Retypedbaechiu luvieNo ratings yet
- Laboratory Interpretation Made Easy: Diana Tamondong-Lachica, MD, FPCPDocument41 pagesLaboratory Interpretation Made Easy: Diana Tamondong-Lachica, MD, FPCPmarieNo ratings yet
- ProtozoologyDocument28 pagesProtozoologyStella Agatha WidjajaNo ratings yet
- Pleural Fluid Testing AlgorithmDocument5 pagesPleural Fluid Testing Algorithm3CBSMLSBRILLO Ma. Therese CabantingNo ratings yet
- Pleural EffusionDocument2 pagesPleural EffusionCharles WangsadjajaNo ratings yet
- Maxillary SinusitisDocument28 pagesMaxillary SinusitisSumaNo ratings yet
- Understanding The Different Routes of Drug AdministrationDocument3 pagesUnderstanding The Different Routes of Drug AdministrationMark Russel Sean LealNo ratings yet
- Yoga de Stress ProgrammDocument6 pagesYoga de Stress ProgrammSnikitaNo ratings yet
- Jurnal 1Document8 pagesJurnal 1Renita Mandalinta SitepuNo ratings yet
- Health6 q1 Mod2 Selfmanagement v1Document23 pagesHealth6 q1 Mod2 Selfmanagement v1BrianJessenMaweDignosNo ratings yet
- Assessment of Aortic RegurgitationDocument8 pagesAssessment of Aortic RegurgitationKhurram NadeemNo ratings yet
- HPV DissertationDocument4 pagesHPV DissertationWriteMyPaperForMeIn3HoursSpringfield100% (1)
- 022 Workplace Stress Evaluation ToolsDocument36 pages022 Workplace Stress Evaluation ToolsISCRRNo ratings yet
- Group Work Case Study Problems-1Document7 pagesGroup Work Case Study Problems-1Rahul Kumar DiwakarNo ratings yet
- SOAL UTS KMB 3 3C (Jawaban)Document20 pagesSOAL UTS KMB 3 3C (Jawaban)Millah SamillahNo ratings yet
- Affections of OesophagusDocument32 pagesAffections of OesophagusNaveen BasudeNo ratings yet
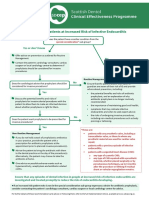
- SDCEP Antibiotic Prophylaxis Summary FlowchartDocument1 pageSDCEP Antibiotic Prophylaxis Summary FlowchartMahmoud EladawyNo ratings yet
- Iron Deficiency AnemiaDocument4 pagesIron Deficiency AnemiaWiljohn de la CruzNo ratings yet
- Health at A Glance - Asia PacificDocument146 pagesHealth at A Glance - Asia PacificPuneet MehtaNo ratings yet
- Tels3340chap# 13 PDFDocument14 pagesTels3340chap# 13 PDFArbindchaudhary0% (1)
- Changes in College Student Endorsement of ADHD Symptoms Across DSM EditionDocument12 pagesChanges in College Student Endorsement of ADHD Symptoms Across DSM EditionRaul Morales VillegasNo ratings yet
- Allianz Prime Cover BrochureDocument17 pagesAllianz Prime Cover Brochurevf5jmszwg2No ratings yet
- Kara No Kyoukai 4Document43 pagesKara No Kyoukai 4Joshua MarceloNo ratings yet
- NeldamDocument10 pagesNeldamdini hanifaNo ratings yet
- Med - Surg Sample QuestionDocument55 pagesMed - Surg Sample QuestionCHARLYN DELOS REYESNo ratings yet
- Soldul 2021 RompharmDocument20 pagesSoldul 2021 RompharmGhica CostinNo ratings yet
- A Study On Operational Audit of Hospital - Kaushalya HospitalDocument105 pagesA Study On Operational Audit of Hospital - Kaushalya Hospitalashish patelNo ratings yet
- Medical Cannabis: Information Brochure For PatientsDocument17 pagesMedical Cannabis: Information Brochure For PatientsKwesi Cudi ArhinNo ratings yet
- Risks and Safety Measures Intig Welding ProcessDocument5 pagesRisks and Safety Measures Intig Welding ProcessSeminarski radoviNo ratings yet
- Covid19 - Nurse Burnout FinalDocument5 pagesCovid19 - Nurse Burnout Finalapi-587935422No ratings yet