Professional Documents
Culture Documents
CDC Covid Vax Report FOIA Response
Uploaded by
walkafyre0 ratings0% found this document useful (0 votes)
741 views417 pagesCDC Covid Vax Report FOIA Response
Copyright
© Public Domain
Available Formats
PDF or read online from Scribd
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCDC Covid Vax Report FOIA Response
Copyright:
Public Domain
Available Formats
Download as PDF or read online from Scribd
0 ratings0% found this document useful (0 votes)
741 views417 pagesCDC Covid Vax Report FOIA Response
Uploaded by
walkafyreCDC Covid Vax Report FOIA Response
Copyright:
Public Domain
Available Formats
Download as PDF or read online from Scribd
You are on page 1of 417
Lee, Man
Mon, 1 Nov 2021 17:05:33 -0400
Bozio, Catherine H. (CDC/DDID/NCIRD/ID)
‘A few questions on recent early release
Dr. Bozio,
Tam a 4th year pharmacy student out of Campbell University in North Carolina and enjoyed
reading the early release of "Laboratory-Confirmed COVID-19 Among Adults Hospitalized with COVID-19-
Like Illness with Infection-Induced or mRNA Vaccine-Induced SARS-CoV-2 Immunity”. [had a few questions that
Thope you can help answer. [will be presenting this study to a group of hospital providers.
1) How were the adjusted odds ratios weighted”
2) Would you be able to send me a copy of the supplemental index?
3) Do you have any data on the following comorbidities diabetes, hypertension, COPD and obesity for each group?
4) Do you have an age breakdown forall the eovi jve? The ones in the study lists
those that tested both positive and negative.
Like illnesses that were eovid po:
| thank you in advance for your time and hope to hear back soon. Thank you again.
Respectilly,
Man Lee
Tumpey, Abbigail (CDC/DDPHSS/CSELS/OD)
Fri, 29 Oct 2021 14:40:58 +0000
Mahon, Barbara (CDC/DDID/NCIRD/OD); Kent, Charlotte
(CDC/DDPHSS/CSELS/OD); Braden, Chris (CDC/DDID/NCEZID/OD); Branam, lan
(CDC/DDPHSS/CSELS/OD); Bozio, Catherine H. (CDC/DDID/NCIRD/ID); Hall, Aron (CDC/DDID/NCIRD/DVD)
Ce: CDC IMS JIC Lead -2; Turner Hoffman, Katherine (Kat) (CDC/DDPHSS/CSELS/OD}
Choban, Ana (CDC/DDID/NCIRD/ID); Fisher, Angela H. (CDC/DDPHSS/CSELS/OD)
Subject: Clean MMWR messaging
Attachments: COVID-19 Comms Rollout - Immunity MMWR_10282021 v2.docx.
Great! Here isa clean, hard copy version of the MMWR messaging.
Thanks to everyone for the very helpful pivot this AM.
Regards,
Abbigail
From: Mahon, Barbara (CDC/DDID/NCIRD/OD)
Sent: Friday, October 29, 2021 10:24 AM
‘To: Tumpey, Abbigail (CDC/DDPHSS/CSELS/OD) ; Kent, Charlotte
(CDC/DDPHSS/CSELS/OD) ; Braden, Chris (CDC/DDID/NCEZID/OD) ;
Branam, lan (CDC/DDPHSS/CSELS/OD) ; Bozio, Catherine H. (CDC/DDID/NCIRD/ID)
; Hall, Aron (CDC/DDID/NCIRD/DVD)
Cc: CDC IMS JIC Lead -2 ; Turner Hoffman, Katherine (Kat)
(CDC/DDPHSS/CSELS/OD) ; Choban, Ana (CDC/DDID/NCIRD/ID) ; Fisher,
Angela H. (CDC/DDPHSS/CSELS/OD)
Subject: RE: Need Quick Check: MMWR messaging,
That works for me.
