You might also like
- Different Sleep Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDifferent Sleep Disorders, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Consent For Below Knee Amputation: Task: No Need For HX and Exam. Obtain Consent From PT and Answer Examiner's QuestionsDocument12 pagesConsent For Below Knee Amputation: Task: No Need For HX and Exam. Obtain Consent From PT and Answer Examiner's QuestionsffaaNo ratings yet
- TGD D 2018Document7 pagesTGD D 2018Nadhirah ZulkifliNo ratings yet
- Instruments WorksheetDocument28 pagesInstruments WorksheetRV's Banana RotiNo ratings yet
- Morning Report: Supervisor Dr. Sabar P. Siregar, SP - KJDocument41 pagesMorning Report: Supervisor Dr. Sabar P. Siregar, SP - KJAyunita PermataNo ratings yet
- Morpot 21 SeptDocument41 pagesMorpot 21 SeptTasia DeastutiNo ratings yet
- Morning Report 17 SeptemberDocument42 pagesMorning Report 17 SeptemberkadibhaNo ratings yet
- Gangguan Katatonik OrganikDocument41 pagesGangguan Katatonik OrganikFerji Rhenald ArdityaNo ratings yet
- Psychiatric Case PerformaDocument8 pagesPsychiatric Case Performaparnika100% (1)
- Sunday, 24 November 2013 Supervisor: DR Sabar P Siregar SP - KJDocument37 pagesSunday, 24 November 2013 Supervisor: DR Sabar P Siregar SP - KJMutiara SazkiaNo ratings yet
- ClinicalDocument61 pagesClinicalokpala ikennaNo ratings yet
- Multiple Choice Questions Multiple Choice QuestionsDocument19 pagesMultiple Choice Questions Multiple Choice QuestionsKay VinesNo ratings yet
- Morning Report 6 Aug 2012Document40 pagesMorning Report 6 Aug 2012Wilutami Rahardiyaning TyasNo ratings yet
- Psychiatry: Questions&AnswersDocument92 pagesPsychiatry: Questions&AnswersCielNo ratings yet
- USMLEasy Psych Case01Document10 pagesUSMLEasy Psych Case01Tanzeel Ur RehmanNo ratings yet
- Psychiatry (1) 1Document26 pagesPsychiatry (1) 1esmatNo ratings yet
- Clinical Tutorial 2008.11.05Document31 pagesClinical Tutorial 2008.11.05Ywagar Ywagar100% (1)
- 21st April 2018Document4 pages21st April 2018lkdsjflsNo ratings yet
- Use of Psychotropics in PregnancyDocument24 pagesUse of Psychotropics in Pregnancymanahil waqasNo ratings yet
- Geriatric Assessment TomtomDocument4 pagesGeriatric Assessment TomtomMark Angelo Soliman AcupidoNo ratings yet
- MCQS:: A) Imipramine 1 C) Nortriptyline 2 D) Duxepine 3 E) AmitryptalineDocument7 pagesMCQS:: A) Imipramine 1 C) Nortriptyline 2 D) Duxepine 3 E) AmitryptalineEyob MizanNo ratings yet
- Coughlin Psyc Exam Results OcrDocument10 pagesCoughlin Psyc Exam Results OcrDoTheMacaRenoNo ratings yet
- Abnormal Psychology ReviewerDocument23 pagesAbnormal Psychology ReviewerPinca, Junea PaulaNo ratings yet
- Aacase 2Document13 pagesAacase 2Michele RogersNo ratings yet
- Review QuestionsDocument5 pagesReview Questionsjmkap13No ratings yet
- Psychology Exam Chapter 1Document29 pagesPsychology Exam Chapter 1Besim HasangjekajNo ratings yet
- Schizophrenia BrochureDocument3 pagesSchizophrenia BrochureFarhana SobriNo ratings yet
- Paediatrics:: Case 1nsionDocument16 pagesPaediatrics:: Case 1nsionYwagar YwagarNo ratings yet
- Psych RecallDocument10 pagesPsych RecallSherif ElbadrawyNo ratings yet
- Psych Questions 1Document34 pagesPsych Questions 1MADHUMITHA VEMULA100% (1)
- MA in Psychology - Clinical Psychology (Thesis) .FEUDocument1 pageMA in Psychology - Clinical Psychology (Thesis) .FEUPaul Anthony PascualNo ratings yet
- Exam Ready To PrintDocument3 pagesExam Ready To PrintYaj Cruzada0% (1)
