You might also like
- Comm 210 Persuasive Speech OutlineDocument8 pagesComm 210 Persuasive Speech Outlineapi-269568046No ratings yet
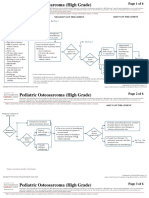
- CA Treatment Osteosarcoma Pedi Web AlgorithmDocument6 pagesCA Treatment Osteosarcoma Pedi Web AlgorithmyaseenNo ratings yet
- Ca - Treatment-Breast-Inflammatory-Web-AlgorithmDocument19 pagesCa - Treatment-Breast-Inflammatory-Web-AlgorithmAgustin SierraNo ratings yet
- Carcinoma de OvarioDocument7 pagesCarcinoma de OvarioNicolás BertachiniNo ratings yet
- Ca Treatment Rectal Web AlgorithmDocument17 pagesCa Treatment Rectal Web AlgorithmPatrick JohnNo ratings yet
- Ca Treatment Prostate Web AlgorithmDocument12 pagesCa Treatment Prostate Web AlgorithmCalvinNo ratings yet
- Cancer of The Endometrium PDFDocument6 pagesCancer of The Endometrium PDFYanita BetraNo ratings yet
- CA Treatment Leptomeningeal Web AlgorithmDocument5 pagesCA Treatment Leptomeningeal Web Algorithmsugoiman100% (1)
- Surgery PearlsDocument2 pagesSurgery Pearlspatriciaatan1497No ratings yet
- PearlsDocument2 pagesPearlspatriciaatan1497No ratings yet
- PREOPinguinalherniaDocument2 pagesPREOPinguinalherniapatriciaatan1497No ratings yet
- CA Treatment Small Cell Web AlgorithmDocument8 pagesCA Treatment Small Cell Web AlgorithmbharatNo ratings yet
- Surgery PearlsDocument2 pagesSurgery Pearlspatriciaatan1497No ratings yet
- Cancer de Mama y EmbarazoDocument5 pagesCancer de Mama y EmbarazoNicolás BertachiniNo ratings yet
- كتاب التمريض الجديد2022Document206 pagesكتاب التمريض الجديد2022mohamed mohamedNo ratings yet
- AUA Guideline Testicular CancerDocument1 pageAUA Guideline Testicular CancerMarco Túlio La Guardia PiresNo ratings yet
- Ca Treatment Breast Noninvasive Web AlgorithmDocument8 pagesCa Treatment Breast Noninvasive Web AlgorithmAgustin SierraNo ratings yet
- Esofago Carvical Valmasoni 2018Document9 pagesEsofago Carvical Valmasoni 2018Carlos N. Rojas PuyolNo ratings yet
- Protocol Update Dec 2019Document13 pagesProtocol Update Dec 2019Aarzu ChoudharyNo ratings yet
- Breast Cancer Protocol (Version Date 10-JAN-2018)Document11 pagesBreast Cancer Protocol (Version Date 10-JAN-2018)Eugène NkusiNo ratings yet
- Ca Treatment Breast Invasive Web AlgorithmDocument27 pagesCa Treatment Breast Invasive Web AlgorithmAgustin SierraNo ratings yet
- Reproducible Quantification in PET - CT: Clinical Relevance and Technological ApproachesDocument28 pagesReproducible Quantification in PET - CT: Clinical Relevance and Technological ApproachesFandoNo ratings yet
- 3 - NCM112Document6 pages3 - NCM112Edthel IniegoNo ratings yet
- Abdomen Blunt Trauma 2 - 3 - 2020Document6 pagesAbdomen Blunt Trauma 2 - 3 - 2020Iqra NazNo ratings yet
- GA SA Miss AiniDocument34 pagesGA SA Miss AiniAmirul Zakiya BraveryNo ratings yet
- Rectal CA JurnalDocument19 pagesRectal CA JurnalkavinNo ratings yet
- RT ArticuloDocument13 pagesRT ArticulojorgeaznarNo ratings yet
- Guia No. 109-Hysterectomy Sogclefebvre2018Document13 pagesGuia No. 109-Hysterectomy Sogclefebvre2018Raul A UrbinaNo ratings yet
- Ahn2008 Article ClinicopathologicalFeaturesAndDocument8 pagesAhn2008 Article ClinicopathologicalFeaturesAndXavier QuinteroNo ratings yet
- Ca Treatment Paget S Web AlgorithmDocument4 pagesCa Treatment Paget S Web AlgorithmAgustin SierraNo ratings yet
- Allen2021 Article ChemotherapyVersusChemotherapyDocument8 pagesAllen2021 Article ChemotherapyVersusChemotherapyXavier QuinteroNo ratings yet
- Oncology OverviewDocument42 pagesOncology OverviewХина КападиаNo ratings yet
- Cardiac Involvement in Non-Hodgkin Lymphoma, An Incidental Large Atrial Mass: A Case ReportDocument4 pagesCardiac Involvement in Non-Hodgkin Lymphoma, An Incidental Large Atrial Mass: A Case Reportkhansa salsabilaNo ratings yet
- Adjuvant RT in GB Cancer - JCRTDocument5 pagesAdjuvant RT in GB Cancer - JCRTneha guptaNo ratings yet
- Eddy 2007Document8 pagesEddy 2007Mimsy Quiñones TafurNo ratings yet
- If HP Cancer Guide Gu001 TesticularDocument23 pagesIf HP Cancer Guide Gu001 TesticularwidyaputraNo ratings yet
- Linee Guida ESMODocument2 pagesLinee Guida ESMODPNo ratings yet
- Dr. Manoj GuptaDocument36 pagesDr. Manoj GuptaafshanNo ratings yet
- CPG Early and Locally Advanced Non-Small-Cell LungDocument6 pagesCPG Early and Locally Advanced Non-Small-Cell LungJess PeltraNo ratings yet
- SupremoDocument82 pagesSupremoRaul Matute MartinNo ratings yet
- PCRmarcador COLECISTITIS2019Document7 pagesPCRmarcador COLECISTITIS2019Daniela VahlisNo ratings yet
- GTD Hour AprilDocument26 pagesGTD Hour AprilGerben VillanuevaNo ratings yet
- Ca Treatment Breast Noninvasive Web AlgorithmDocument6 pagesCa Treatment Breast Noninvasive Web Algorithmmarcelo chavez diazNo ratings yet
- Jurnal GastroDocument24 pagesJurnal Gastronurul haeraniNo ratings yet
- 【一般】Journal readingDocument28 pages【一般】Journal readingCY PNo ratings yet
- NCCN Practice Guidelines Narrative Summary of Indications For FDG PET and PET/CTDocument8 pagesNCCN Practice Guidelines Narrative Summary of Indications For FDG PET and PET/CTdeoNo ratings yet
- Ha Vital-Signs Hidalgo 2Document23 pagesHa Vital-Signs Hidalgo 2MERAZOLE PACA-ANASNo ratings yet
- Impact of Surgical Margins On Overall Survival After Gastrectomy For Gastric Cancer: A Validation of Japanese Gastric Cancer Association Guidelines On A Western SeriesDocument13 pagesImpact of Surgical Margins On Overall Survival After Gastrectomy For Gastric Cancer: A Validation of Japanese Gastric Cancer Association Guidelines On A Western SeriesХулан ХүрэлбаатарNo ratings yet
- Negen Born 2018Document10 pagesNegen Born 2018salyouhaNo ratings yet
- Blunt Abdominal TraumaDocument11 pagesBlunt Abdominal TraumaRahmat SyahiliNo ratings yet
- Nakachi 2018Document4 pagesNakachi 2018Nikos SerifisNo ratings yet
- Panc Adenocarcinoma Recent Data and Perspective JR Delpero HPB Course 2022 V4-NuoveDocument176 pagesPanc Adenocarcinoma Recent Data and Perspective JR Delpero HPB Course 2022 V4-NuoveDiana MitreaNo ratings yet
- Assessment and Management of Delirium in Pediatric PatientsDocument7 pagesAssessment and Management of Delirium in Pediatric PatientsEunike Karamoy100% (1)
- Granulomatous Lobular Mastitis: Original ArticlesDocument5 pagesGranulomatous Lobular Mastitis: Original ArticlesFirdillaQonitaFirodiyaRobbyNo ratings yet
- Neoadjuvant Chemoradiotherapy Plus Surgery Versus Surgery Alone For Oesophageal or Junctional Cancer (CROSS) Long-Term Results of A Randomised Controlled TrialDocument9 pagesNeoadjuvant Chemoradiotherapy Plus Surgery Versus Surgery Alone For Oesophageal or Junctional Cancer (CROSS) Long-Term Results of A Randomised Controlled TrialSergioNo ratings yet
- London Cancer Head and Neck Radiotherapy Protocol March 2013Document10 pagesLondon Cancer Head and Neck Radiotherapy Protocol March 2013handrionoNo ratings yet
- Rtog1005 Protocol PresentationDocument9 pagesRtog1005 Protocol Presentationapi-634067897No ratings yet
- 010 Hyr011Document4 pages010 Hyr011Maher GamingNo ratings yet
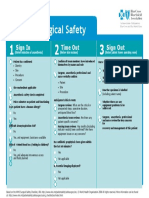
- Surgical Safety: Sign in Time Out Sign OutDocument1 pageSurgical Safety: Sign in Time Out Sign OutNathanNo ratings yet
- Righ Choise TrialDocument17 pagesRigh Choise TrialOscar FloresNo ratings yet
- Rectal Cancer: International Perspectives on Multimodality ManagementFrom EverandRectal Cancer: International Perspectives on Multimodality ManagementBrian G. CzitoNo ratings yet
- The Effects of Climate Variability On The Choices of Livelihood Among Farm Households in Anambra State, NigeriaDocument103 pagesThe Effects of Climate Variability On The Choices of Livelihood Among Farm Households in Anambra State, NigeriaEVELYN EZEKWENo ratings yet
- Common Problems in Acute Care Surgery 2nbsped 9783319427904 3319427903 9783319427928 331942792x - CompressDocument493 pagesCommon Problems in Acute Care Surgery 2nbsped 9783319427904 3319427903 9783319427928 331942792x - CompressEVELYN EZEKWE100% (1)
