You might also like
- Acute Ankle Sprain - An UpdateDocument7 pagesAcute Ankle Sprain - An UpdateFran Leiva CorreaNo ratings yet
- NATO Intelligence Exploitation of The InternetDocument104 pagesNATO Intelligence Exploitation of The Internetmauro.pennacchietti100% (1)
- AnalogyDocument50 pagesAnalogyNathaniel Campeciño89% (9)
- Esophagus Surgery Lectures: Anatomy, Physiology, Diseases & TreatmentsDocument22 pagesEsophagus Surgery Lectures: Anatomy, Physiology, Diseases & Treatmentsj,007No ratings yet
- SURGERYFinals - 1. The AppendixDocument10 pagesSURGERYFinals - 1. The AppendixRenatoCosmeGalvanJuniorNo ratings yet
- Characteristics of An Effective CounselorDocument5 pagesCharacteristics of An Effective CounselorAbbas KhanNo ratings yet
- Pelvic Floor Ultrasound - A Review - 220211 - 100603Document24 pagesPelvic Floor Ultrasound - A Review - 220211 - 100603Mariana Larroulet SantanderNo ratings yet
- Imperforate Anus and Cloacal MalformationsDocument110 pagesImperforate Anus and Cloacal MalformationsAhmad Abu KushNo ratings yet
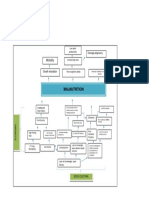
- Problem Tree Analysis MalnutritionDocument1 pageProblem Tree Analysis MalnutritionMho Dsb50% (6)
- Hernia AbdominalisDocument45 pagesHernia AbdominalisFAIRUZ RIFANINo ratings yet
- Audit ChecklistDocument21 pagesAudit ChecklistRob WillestoneNo ratings yet
- Voh Sham Kuch Ajeeb Thi - A Brother Sister Saga (HindiDocument403 pagesVoh Sham Kuch Ajeeb Thi - A Brother Sister Saga (HindiDesi Rocks100% (1)
- JCDR 9 PD26Document2 pagesJCDR 9 PD26ceciliaNo ratings yet
- Spigelian Hernia in A Virgin Abdomen - An Enigmatic Case Report On A Coincidental Finding During Total Laparoscopic HysterectomyDocument4 pagesSpigelian Hernia in A Virgin Abdomen - An Enigmatic Case Report On A Coincidental Finding During Total Laparoscopic HysterectomyIJAR JOURNALNo ratings yet
- Case Report Amayand, S HerniaDocument13 pagesCase Report Amayand, S HerniaJavaidIqbalNo ratings yet
- Bet 4 051Document3 pagesBet 4 051myway999No ratings yet
- Anal FistulasDocument9 pagesAnal FistulasikeernawatiNo ratings yet
- Ultrasound Findings of Appendico-Cecal Invagination: A Case Report and Literature ReviewDocument6 pagesUltrasound Findings of Appendico-Cecal Invagination: A Case Report and Literature Reviewlailan maghfirahNo ratings yet
- AdminDocument5 pagesAdminFirman adiNo ratings yet
- BedahDocument14 pagesBedahRorrieNo ratings yet
- Template 1Document3 pagesTemplate 1Mohd KhalilNo ratings yet
- Bazo Errante 2016 REVISED Ijtra1601084Document4 pagesBazo Errante 2016 REVISED Ijtra1601084luisalfredo_montesNo ratings yet
- Pelvic Organ Prolapse Suspension (POPS) in A Case of Uterine Prolapse With Rectal Prolapse - A Case ReportDocument3 pagesPelvic Organ Prolapse Suspension (POPS) in A Case of Uterine Prolapse With Rectal Prolapse - A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Ssi-Yan-Kai2017Document9 pagesSsi-Yan-Kai2017dw21541No ratings yet
- Hernia Uterine Inguinale: An Uncommon Cause of Pelvic Pain in The Adult Female PatientDocument4 pagesHernia Uterine Inguinale: An Uncommon Cause of Pelvic Pain in The Adult Female PatientJeje MoNo ratings yet
- Laparoscopic Heller Myotomy For Achalasia: Robert N. Cacchione, M.D., Dan N. Tran, M.D., Diane H. Rhoden, M.DDocument5 pagesLaparoscopic Heller Myotomy For Achalasia: Robert N. Cacchione, M.D., Dan N. Tran, M.D., Diane H. Rhoden, M.Dgabriel martinezNo ratings yet
- Conventional and Laparoscopic Epigastric Hernia RepairDocument4 pagesConventional and Laparoscopic Epigastric Hernia RepairOhana S.No ratings yet
- Umbilicalherniarepair TechniqueDocument9 pagesUmbilicalherniarepair Techniqueanz_4191No ratings yet
- Femoral Hernia in MenDocument2 pagesFemoral Hernia in MenSa FariNo ratings yet
- Minilaparoscopic Left Paraduodenal Hernia Repair-A CaseDocument4 pagesMinilaparoscopic Left Paraduodenal Hernia Repair-A CaseAritra PaulNo ratings yet
- Richter Type Spigelian Hernia Mimicking Acute AppendicitisDocument3 pagesRichter Type Spigelian Hernia Mimicking Acute AppendicitisOmar SuleimanNo ratings yet
- Recurrent Infected Mesenteric Cyst Rare Surgical CauseDocument2 pagesRecurrent Infected Mesenteric Cyst Rare Surgical CauseMotivational SpeechNo ratings yet
- Inguino Scrotal ExaminationDocument76 pagesInguino Scrotal Examinationeiuj497No ratings yet
- Retroperitoneal Appendicitis: A Surgical DilemmaDocument2 pagesRetroperitoneal Appendicitis: A Surgical DilemmaputraNo ratings yet
- Indirect Inguinal Hernia Masquerading As A Spigelian HerniaDocument3 pagesIndirect Inguinal Hernia Masquerading As A Spigelian HerniaMuhammad Benny SetiyadiNo ratings yet
- Sabitson - Appendiks EngDocument17 pagesSabitson - Appendiks Engzeek powerNo ratings yet
- Acute Appendicitis Diagnosis and TreatmentDocument3 pagesAcute Appendicitis Diagnosis and TreatmentMavi HayalNo ratings yet
- 1 s2.0 S2210261221012268 MainDocument4 pages1 s2.0 S2210261221012268 Mainzenatihanen123No ratings yet
- Laparoscopic Repair of Perineal Hernia: Jessica Rayhanabad, MD, Pejvak Sassani, MD, Maher A. Abbas, MDDocument5 pagesLaparoscopic Repair of Perineal Hernia: Jessica Rayhanabad, MD, Pejvak Sassani, MD, Maher A. Abbas, MDcleybismarNo ratings yet
- 161004acuteaof Gi - MadridDocument73 pages161004acuteaof Gi - MadridMAPACHE 91No ratings yet
- Proceedings of The Southern European Veterinary Conference and Congreso Nacional AVEPADocument9 pagesProceedings of The Southern European Veterinary Conference and Congreso Nacional AVEPAINDRANo ratings yet
- Torsio Omentum 1Document5 pagesTorsio Omentum 1prabowoaji12No ratings yet
- The 3rd Edition: Prevention & Management: Complications of Laparoscopic Inguinal Hernia RepairDocument5 pagesThe 3rd Edition: Prevention & Management: Complications of Laparoscopic Inguinal Hernia RepairVishnu KumarNo ratings yet
- Williams2013 Article LaparoscopicManagementOfHighTrDocument3 pagesWilliams2013 Article LaparoscopicManagementOfHighTrVishnu priya kokkulaNo ratings yet
- Peritoneal Encapsulation: A Rare Cause of Small Bowel ObstructionDocument3 pagesPeritoneal Encapsulation: A Rare Cause of Small Bowel ObstructionNatalindah Jokiem Woecandra T. D.No ratings yet
- Jurnal Bedah 2Document5 pagesJurnal Bedah 2nafamaulidinaNo ratings yet
- 2.4.5.2.3.a Bowel ObstructionDocument35 pages2.4.5.2.3.a Bowel ObstructionProject ByNo ratings yet
- Imperforate Anus and Cloacal MalformationsDocument23 pagesImperforate Anus and Cloacal MalformationsGwyneth JangadNo ratings yet
- Retroperitoneal Appendicitis: A Surgical Dilemma: Euroasian Journal of Hepato-Gastroenterology January 2013Document3 pagesRetroperitoneal Appendicitis: A Surgical Dilemma: Euroasian Journal of Hepato-Gastroenterology January 2013putraNo ratings yet
- Primary Review: Psoas Abscess: Case of The LiteratureDocument3 pagesPrimary Review: Psoas Abscess: Case of The LiteratureDung Tran HoangNo ratings yet
- Acute Appendicitis: Causes, Symptoms and TreatmentDocument46 pagesAcute Appendicitis: Causes, Symptoms and TreatmentRAJAT DUGGALNo ratings yet
- 2 5 21 861 PDFDocument3 pages2 5 21 861 PDFAhmed ZidanNo ratings yet
- Surgical Treatment of Displaced Abomasum in CattleDocument8 pagesSurgical Treatment of Displaced Abomasum in CattleIkhwanul KhairiaNo ratings yet
- UTD_13_1_74_77Document4 pagesUTD_13_1_74_77Abhishek Soham SatpathyNo ratings yet
- Hérnia tbDocument3 pagesHérnia tbPietra LocatelliNo ratings yet
- Case Report: Laparoscopic Repair of Postoperative Perineal HerniaDocument3 pagesCase Report: Laparoscopic Repair of Postoperative Perineal HerniacleybismarNo ratings yet
- CSS Hernia Inguinalis - SalmaDocument28 pagesCSS Hernia Inguinalis - SalmaNamira PutriNo ratings yet