From: Tumpey, Abbigail (COC/DDPHSS/CSELS/0D)
Sent: Friday, October 29, 2021 10:02 AM
To: Mahon, Barbara (CDC/DDID/NCIRD/OD) ; Kent, Charlotte
(CDC/DDPHSS/CSELS/OD) ; Braden, Chris (CDC/ODID/NCEZID/OD) ;
Branam, lan (CDC/DDPHSS/CSELS/OD) ; Bozio, Catherine H. (CDC/DDID/NCIRD/ID)
; Hall, Aron (CDC/DDID/NCIRD/OVD)
Cc: CDC IMS JIC Lead -2 ; Turner Hoffman, Katherine (Kat)
(CDC/DDPHSS/CSELS/OD) ; Choban, Ana (CDC/DDID/NCIRD/ID) ; Fisher,
Angela H. (CDC/DDPHSS/CSELS/0D)
Subject: RE: Need Quick Check: MMWR messaging,
Good catches all WE JAll good? Clean
version at same link
eyo)
From: Mahon, Barbara (CDC/DDID/NCIRD/OD)
Sent: Friday, October 29, 2021 8:56 AM
‘To: Tumpey, Abbigail (CDC/DDPHSS/CSELS/OD) ; Kent, Charlotte
(CDC/DDPHSS/CSELS/OD) ; Braden, Chris (COC/DDID/NCEZID/OD) ;
Branam, lan (CDC/DDPHSS/CSELS/OD) ; Bozio, Catherine H. (CDC/DDID/NCIRD/ID)
; Hall, Aron (CDC/DDID/NCIRD/DVD)
Ce: CDC IMSJIC Lead -2 ; Turner Hoffman, Katherine (Kat)
(COC/DOPHSS/CSELS/OD) ; Choban, Ana (CDC/DDID/NCIRD/I0) ; Fisher,
Angela H. (CDC/DDPHSS/CSELS/OD)
Subject: RE: Need Quick Check: MMWR messaging
Hi Abbigall,
Have made some suggested edits, er
©
Barbara
From: Tumpey, Abbigail (CDC/DDPHSS/CSELS/0D)
Sent: Friday, October 29, 2022 8:25 AM
To: Kent, Charlotte (CDC/DDPHSS/CSELS/OD) ; Mahon, Barbara (CDC/DDID/NCIRD/OD)
; Braden, Chris (CDC/DDID/NCEZID/OD) ; Branam, lan
(CDC/DDPHSS/CSELS/OD) ; Bozio, Catherine H. (CDC/DDID/NCIRD/I0) ;
Hall, Aron (CDC/DDID/NCIRD/DVD)
Ce: CDC IMS JIC Lead -2 ; Turner Hoffman, Katherine (Kat)
(CDC/DDPHSS/CSELS/OD) ; Choban, Ana (CDC/DDID/NCIRD/ID) ; Fisher,
Angela H. (CDC/DDPHSS/CSELS/0D)
Subject: Need Quick Check: MMWR messaging
Colleagues,
Now that the MMWR is going earlier than the Science Brief, we changed the messaging to focus just on
the MMWR.
Can you all double check the accuracy?? Possible to tell me by Sam??
F)covp-19 comms Rollout - immunity MMWR 10282021 v2.docx
Thanks to lan for his leadership and help here.
Regards,
Abbigail
Abbigail Tumpey, MPH CHES
Acting Associate Director for Communication
Centers for Disease Control and Prevention
11600 Clifton Rd. NE
Atlanta, GA
Phone: 404-639-1125
Cell: 404-259-7064
Email: atumpey@cdc.gov
pene
Steve McConnell
Tue, 2 Nov 2021 17:42:09 +0000
Bozio, Catherine H. (CDC/DDID/NCIRD/ID)
Subject: Comment on "Laboratory-Confirmed COVID-19 Among Adults Hospitalized with
COVID-19-Like IlIness with Infection"
Dear Dr. Bozio,
head one of the teams that submits Covid-19 death forecasts into the CDC's forecast hub.
tread with great interest your early release paper “Laboratory-Confirmed COVID-19 Among Adults
Hospitalized with COVID-19-Like lliness with Infection-induced or mRNA Vaccine-Induced SARS-CoV-2
Immunity — Nine States, January-September 2021.” (accessed from here).
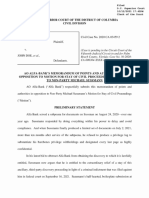
‘The graphic on the website summarizes the conclusi
previous infection were 5x more likely to have a pi
Here's the graphic:
of the paper as: “Unvaccinated people with
/e covid-19 test compared to vaccinated people.”