- Psychiatry: When Your Mood Is High?Document38 pagesPsychiatry: When Your Mood Is High?Mavra zNo ratings yet
- 68 Important Scenarios For ST 5 PracticeDocument20 pages68 Important Scenarios For ST 5 PracticeSalem ELsayed Abdel AzizNo ratings yet
- Recall 67, 25.2.12Document23 pagesRecall 67, 25.2.12fdsadfNo ratings yet
- Station 1-Relapse of Schizophrenia (PASS)Document6 pagesStation 1-Relapse of Schizophrenia (PASS)PragashRajendirenNo ratings yet
- Case Pres-Banag Laum SuperfinaleDocument46 pagesCase Pres-Banag Laum SuperfinaleAyen FornollesNo ratings yet
- 03 PAEDS NeurologyDocument13 pages03 PAEDS Neurologyfire_n_iceNo ratings yet
- Morning Report: Supervisor Dr. Sabar P. Siregar, SP - KJDocument47 pagesMorning Report: Supervisor Dr. Sabar P. Siregar, SP - KJVike Poraddwita YuliantiNo ratings yet
- Obstetrics and Gynaecology Cases Amc Clinical RecallsDocument2 pagesObstetrics and Gynaecology Cases Amc Clinical RecallsRamez Abu KhalilNo ratings yet
- H&P and Daily Progress NotesDocument1 pageH&P and Daily Progress NotesМилица СвиларNo ratings yet
- Psychiatry: Taking A Psychiatric HistoryDocument48 pagesPsychiatry: Taking A Psychiatric Historyfdjslajf100% (1)
- Psychiatry Notes - Depressive DisorderDocument2 pagesPsychiatry Notes - Depressive DisorderLiSenNo ratings yet
- 15 - SchizophreniaDocument4 pages15 - SchizophreniaGede Tamblang Baswara PutraNo ratings yet
- Clinical Case Reviews 2016Document34 pagesClinical Case Reviews 2016johnNo ratings yet
- Recall Brisbane February 2008Document7 pagesRecall Brisbane February 2008Ywagar YwagarNo ratings yet
- PSYC 2740 Term Test PDFDocument7 pagesPSYC 2740 Term Test PDFsukhleen Saini100% (1)
- 05.psychiatry Fixed by E.G E.KDocument54 pages05.psychiatry Fixed by E.G E.KMoataz Trabeh100% (1)
- Dams Psychiatry Pyq Fmge SolvedDocument81 pagesDams Psychiatry Pyq Fmge SolvedmeetsinhhermaNo ratings yet
- Lecture Notes On PsychiatryDocument38 pagesLecture Notes On Psychiatrygemazy123No ratings yet
- A Case Study of A Mental DisorderDocument7 pagesA Case Study of A Mental DisorderMaurine TuitoekNo ratings yet
- Psychiatry Diagnosis PDFDocument4 pagesPsychiatry Diagnosis PDFEpstein HouseNo ratings yet
- 7 - Common Psychiatric Problems - Mubarak-SubaieDocument62 pages7 - Common Psychiatric Problems - Mubarak-SubaieLavitSutcharitkulNo ratings yet
- 4 - Anti-Psychotics-Redi (Nema)Document40 pages4 - Anti-Psychotics-Redi (Nema)Endre Shitaye KulkiNo ratings yet
- Clinical Features of Common Psychiatric DisordersDocument21 pagesClinical Features of Common Psychiatric DisordersShivan A.C.No ratings yet
- Activity10 7 17Document11 pagesActivity10 7 17Charlotte GallegoNo ratings yet
- 16 Batch PsychiatryDocument12 pages16 Batch Psychiatryangad.soniv100% (1)
- Definition:: I. Diagnostic Tests 1. Phases-Pretests Intratests Post Tests 2. Blood Tests - CBCDocument13 pagesDefinition:: I. Diagnostic Tests 1. Phases-Pretests Intratests Post Tests 2. Blood Tests - CBCKelly Sosa LuyunNo ratings yet
- Adolf Meyer & George Barton3 in OTDocument14 pagesAdolf Meyer & George Barton3 in OTHermito GideonNo ratings yet
- Somatoform DisorderDocument3 pagesSomatoform DisorderJunar M. BalasbasNo ratings yet
- OBS & Gynec-Antepartum HaemorrhageDocument18 pagesOBS & Gynec-Antepartum HaemorrhageRahul Kumar DiwakarNo ratings yet
- ENT-Laryngeal ParalysisDocument26 pagesENT-Laryngeal ParalysisRahul Kumar DiwakarNo ratings yet
