You might also like
- Routine Blood Results Explained 3/e: A guide for Nurses & Allied Health ProfessionalsFrom EverandRoutine Blood Results Explained 3/e: A guide for Nurses & Allied Health ProfessionalsRating: 3 out of 5 stars3/5 (2)
- Diagnostic Exam Answer KeyDocument38 pagesDiagnostic Exam Answer KeyGlen DizonNo ratings yet
- Capillary Puncture Equipment and ProcedureDocument3 pagesCapillary Puncture Equipment and ProcedureSieg100% (1)
- Anesthesiology 2015Document11 pagesAnesthesiology 2015The Vancouver SunNo ratings yet
- Comparison of Point-of-Care Measurement of Electrolyte Concentrations On Calculations of The Anion Gap and The Strong Ion DifferenceDocument8 pagesComparison of Point-of-Care Measurement of Electrolyte Concentrations On Calculations of The Anion Gap and The Strong Ion DifferenceMuhammad DaffaNo ratings yet
- Hematocrit - StatPearls - NCBI BookshelfDocument4 pagesHematocrit - StatPearls - NCBI BookshelfVincent ReyesNo ratings yet
- HarrisADVIA2120methods LabHema2005 11 47-61 PDFDocument16 pagesHarrisADVIA2120methods LabHema2005 11 47-61 PDFedu_14cNo ratings yet
- AnnCardAnaesth9144-7552051 020552Document5 pagesAnnCardAnaesth9144-7552051 020552Imanuel Far-FarNo ratings yet
- HarrisADVIA2120methods LabHema2005 11 47-61 PDFDocument16 pagesHarrisADVIA2120methods LabHema2005 11 47-61 PDFSilvânia RochaNo ratings yet
- Less Invasive Hemodynamic Monitoring in Critically Ill PatientsDocument11 pagesLess Invasive Hemodynamic Monitoring in Critically Ill Patientsهبة بسمان شاكرNo ratings yet
- Hematocrit (HCT) : June 2019Document7 pagesHematocrit (HCT) : June 2019لطيفة نورNo ratings yet
- Hepatology - 2004 - Colle - Diagnosis of Portopulmonary Hypertension in Candidates For Liver Transplantation A ProspectiveDocument9 pagesHepatology - 2004 - Colle - Diagnosis of Portopulmonary Hypertension in Candidates For Liver Transplantation A ProspectiveYasin DeveliogluNo ratings yet
- Peripheral Blood Smear Pathologist ToolDocument3 pagesPeripheral Blood Smear Pathologist ToolSimon HafeniNo ratings yet
- Zhang 2000Document6 pagesZhang 2000hoangkiett0904No ratings yet
- Principles and Techniques of Blood Pressure MeasurementDocument26 pagesPrinciples and Techniques of Blood Pressure MeasurementWagnerNo ratings yet
- Prediction of Hyperkalemia in ESRD Patients by Identification of Multiple Leads and Multiple Features On ECGDocument11 pagesPrediction of Hyperkalemia in ESRD Patients by Identification of Multiple Leads and Multiple Features On ECG8ctvnvpbnpNo ratings yet
- Journal of Cardiothoracic and Vascular Anesthesia: Original ArticleDocument11 pagesJournal of Cardiothoracic and Vascular Anesthesia: Original ArticleRicardoNo ratings yet
- Hema Activity 3Document5 pagesHema Activity 3Nico LokoNo ratings yet
- AARC Clinical Practice Guideline Blood Gas Analysis and Hemoximetry 2013.Document14 pagesAARC Clinical Practice Guideline Blood Gas Analysis and Hemoximetry 2013.Madalina TalpauNo ratings yet
- Platelet Counting by The Coulter LH 750, Sysmex XE 2100Document7 pagesPlatelet Counting by The Coulter LH 750, Sysmex XE 2100blanket_thNo ratings yet
- Cost Analysis of A Neonatal Point-of-Care MonitorDocument10 pagesCost Analysis of A Neonatal Point-of-Care MonitorMARIO LOPEZ VILLAMILNo ratings yet
- Potential of Cell Tracking Velocimetry As An Economical and Portable Hematology Analyzer.Document13 pagesPotential of Cell Tracking Velocimetry As An Economical and Portable Hematology Analyzer.Lizet SantacruzNo ratings yet
- DR Preeti Mansukhani - CBC 5 Parts - 2017Document56 pagesDR Preeti Mansukhani - CBC 5 Parts - 2017Silence T-jmNo ratings yet
- IndianJPatholOncol 7 4 625 630Document6 pagesIndianJPatholOncol 7 4 625 630Yaser MNo ratings yet
- 2023 PlosOne ArvinHSoeproatnaDocument25 pages2023 PlosOne ArvinHSoeproatnaTKimNo ratings yet
- Hema I Chapter 10 - PCVDocument24 pagesHema I Chapter 10 - PCVchris andrieNo ratings yet
- SaudiJKidneyDisTranspl252438-4286359 115423Document6 pagesSaudiJKidneyDisTranspl252438-4286359 115423yosefNo ratings yet
- Technical College of Applied Sciences Medical Laboratory Science First Stage - Second Semester Lab Technic ReportDocument9 pagesTechnical College of Applied Sciences Medical Laboratory Science First Stage - Second Semester Lab Technic ReportELYANNo ratings yet
- Cytologic and Hematologic Tests Arterial Blood Gases: Medical Background: Chronic Restrictive Pulmonary DiseaseDocument7 pagesCytologic and Hematologic Tests Arterial Blood Gases: Medical Background: Chronic Restrictive Pulmonary Diseasejoanna gurtizaNo ratings yet
- Introduction To Lateral Flow Speedy Test DiagnosticsDocument3 pagesIntroduction To Lateral Flow Speedy Test DiagnosticsryalasfycoNo ratings yet
- Assignment2 NamocDocument5 pagesAssignment2 NamocHenry Darius NamocNo ratings yet
- Thesis Heart FailureDocument8 pagesThesis Heart Failurebspq3gma100% (2)
- (Q1) Pone.0169593Document16 pages(Q1) Pone.0169593wiradewi lestariNo ratings yet
- Limited Face-To-Face Module (Central Lab)Document3 pagesLimited Face-To-Face Module (Central Lab)Junah BigorniaNo ratings yet
- Hemolysis in Serum Samples Drawn by Emergency Department Personnel Versus Laboratory PhlebotomistsDocument3 pagesHemolysis in Serum Samples Drawn by Emergency Department Personnel Versus Laboratory PhlebotomistsmuhammadhanifmohdfahmiNo ratings yet
- Erythrocyte Sedimentation Rate Journey Verifying A New Method For An Imperfect TestDocument3 pagesErythrocyte Sedimentation Rate Journey Verifying A New Method For An Imperfect TestRina ErlinaNo ratings yet
- Int J Lab Hematology - 2021 - Kitchen - International Council For Standardization in Haematology ICSH Recommendations ForDocument12 pagesInt J Lab Hematology - 2021 - Kitchen - International Council For Standardization in Haematology ICSH Recommendations ForLaboratorium RS BELLANo ratings yet
- Hematocrit (HCT) : Publication DetailsDocument7 pagesHematocrit (HCT) : Publication DetailsPutri SyarifaniNo ratings yet
- Monitoring of Critically Ill Patient Presented byDocument12 pagesMonitoring of Critically Ill Patient Presented byMansi PatelNo ratings yet
- Five-Part Hematology AnalyzerDocument78 pagesFive-Part Hematology Analyzerswaraj sharmaNo ratings yet
- Validation and standardization of blood cell countersDocument15 pagesValidation and standardization of blood cell countersPaul Avelino CallupeNo ratings yet
- Optimal Blood Pressure During CPBDocument7 pagesOptimal Blood Pressure During CPBAdy WarsanaNo ratings yet
- Stability of whole blood samples for haematological measurementsDocument2 pagesStability of whole blood samples for haematological measurementssabin shaikNo ratings yet
- Fellows Forum: Pediatrics, Texas Children's Hospital/Baylor College of Medicine, Houston, Tex, USADocument8 pagesFellows Forum: Pediatrics, Texas Children's Hospital/Baylor College of Medicine, Houston, Tex, USAalexNo ratings yet
- Monitoring of Critically Ill PatientDocument11 pagesMonitoring of Critically Ill PatientAnusikta PandaNo ratings yet
- Automated Hematology Cell CountersDocument53 pagesAutomated Hematology Cell CountersFidaa Jaafrah100% (2)
- Verification and Standardization of Blood Cell Counters For Routine Clinical Laboratory TestsDocument15 pagesVerification and Standardization of Blood Cell Counters For Routine Clinical Laboratory TestsLorena Ek MaciasNo ratings yet
- 7: Effective Transfusion in Surgery and Critical CareDocument16 pages7: Effective Transfusion in Surgery and Critical CareNick-Hugh Sean WisdomNo ratings yet
- Journal Critique Technical MethodsDocument4 pagesJournal Critique Technical MethodsJam SalazarNo ratings yet
- bb5 ClassifsofttissueDocument5 pagesbb5 ClassifsofttissueMuhammad MaulanaNo ratings yet
- Int J Lab Hematology - 2007 - ZANDECKI - Spurious Counts and Spurious Results On Haematology Analysers A Review Part IDocument17 pagesInt J Lab Hematology - 2007 - ZANDECKI - Spurious Counts and Spurious Results On Haematology Analysers A Review Part IYangnuu TitusNo ratings yet
- Manajemen RsDocument9 pagesManajemen RsYenni ElfiraNo ratings yet
- Artículo 5Document10 pagesArtículo 5everildoNo ratings yet
- Echocardiography in Hemodynamic MonitoringDocument5 pagesEchocardiography in Hemodynamic MonitoringDr.Biswajit jenaNo ratings yet
- Pressure and Flow MeasurementsDocument25 pagesPressure and Flow Measurements윤원용No ratings yet