A study of hospitalized patients with symptoms
similar to COVID-19* found...
Unvaccinated people with a previous infection were
° *
a ™ 5x *, #
more likely to have a positive COVID-19 test
Get vaccinated
as soon as possible
bitLIy/MMWR704401 MMWR
‘This statement implies that the data in the paper applies to the population at large. But the data in the
paper does not include the population at large, rather it includes only people who were hospitalized
With covid-19 like illnesses,
‘My reading of the paper suggests that strongest conclusion the data supports is: “Among patients who
were hospitalized with covid-like symptoms, unvaccinated patients with previous infection were Sx
more likely to test positive for covid than vaccinated patients.” This s still an interesting finding, but itis
not as broad as the graphic implies.
‘My other question about the paper concerned Table 1, Since the paper is about patients who tested
positive for covid, | thought the data in Table 1 would have been more appropriately limited to patients
who tested positive, rather than describing the entire population of patients. The way that Table 1 is,
currentiy presented, there is no way to see the disaggregated data for patients who tested positive.
Thank you for considering these comments, and thank you for your important work in this area
Best regards,
Steve McConnell
Chief Executive Officer
Construx Software
c: 206-714-8467
8: 10900 NE 8th St. Ste. 1300, Bellevue, WA 98004
w; construx.com e: stevemec@construx.com
Medu, Lanre SHA
Tue, 2 Nov 2021 20:18:09 +0000
Bozio, Catherine H. (CDC/DDID/NCIRD/ID)
Follow-up question on your paper
‘Thank you, Dr. Bozio, for your work on the paper titled “Laboratory-Confirmed COVID-19 Among Adults
Hospitalized with COVID-19-Like Iliness with infection-induced or mRNA Vaccine-Induced SARS-CoV-2
Immunity — Nine States, January-September 2021”
I wanted to find out if you had data about the outcomes in these two groups, ie. clinical course after the
I visit, which was the basis of the analysis. Additionally, do you have an idea of the infection rates
in the non-hospitalized cases, or do you expect this finding to be similar in cases that were not
sufficiently ill to seek hospital care?
Thanks again, and | look forward to your response.
Dr. ‘Lanre Medu,
Medical Health Officer,
Population and Public Health Services,
Saskatchewan Health Authority,
2110 Hamilton Street, Regina, SK S4P2E3,
Tel-306 766 7771; Fax-306 766 7607
Bozio, Catherine H. (CDC/DDID/NCIRD/ID)
Sat, 30 Oct 2021 11:33:52 +0000
Choban, Ana (CDC/DDID/NCIRD/ID)
Fwd: covid-19 natural immunity vs. vaccine report
Best,
Catherine
From: Charles&Ruth Binford
Sent: Saturday, October 30, 2021 12:48:31 AM
To: Bozio, Catherine H. (CDC/DDID/NCIRD/ID)
Subject: covid-19 natural immunity vs. vaccine report
This is regarding the paper, "Laboratory-Confirmed COVID-19 Among Adults Hospitalized with
COVID-19-Like Hiness with Infection-Induced or mRNA Vaccine-Induced SARS-CoV-2
Immunity — Nine States, JanuarySeptember 2021, Early Release / October 29, 2021/70".
I've see the study you mentioned from Tsrael that indicated natural immunity is as good or better
then immunity from vaccination, Yet your paper indicates the opposite. I'm trying to understand
why.
1 can see from the article and tables that the ratio of those testing positive for covid-19 was lower
for the vaccinated group. But what I don't understand is why the raw numbers of those in the
hospital with covid-like symptoms was so much higher for the vaccinated (over 6000 vaccinated
vs. roughly 1000 unvaccinated). ‘The paper didn't address that issue. Does the estimated
number of vaccinated people to unvaccinated-but-previously-had-covid ratio account for that
difference in the raw numbers?
‘Thanks,
Charles Binford
Hill, Andrew (CDC/ODID/NCHHSTP/DTE)
Tue, 2 Nov 2021 16:03:01 +0000
Reynolds, