You might also like
- ICU IV Infusion GuidelinesDocument2 pagesICU IV Infusion Guidelinessgod34No ratings yet
- Clinical Log Book BSC Nursing 170622Document87 pagesClinical Log Book BSC Nursing 170622Shital Pawar100% (1)
- Head and Neck: Openings in The Base of The Skull and The Structures That Pass Through ThemDocument11 pagesHead and Neck: Openings in The Base of The Skull and The Structures That Pass Through ThemcathdelosoNo ratings yet
- Barış Çakır - Aesthetic Septorhinoplasty-Springer (2021) PDFDocument796 pagesBarış Çakır - Aesthetic Septorhinoplasty-Springer (2021) PDFaztec8765No ratings yet
- Biology NMAT Notes AnatomyCirculatory and RespiratoryDocument13 pagesBiology NMAT Notes AnatomyCirculatory and RespiratoryMa. Teresa M. AbainzaNo ratings yet
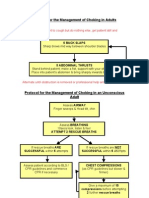
- Protocol For The Management of Choking in AdultsDocument3 pagesProtocol For The Management of Choking in AdultsSarinah RynaNo ratings yet
- Yagnik 2192017 BJMMR32834Document8 pagesYagnik 2192017 BJMMR32834aminNo ratings yet
- Decision Algỏithm and Surgical Strategies For Managing Trachecutaneous FistulaDocument9 pagesDecision Algỏithm and Surgical Strategies For Managing Trachecutaneous Fistulahai1No ratings yet
- Merits of Harmonic ScalpelDocument5 pagesMerits of Harmonic ScalpelVikrant VazeNo ratings yet
- Alesina et al., 2021Document9 pagesAlesina et al., 2021NyomantrianaNo ratings yet
- Emergency Inguinal Hernia Repair Under Local Anesthesia: A 5-Year Experience in A Teaching HospitalDocument5 pagesEmergency Inguinal Hernia Repair Under Local Anesthesia: A 5-Year Experience in A Teaching HospitalleonardoNo ratings yet
- armijo2020Document7 pagesarmijo2020Yeudiel SuroNo ratings yet
- Anterior Versus Posterior Surgical Approach For Lumbosacral TuberculosisDocument9 pagesAnterior Versus Posterior Surgical Approach For Lumbosacral TuberculosisI Made Dhita PriantharaNo ratings yet
- JurnalDocument8 pagesJurnalahtarunnisaNo ratings yet
- Assessment of Enhanced Recovery After Surgery (Erasâ®) Protocol in Colorectal Cancer SurgeryDocument8 pagesAssessment of Enhanced Recovery After Surgery (Erasâ®) Protocol in Colorectal Cancer SurgeryIJAR JOURNALNo ratings yet
- Incisional Hernia Mesh RepairDocument5 pagesIncisional Hernia Mesh Repaireka henny suryaniNo ratings yet
- Comparison of Closed Femur Fracture: Skeletal Traction and Intramedullary Nailing Cost-EffectivenessDocument6 pagesComparison of Closed Femur Fracture: Skeletal Traction and Intramedullary Nailing Cost-EffectivenessS3V4_9154No ratings yet
- JCM 10 01853Document16 pagesJCM 10 01853Katrina Mae FajardoNo ratings yet
- JurnalDocument8 pagesJurnalwiliaNo ratings yet
- 10 36516-Jocass 1240290-2908682Document5 pages10 36516-Jocass 1240290-2908682yyyyx842No ratings yet
- Medip, ISJ-5301 ODocument4 pagesMedip, ISJ-5301 OJesus EspinozaNo ratings yet
- Jurnal EBM WBWMDocument10 pagesJurnal EBM WBWMUliza Nur AiniNo ratings yet
- Type A1 Intertroch PFN VS DHS RetrospectiveDocument11 pagesType A1 Intertroch PFN VS DHS RetrospectiveMuhammad Tabish SaleemNo ratings yet
- Vrijland Et Al-2002-British Journal of SurgeryDocument5 pagesVrijland Et Al-2002-British Journal of SurgeryTivHa Cii Mpuzz MandjaNo ratings yet
- GJHS 6 221Document5 pagesGJHS 6 221Teuku FaisalNo ratings yet
- Jurnal 5Document4 pagesJurnal 5Roro Khairiyah AmaliaNo ratings yet
- Hemipelvectomia INCADocument7 pagesHemipelvectomia INCAdrjccanciolopesNo ratings yet