- Abdominopelvic Ectopic Spleen With A Comprehensive Imaging Examination: A Case ReportDocument6 pagesAbdominopelvic Ectopic Spleen With A Comprehensive Imaging Examination: A Case ReportceciliaNo ratings yet
- Wiitm 7 17104 PDFDocument4 pagesWiitm 7 17104 PDFZam HusNo ratings yet
- APENDICITIS Fischers Mastery of Surgery 7th ING PDFDocument33 pagesAPENDICITIS Fischers Mastery of Surgery 7th ING PDFMichel RamirezNo ratings yet
- Larrey Hernia Complicated With Colonic Obstruction in A 77-Year-Old Woman A Case ReportDocument4 pagesLarrey Hernia Complicated With Colonic Obstruction in A 77-Year-Old Woman A Case ReportAli AjNo ratings yet
- 41 DiverticulDocument7 pages41 DiverticulAndrei KrupaciNo ratings yet
- Spigelian Hernia - Md-Medical Data 2016 8 1 051-053Document3 pagesSpigelian Hernia - Md-Medical Data 2016 8 1 051-053Milan ScepanovicNo ratings yet
- Hernia 2Document8 pagesHernia 2Hamza khalidNo ratings yet
- Laparoscopic Tension Free Mesh Repair in Adult Cases of Diaphragmatic Defects A Series of Four Cases - June - 2020 - 1591105612 - 9229294Document3 pagesLaparoscopic Tension Free Mesh Repair in Adult Cases of Diaphragmatic Defects A Series of Four Cases - June - 2020 - 1591105612 - 9229294Ashish MehraNo ratings yet
- Bretzing y Kulhavy (1981) Note-Taking Passage Style PDFDocument9 pagesBretzing y Kulhavy (1981) Note-Taking Passage Style PDFSergio Andrés Quintero MedinaNo ratings yet
- 2016 UCF Depth ChartDocument1 page2016 UCF Depth ChartBrandon HelwigNo ratings yet
- Primary Year 3 SJK SOWDocument150 pagesPrimary Year 3 SJK SOWJoshua100% (1)
- Commercial Invoice: Exporter/Shipper Importer/ConsigneeDocument1 pageCommercial Invoice: Exporter/Shipper Importer/ConsigneePrem ChanderNo ratings yet
- Tee Cube Collections Catalogue With Google Photos Link PDFDocument4 pagesTee Cube Collections Catalogue With Google Photos Link PDFKirat SinghNo ratings yet
- Calculus Problems Solutions BlogDocument5 pagesCalculus Problems Solutions BlogheeraNo ratings yet
- Jurnal Kebidanan KomunitasDocument5 pagesJurnal Kebidanan KomunitasdeffiNo ratings yet
- DinithDocument102 pagesDinithVishmi amashaNo ratings yet
- Evangelion Cruel Angels Thesis - Moonbase AlphaDocument5 pagesEvangelion Cruel Angels Thesis - Moonbase Alphasionothewil1977100% (1)
- Emerald Emerging Markets Case Studies: Article InformationDocument25 pagesEmerald Emerging Markets Case Studies: Article InformationHannah CastroNo ratings yet
- Automatic Analysis of Annual Financial Reports: A Case StudyDocument11 pagesAutomatic Analysis of Annual Financial Reports: A Case StudyYuliana MargarettaNo ratings yet
- Ambien Withdrawal TreatmentDocument6 pagesAmbien Withdrawal TreatmentSurvival SabariNo ratings yet
- Mama and Mommy and Me in The Middle Press ReleaseDocument2 pagesMama and Mommy and Me in The Middle Press ReleaseCandlewick Press0% (1)
- BengzonDocument5 pagesBengzonmceline19No ratings yet
- Kinematics of MachineDocument4 pagesKinematics of MachineSumit KambleNo ratings yet
- Dokumen - Tips - Ielts and Toefl Made Easy George John Efc and Is The First Coherence PDFDocument2 pagesDokumen - Tips - Ielts and Toefl Made Easy George John Efc and Is The First Coherence PDFPayal SethiNo ratings yet
- Unit 5 Math-Parent Letter-4th GradeDocument4 pagesUnit 5 Math-Parent Letter-4th Gradeapi-346081420No ratings yet
- Jude Sheerin (BBC/Sky - DC) Twitter DM Conversation - @supernanaDocument7 pagesJude Sheerin (BBC/Sky - DC) Twitter DM Conversation - @supernanaAlva FRENCH-N'GUESSANNo ratings yet
- HelloDocument42 pagesHelloSumit KashyapNo ratings yet
- (Appendix C-02) COT-RPMS Rating Sheet For T I-III For SY 2022-2023Document1 page(Appendix C-02) COT-RPMS Rating Sheet For T I-III For SY 2022-2023Michelle Tamayo TimadoNo ratings yet
- GCC Students-IN Unit 5 Travel and TourismDocument3 pagesGCC Students-IN Unit 5 Travel and TourismMuhammad IrzanNo ratings yet
- Tawassulan Fik TjakrabuanaDocument6 pagesTawassulan Fik TjakrabuanafikditasresNo ratings yet