- Balogh 1Document95 pagesBalogh 1EVELYN EZEKWENo ratings yet
- Untitled Form (Responses)Document28 pagesUntitled Form (Responses)EVELYN EZEKWENo ratings yet
- Textbook of Plastic, Reconstructive, and Aesthetic SurgeryDocument2 pagesTextbook of Plastic, Reconstructive, and Aesthetic SurgeryEVELYN EZEKWENo ratings yet
- Jco.2022.40.16 Suppl.e14002Document1 pageJco.2022.40.16 Suppl.e14002hamzaNo ratings yet
- 1chemo - Scenarios - Chapter 1Document6 pages1chemo - Scenarios - Chapter 1Esmareldah Henry SirueNo ratings yet
- Stem - Cells - and - Cancer - PPT 1Document31 pagesStem - Cells - and - Cancer - PPT 1Muhammad Ikram RabbaniNo ratings yet
- How I Treat Mixed-Phenotype Acute LeukemiaDocument9 pagesHow I Treat Mixed-Phenotype Acute LeukemiaFachitah AndrianicNo ratings yet
- CME Palliative Medicine (126358) : Self-Assessment QuestionnaireDocument2 pagesCME Palliative Medicine (126358) : Self-Assessment Questionnairealialison7666No ratings yet
- Dermoscopy ChallengeDocument2 pagesDermoscopy ChallengegongutzNo ratings yet
- Alveolar Rhabdomyosarcoma of The Hand: A Very Rare Case of Soft Tissue SarcomaDocument4 pagesAlveolar Rhabdomyosarcoma of The Hand: A Very Rare Case of Soft Tissue Sarcomahannatambun24No ratings yet
- Breast CarcinomasDocument19 pagesBreast CarcinomasGirkati ShivaniNo ratings yet
- Consensus On The Pathological Definition and Classification of Poorly Cohesive Gastric CarcinomaDocument9 pagesConsensus On The Pathological Definition and Classification of Poorly Cohesive Gastric CarcinomaMariangel FloresNo ratings yet
- By: Vismin Prince Magno: Liver CancerDocument17 pagesBy: Vismin Prince Magno: Liver Cancerhedokido100% (1)
- Palliative Care in Patients With Severe Mental Illness: Case 1Document3 pagesPalliative Care in Patients With Severe Mental Illness: Case 1Cristian Vale VarelaNo ratings yet
- Locaaly Advanced Cervical CancerDocument50 pagesLocaaly Advanced Cervical CancerMichaelNo ratings yet
- Endometrial Carcinoma: Amina Adel Al-QaysiDocument42 pagesEndometrial Carcinoma: Amina Adel Al-Qaysitaufik perdanaNo ratings yet
- Prostate CancerDocument12 pagesProstate CancerSaloni PatelNo ratings yet
- Hosneara Begum - Aastha ConcentDocument2 pagesHosneara Begum - Aastha ConcentAbul HasnatNo ratings yet
- SCORE de GLEASON - Pathology OutlinesDocument18 pagesSCORE de GLEASON - Pathology OutlineslucasantoniofernandeNo ratings yet
- GemcitabineDocument6 pagesGemcitabineCaballero X CaballeroNo ratings yet
- Molecular Sciences. 2020Document4 pagesMolecular Sciences. 2020Dyerik LilingNo ratings yet
- HSS Dysphagia and Dysphonia Inventory (HSS-DDI) Following Anterior Cervical FusionDocument10 pagesHSS Dysphagia and Dysphonia Inventory (HSS-DDI) Following Anterior Cervical FusionLarissa MeloNo ratings yet
- Diagnostic Approach of Malignant Lesions in The Jaws PDFDocument1 pageDiagnostic Approach of Malignant Lesions in The Jaws PDFmahnoorNo ratings yet
- Onco 4 Prostate CancerDocument30 pagesOnco 4 Prostate CancerTej Narayan Yadav100% (1)
- Paras ProtocolDocument14 pagesParas Protocolparas yadavNo ratings yet
- Recent Advances in The Management of LiposarcomaDocument15 pagesRecent Advances in The Management of LiposarcomaBudhiNo ratings yet
- Anti Cancer DrugsDocument4 pagesAnti Cancer Drugsnerdo1999No ratings yet
- Cervical CancerDocument23 pagesCervical CancerShinal ChandNo ratings yet
- Childhood Cancer Resources Directory Asia - Final v170908Document35 pagesChildhood Cancer Resources Directory Asia - Final v170908Anna VieeNo ratings yet
- Week 10 Discussion SectionDocument14 pagesWeek 10 Discussion Sectionwriter topNo ratings yet
- Pretest Onco Key (May 2024) 1Document1 pagePretest Onco Key (May 2024) 1Nathan BuhawiNo ratings yet
- Liver CancerDocument4 pagesLiver CancerZhyraine Iraj D. CaluzaNo ratings yet