- Human Devlopment 1: Level 1Document27 pagesHuman Devlopment 1: Level 1Rahul Kumar DiwakarNo ratings yet
- Antidepressants PrintedDocument3 pagesAntidepressants PrintedRahul Kumar DiwakarNo ratings yet
- Psychological Aspects of HIVDocument17 pagesPsychological Aspects of HIVRahul Kumar DiwakarNo ratings yet
- Ward 8M: Evaluation of Thought Process and SpeechDocument17 pagesWard 8M: Evaluation of Thought Process and SpeechRahul Kumar DiwakarNo ratings yet
- Ophthalmology-Development of EyeDocument20 pagesOphthalmology-Development of EyeRahul Kumar DiwakarNo ratings yet
- Postpartum Blues: by DR Wangari KuriaDocument9 pagesPostpartum Blues: by DR Wangari KuriaRahul Kumar DiwakarNo ratings yet
- Intellectual Disability/ Mental Retardation: Level IV Tutorial 2015/2016 DR J. KamauDocument21 pagesIntellectual Disability/ Mental Retardation: Level IV Tutorial 2015/2016 DR J. KamauRahul Kumar DiwakarNo ratings yet
- Pain and Behavior: Objectives - Understand Purpose of Pain - Pain Pathway - Differences On Different IndividualsDocument26 pagesPain and Behavior: Objectives - Understand Purpose of Pain - Pain Pathway - Differences On Different IndividualsRahul Kumar DiwakarNo ratings yet
- Training Guide: Recording and Handling of Schedule 8 Drugs in Hospital WardsDocument41 pagesTraining Guide: Recording and Handling of Schedule 8 Drugs in Hospital WardsRahul Kumar DiwakarNo ratings yet
- Eating Disorders: by Pius KigamwaDocument20 pagesEating Disorders: by Pius KigamwaRahul Kumar DiwakarNo ratings yet
- Emergency Psychiatry: SuicideDocument3 pagesEmergency Psychiatry: SuicideRahul Kumar Diwakar100% (1)
- HELPPP FinalDocument55 pagesHELPPP FinalRahul Kumar DiwakarNo ratings yet
- Male Sexual Disordees: Tutorial Level 4-2015Document57 pagesMale Sexual Disordees: Tutorial Level 4-2015Rahul Kumar DiwakarNo ratings yet
- Delirium: by Pius KigamwaDocument15 pagesDelirium: by Pius KigamwaRahul Kumar DiwakarNo ratings yet
- Process of Rehabilitation in PsychiatryDocument29 pagesProcess of Rehabilitation in PsychiatryRahul Kumar DiwakarNo ratings yet
- SUBSTANCE ABUSEpresentation Level 4Document43 pagesSUBSTANCE ABUSEpresentation Level 4Rahul Kumar Diwakar100% (1)
- Drug Addiction: Alcohol Other Substances Counselling Class Lesson 6Document34 pagesDrug Addiction: Alcohol Other Substances Counselling Class Lesson 6Rahul Kumar DiwakarNo ratings yet
- Mental Disorders Secondary To General Medical ConditionsDocument25 pagesMental Disorders Secondary To General Medical ConditionsRahul Kumar DiwakarNo ratings yet
- Schizophrenia Lecture 2010 PART 1 and 2Document69 pagesSchizophrenia Lecture 2010 PART 1 and 2Rahul Kumar DiwakarNo ratings yet
- Schizophrenia and Other Psychotic Disorders: DR Rachel Kang'Ethe Department of PsychiatryDocument76 pagesSchizophrenia and Other Psychotic Disorders: DR Rachel Kang'Ethe Department of PsychiatryRahul Kumar Diwakar100% (1)
- What You Should Know About COVID-19 To Protect Yourself and OthersDocument2 pagesWhat You Should Know About COVID-19 To Protect Yourself and OthersRahul Kumar DiwakarNo ratings yet
- Psychological Aspects of HIV-level IIDocument18 pagesPsychological Aspects of HIV-level IIRahul Kumar DiwakarNo ratings yet
- Review Artilces Annals and Essences of DentistryDocument14 pagesReview Artilces Annals and Essences of DentistryRahul Kumar DiwakarNo ratings yet
- Lesson Plan DepressionDocument19 pagesLesson Plan DepressionRahul Kumar Diwakar100% (1)
- Punjab Medicolegal Manual Jan30 PDFDocument18 pagesPunjab Medicolegal Manual Jan30 PDFFrank NobodNo ratings yet
- ANALYSISDocument1 pageANALYSISIstikharohNo ratings yet
- HIV and AIDsDocument4 pagesHIV and AIDsPersistance MharadzeNo ratings yet
- Application Form - FMU (New Form BUPA)Document16 pagesApplication Form - FMU (New Form BUPA)gabinicolescu9999No ratings yet
- Analyzing Exposition Text (Tarishah Ayu - 34)Document3 pagesAnalyzing Exposition Text (Tarishah Ayu - 34)Tarisa AyuNo ratings yet
- Muscles Developing Properties of Gamma Oryzanol - ResearchDocument1 pageMuscles Developing Properties of Gamma Oryzanol - ResearchRAJESH ANNAMALAI ALNo ratings yet
- Angela Shrestha - Written Assessment AnswersDocument3 pagesAngela Shrestha - Written Assessment AnswersAngela ShresthaNo ratings yet
- Care of Elderly - NCP1Document2 pagesCare of Elderly - NCP1ROGEN KATE AZARCONNo ratings yet
- Đề số 1Document5 pagesĐề số 1Thúy NgânNo ratings yet
- 2ed Y2 72-73 3-9 Hypotheses and SignificanceDocument1 page2ed Y2 72-73 3-9 Hypotheses and SignificancejNo ratings yet
- Endo-Perio Dilemma A Brief ReviewDocument10 pagesEndo-Perio Dilemma A Brief ReviewLuisNo ratings yet
- How To Do Dhanurasana (Bow Pose)Document2 pagesHow To Do Dhanurasana (Bow Pose)MIBNo ratings yet
- Hard Hat, Safety Glasses, Gloves: Yemen DrillingDocument2 pagesHard Hat, Safety Glasses, Gloves: Yemen DrillingkhurramNo ratings yet
- Nursing and Interdisciplinary of StrokeDocument36 pagesNursing and Interdisciplinary of StrokeMohamed Abd El MonemNo ratings yet
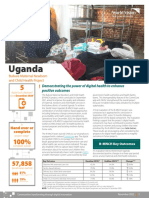
- 2021 Digital Health Factsheet - B-MNCH - UgandaDocument2 pages2021 Digital Health Factsheet - B-MNCH - UgandaMd UmerNo ratings yet
- The Generation of DRR With Six ParametersDocument4 pagesThe Generation of DRR With Six ParametersBojar DogNo ratings yet
- Gerontologic Nursing 10Document10 pagesGerontologic Nursing 10Sherrylyne Anne De Francia - OrdanzaNo ratings yet
- Sample Brgy DTPDocument43 pagesSample Brgy DTPpagangpang galimuyod100% (19)
- 2nd Summative TestDocument4 pages2nd Summative TestMarie Antonette Aco BarbaNo ratings yet
- Shell Helix HX5 15W 40 TDS PDFDocument2 pagesShell Helix HX5 15W 40 TDS PDFhoussem houssemNo ratings yet
- Soccer Training: An Annual ProgrammeDocument314 pagesSoccer Training: An Annual Programmefranco03567% (3)
- Makassar 1: Total Target OptimisDocument2 pagesMakassar 1: Total Target OptimisAchaElmanNo ratings yet
- Medical For Athletes 1Document2 pagesMedical For Athletes 1carmina duldulaoNo ratings yet
- Cholinergic Urticaria - Google SearchDocument1 pageCholinergic Urticaria - Google SearchStephanie NhyiraNo ratings yet
- Welcome Plan Welcome CorpsDocument20 pagesWelcome Plan Welcome CorpsAxmed Cadnaan50% (2)
- F 01 01 02 A FORM PENDAFTARAN Rev 28-20 TRAINING IKBAL IKBAL-M-YOSDocument2 pagesF 01 01 02 A FORM PENDAFTARAN Rev 28-20 TRAINING IKBAL IKBAL-M-YOSjerrysibaoadiNo ratings yet
- Practice Lw-03: Questions 1-5 Choose The Correct Letter, A, B or CDocument6 pagesPractice Lw-03: Questions 1-5 Choose The Correct Letter, A, B or CViet HoangNo ratings yet
- Biotechnology - Humber CollegeDocument1 pageBiotechnology - Humber CollegeYouTube AsuranNo ratings yet
- LPN RN Exam AppDocument21 pagesLPN RN Exam Appstring44No ratings yet
- Erich Fromm - A Therapeutic Vision Well Ahead of Its TimeDocument8 pagesErich Fromm - A Therapeutic Vision Well Ahead of Its TimeSteluța DrâmbuNo ratings yet