- Annals of Medicine and Surgery: SciencedirectDocument7 pagesAnnals of Medicine and Surgery: SciencedirectBagoes AsNo ratings yet
- Single-Incision Thoracoscopic Surgery For Primary Spontaneous PneumothoraxDocument4 pagesSingle-Incision Thoracoscopic Surgery For Primary Spontaneous PneumothoraxRiani NazilaNo ratings yet
- Comparative Analysis of Clinical Outcomes of Open Appendectomy and Laparoscopic AppendectomyDocument6 pagesComparative Analysis of Clinical Outcomes of Open Appendectomy and Laparoscopic AppendectomyIJRASETPublicationsNo ratings yet
- International Journal of SurgeryDocument6 pagesInternational Journal of SurgeryRadhwen Zarg el ayounNo ratings yet
- With The Advance in The Techniques of Hemostasis Is It Necessary To Use Drain Routinely in Thyroid Surgery A Comparative StudyDocument8 pagesWith The Advance in The Techniques of Hemostasis Is It Necessary To Use Drain Routinely in Thyroid Surgery A Comparative StudyAthenaeum Scientific PublishersNo ratings yet
- Rectal Stenosis After Procedures For Prolapse and Hemorrhoids (PPH) - A Report From ChinaDocument5 pagesRectal Stenosis After Procedures For Prolapse and Hemorrhoids (PPH) - A Report From ChinaAmriansyah PranowoNo ratings yet
- Jamil Ahmed - Effectiveness of ProcedureDocument4 pagesJamil Ahmed - Effectiveness of ProcedureMansoor TariqNo ratings yet
- Laparoscopic Appendectomy PostoperativeDocument6 pagesLaparoscopic Appendectomy PostoperativeDamal An NasherNo ratings yet
- ACFrOgAB8 Tkw2cTNZ5H661ndcneV9fi1RTn1ykvnJvumEFlHYEvSpEHtoXIvYK5jjNGQbrB35rwgjvkxfQME3bphkaekY6xwI BQlK08W3zxE2v4uvQ7YrquWEUIv3SWl0RB VNAPF1WDhLtIIeDocument6 pagesACFrOgAB8 Tkw2cTNZ5H661ndcneV9fi1RTn1ykvnJvumEFlHYEvSpEHtoXIvYK5jjNGQbrB35rwgjvkxfQME3bphkaekY6xwI BQlK08W3zxE2v4uvQ7YrquWEUIv3SWl0RB VNAPF1WDhLtIIevinicius.alvarez3No ratings yet
- Ejm 46578 Original - Article TumerDocument7 pagesEjm 46578 Original - Article TumerMohammed FaragNo ratings yet
- Outcomes of 207 Totally Extraperitoneal Hernia Repairs Using Self Fixation MeshDocument8 pagesOutcomes of 207 Totally Extraperitoneal Hernia Repairs Using Self Fixation Mesha kNo ratings yet
- Homemade Mitral RingDocument4 pagesHomemade Mitral Ringadel husseinNo ratings yet
- 1-s2.0-S0901502716300728-mainDocument4 pages1-s2.0-S0901502716300728-mainCaio GonçalvesNo ratings yet
- FUNCTIONAL OUTCOME OF TOTAL HIP ARTHROPLASTY WITH DUAL MOBILITY CUPS IN HIP ARTHRITIS-A PROSPECTIVE COHORT STUDYDocument7 pagesFUNCTIONAL OUTCOME OF TOTAL HIP ARTHROPLASTY WITH DUAL MOBILITY CUPS IN HIP ARTHRITIS-A PROSPECTIVE COHORT STUDYIJAR JOURNALNo ratings yet
- Stapled Rectal Mucosectomy vs. Close HemorrhoidectomyDocument9 pagesStapled Rectal Mucosectomy vs. Close HemorrhoidectomyNadllely Garcia ZapataNo ratings yet
- f194 DikonversiDocument5 pagesf194 DikonversiFarizka Dwinda HNo ratings yet
- Precedex Delirium Spine - AA2023Document9 pagesPrecedex Delirium Spine - AA2023Ahida VelazquezNo ratings yet
- Ismaeil 2018Document15 pagesIsmaeil 2018Javier ZaquinaulaNo ratings yet
- Fsurg 10 1151327Document7 pagesFsurg 10 1151327theomnagarowner2811No ratings yet
- 1 s2.0 S1015958422008909 MainDocument4 pages1 s2.0 S1015958422008909 MainYohan WijayabahuNo ratings yet
- Cutaneous Needle Aspirations in Liver DiseaseDocument6 pagesCutaneous Needle Aspirations in Liver DiseaseRhian BrimbleNo ratings yet
- DTSCH Arztebl Int-115 0031Document12 pagesDTSCH Arztebl Int-115 0031Monika Diaz KristyanindaNo ratings yet
- Clinical Efficacy of Enhanced Recovery After Surgery in Percutaneous Nephrolithotripsy: A Randomized Controlled TrialDocument8 pagesClinical Efficacy of Enhanced Recovery After Surgery in Percutaneous Nephrolithotripsy: A Randomized Controlled TrialfaundraNo ratings yet
- Single Incision Laparoscopic Appendicectomy Versus Conventional Laparoscopic Appendicectomy-A Prospective StudyDocument6 pagesSingle Incision Laparoscopic Appendicectomy Versus Conventional Laparoscopic Appendicectomy-A Prospective StudySabreen SaniaNo ratings yet
- Laparoscopic Appendectomy For Complicated Appendicitis - An Evaluation of Postoperative Factors.Document5 pagesLaparoscopic Appendectomy For Complicated Appendicitis - An Evaluation of Postoperative Factors.Juan Carlos SantamariaNo ratings yet
- Umesh Singh. TLTK-47Document5 pagesUmesh Singh. TLTK-47HẢI HOÀNG THANHNo ratings yet
- A Wet Dressing For Male Genital Surgery: A Phase II Clinical TrialDocument8 pagesA Wet Dressing For Male Genital Surgery: A Phase II Clinical TrialhendraNo ratings yet
- Effect of Pterygomaxillary Disjunction on Orthodontic Treatment OutcomesDocument11 pagesEffect of Pterygomaxillary Disjunction on Orthodontic Treatment OutcomesArthur CésarNo ratings yet
- Estenosis AnalDocument5 pagesEstenosis AnalluissparkNo ratings yet
- Iranjradiol 14 03 21742Document5 pagesIranjradiol 14 03 21742AisahNo ratings yet
- AmJGastroenterol20061012016 24Document9 pagesAmJGastroenterol20061012016 24AbhinavNo ratings yet
- Art 3Document6 pagesArt 3Claudia IrimieNo ratings yet
- Long-Term Results of a Randomized Trial on Prophylactic Intraperitoneal Mesh for Midline Incisional Hernia PreventionDocument7 pagesLong-Term Results of a Randomized Trial on Prophylactic Intraperitoneal Mesh for Midline Incisional Hernia PreventiondrpklalNo ratings yet
- JurnalDocument5 pagesJurnalFuchsia ZeinNo ratings yet
- Comparative Efficacy of Neuraxial and General Anesthesia For Hip Fracture SurgeryDocument12 pagesComparative Efficacy of Neuraxial and General Anesthesia For Hip Fracture Surgeryangelama1783riosNo ratings yet
- Initial Experience With Application of Single Layer Modified Kugel Mesh For Inguinal Hernia Repair: Case Series of 72 Consecutive PatientsDocument6 pagesInitial Experience With Application of Single Layer Modified Kugel Mesh For Inguinal Hernia Repair: Case Series of 72 Consecutive Patientsnur hasnahNo ratings yet
- Transoral Thyroidectomy and Parathyroidectomy: A North American Series of Robotic and Endoscopic ApproachesDocument6 pagesTransoral Thyroidectomy and Parathyroidectomy: A North American Series of Robotic and Endoscopic Approachespancholin_9No ratings yet
- Clinical Approach For The Pneumomediastinum After Blunt Chest TraumaDocument7 pagesClinical Approach For The Pneumomediastinum After Blunt Chest TraumaIdham Adyasa Manggala PutraNo ratings yet
- Case Studies of Postoperative Complications after Digestive SurgeryFrom EverandCase Studies of Postoperative Complications after Digestive SurgeryNo ratings yet
- 16 CR 6907 IngDocument2 pages16 CR 6907 IngdianisaindiraNo ratings yet
- Iodine 125 Seed Implantation Combined Chemotherapy.47Document4 pagesIodine 125 Seed Implantation Combined Chemotherapy.47dianisaindiraNo ratings yet
- Anatomi Systema Respiratorium Dr. DodikDocument58 pagesAnatomi Systema Respiratorium Dr. DodikIrfan Maulana AjiNo ratings yet
- 10.scenario 2Document2 pages10.scenario 2dianisaindiraNo ratings yet
- Document PDFDocument11 pagesDocument PDFYANDA PELIA ANo ratings yet
- Tropicalmed 03 00037Document9 pagesTropicalmed 03 00037dianisaindiraNo ratings yet
- R Cube Healthcare Industries: Leading Medical Equipment ProviderDocument27 pagesR Cube Healthcare Industries: Leading Medical Equipment Providerrcube healthcareNo ratings yet
- Pharmacokinetic and Pharmacodynamic Concepts Underpinning Total Intravenous AnesthesiaDocument4 pagesPharmacokinetic and Pharmacodynamic Concepts Underpinning Total Intravenous AnesthesiaZaida RamosNo ratings yet
- Zone 3 REBOA EvaluationDocument7 pagesZone 3 REBOA EvaluationJean CotteNo ratings yet
- Tosp Booklet With MSP (3 Jan 2017) WordDocument112 pagesTosp Booklet With MSP (3 Jan 2017) WordArif Tri Prasetyo HarunNo ratings yet
- Deena Horn DPM AACFAS, John Doolan DPM FACFAS, Adam Cirlincione FACFAS DPM Joseph Larsen DPM FACFASDocument1 pageDeena Horn DPM AACFAS, John Doolan DPM FACFAS, Adam Cirlincione FACFAS DPM Joseph Larsen DPM FACFASbaoNo ratings yet
- Final SurgeryDocument35 pagesFinal SurgeryChinniah RamkumarNo ratings yet
- DR - Kavita Priya Iicm 1Document68 pagesDR - Kavita Priya Iicm 1Kavita PriyaNo ratings yet
- Tumors of The Meninges NotesDocument20 pagesTumors of The Meninges NotesUltrasound ResultNo ratings yet
- Procedural Skills (Awasir)Document34 pagesProcedural Skills (Awasir)Yousef TaqatqehNo ratings yet
- Int Endodontic J - 2016 - Ahmed - A New System For Classifying Root and Root Canal MorphologyDocument10 pagesInt Endodontic J - 2016 - Ahmed - A New System For Classifying Root and Root Canal MorphologyRodrigo Cassana RojasNo ratings yet
- Priyanka New PPT Final 2-1Document49 pagesPriyanka New PPT Final 2-1sourabh jakharNo ratings yet
- Syaqiq 094-Lpk EkgDocument6 pagesSyaqiq 094-Lpk EkgEko HarmokoNo ratings yet
- Preboard 28 BDocument7 pagesPreboard 28 BRakeem MarquiseNo ratings yet
- Emergency Drug Box Approved ListDocument1 pageEmergency Drug Box Approved ListGee_anne_Saldi_9627No ratings yet
- Cesarean SectionDocument14 pagesCesarean Sectionمؤمن شطناويNo ratings yet
- KSDP TOG The Obstetric Gynaecologis - 2021 - Ekanem - Surgical Site Infection in Obstetrics and Gynaecology Prevention andDocument14 pagesKSDP TOG The Obstetric Gynaecologis - 2021 - Ekanem - Surgical Site Infection in Obstetrics and Gynaecology Prevention andVu AnNo ratings yet
- US - Recovery - Article - 2021Document8 pagesUS - Recovery - Article - 2021Odett NuñezNo ratings yet
- Hyperbaric Oxygen Therapy For A Pediatric Electrical BurnDocument3 pagesHyperbaric Oxygen Therapy For A Pediatric Electrical Burnsarah iriamanaNo ratings yet
- Spinal Anesthesia in Children With Rectal Premedication With Midazolam, Ketamine and AtropineDocument4 pagesSpinal Anesthesia in Children With Rectal Premedication With Midazolam, Ketamine and AtropineKunal YadavNo ratings yet
- Surface Anatomy of GITDocument15 pagesSurface Anatomy of GITnaseer ahmadNo ratings yet
- Respiratory System Muamar Aldalaeen, RN, Mba, HCRM, Cic, Ipm, MSN, PHD - Haneen Alnuaimi, MSNDocument46 pagesRespiratory System Muamar Aldalaeen, RN, Mba, HCRM, Cic, Ipm, MSN, PHD - Haneen Alnuaimi, MSNAboodsha ShNo ratings yet
- Our Purpose Our Mission Our Solid Strategic Platform: An Emphasis OnDocument2 pagesOur Purpose Our Mission Our Solid Strategic Platform: An Emphasis Onwmturner72No ratings yet
- Bundles in Infection Prevention and SafetyDocument15 pagesBundles in Infection Prevention and SafetyInfectologia DiagnosticaNo ratings yet
- GE Medical Systems Responder AED Pro User ID10626Document35 pagesGE Medical Systems Responder AED Pro User ID10626sermedNo ratings yet