- Automation in HematologyDocument75 pagesAutomation in HematologyDann Francis Sarnillo50% (2)
- Lippi 2018Document6 pagesLippi 2018Harika PutraNo ratings yet
- Clinical Review: Update On Hemodynamic Monitoring - A Consensus of 16Document8 pagesClinical Review: Update On Hemodynamic Monitoring - A Consensus of 16KumarNo ratings yet
- AARC Clinical Practice Guideline Blood Gas Analysis and Hemoximetry: 2013Document10 pagesAARC Clinical Practice Guideline Blood Gas Analysis and Hemoximetry: 2013jvalenciagNo ratings yet
- Packed Cell Volume (PCV)Document24 pagesPacked Cell Volume (PCV)Eyasu demsewNo ratings yet
- Ijlh 12503Document11 pagesIjlh 12503MUCHLISOH ZULAEHANo ratings yet
- Evaluation of The Effect of Temperature and Time of Incubation On Complete Blood Count (CBC) TestsDocument4 pagesEvaluation of The Effect of Temperature and Time of Incubation On Complete Blood Count (CBC) TestsYaser MNo ratings yet
- Conduct of Cardiovascular PerfusionDocument24 pagesConduct of Cardiovascular PerfusionBranka KurtovicNo ratings yet
- Compre-5-Supplementary-Lecture 3Document32 pagesCompre-5-Supplementary-Lecture 3Aubrey Jane TagolinoNo ratings yet
- CBCDocument3 pagesCBCDicky DamaraNo ratings yet
- Test Bank For Rodaks Hematology 5th Edition by KeohaneDocument33 pagesTest Bank For Rodaks Hematology 5th Edition by Keohanegainerhanukkah.zv28wx100% (38)
- Week 7-9 Module (Hema 1 Laboratory)Document25 pagesWeek 7-9 Module (Hema 1 Laboratory)Jam RamosNo ratings yet
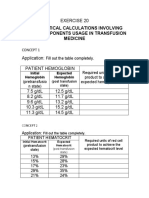
- Mathematical Calculations Involving Blood Components Usage in Transfusion MedicineDocument8 pagesMathematical Calculations Involving Blood Components Usage in Transfusion MedicineNatalie CuNo ratings yet
- POLYCYTHEMIADocument29 pagesPOLYCYTHEMIAFaizan KhanNo ratings yet
- All Objectives HematologyDocument45 pagesAll Objectives HematologyNursing200980% (5)
- SuriDocument5 pagesSurikevins chiloNo ratings yet
- Bishop 2001 RheologicalEffectsRBCDocument13 pagesBishop 2001 RheologicalEffectsRBCAfkir HamzaNo ratings yet
- BioBuild Desert CrossingDocument8 pagesBioBuild Desert CrossingSubbaraju GvNo ratings yet
- Laboratory Tests InterpretationDocument12 pagesLaboratory Tests InterpretationKaloy Kamao100% (1)
- Equipment Specification SL-1Document21 pagesEquipment Specification SL-1Ibrahim KamaraNo ratings yet
- Case Study Pre-EclampsiaDocument51 pagesCase Study Pre-EclampsiaRomelle Jane M. VelascoNo ratings yet
- Piscicide Effects of Mahua Oil Cake From The Finfish Culture SystemDocument7 pagesPiscicide Effects of Mahua Oil Cake From The Finfish Culture SystemEditor IJTSRDNo ratings yet
- Kim1985 PDFDocument7 pagesKim1985 PDFfadwa lachkerNo ratings yet
- The Effect of High Temperature On The Hematological Parameters of Bakery WorkersDocument4 pagesThe Effect of High Temperature On The Hematological Parameters of Bakery WorkersYaser MNo ratings yet
- XN Cal TraceabilityDocument5 pagesXN Cal TraceabilityAnonymous brvvLxoIluNo ratings yet
- Case PresentationDocument43 pagesCase PresentationSusan Albaran IraganaNo ratings yet
- Critical Care Monitoring Made Simple with System MDocument26 pagesCritical Care Monitoring Made Simple with System MTravis DayNo ratings yet
- Measuring Whole Blood Viscosity with a MicroviscometerDocument5 pagesMeasuring Whole Blood Viscosity with a MicroviscometerSanda Pyae SoneNo ratings yet
- Medical Laboratory SIWES ReportDocument27 pagesMedical Laboratory SIWES ReportElias Samuel UnekwuNo ratings yet
- Normal Laboratory ValuesDocument5 pagesNormal Laboratory ValuesensooooooooooNo ratings yet
- CelQuant 3i User Manual & Operational Guide PDFDocument49 pagesCelQuant 3i User Manual & Operational Guide PDFKeigo ChewNo ratings yet
- Dengue Fever Case StudyDocument28 pagesDengue Fever Case StudyAnastasya Gishella RorongNo ratings yet
- Complete Blood Count PPT PresentationDocument15 pagesComplete Blood Count PPT PresentationShelley Ann Badayos0% (1)
- Xenotransfusion of Canine Blood To A CatDocument3 pagesXenotransfusion of Canine Blood To A CatFelipe GonzalezNo ratings yet
- Dongzal-MLS - Classification of LabDocument2 pagesDongzal-MLS - Classification of LabShin DongzalNo ratings yet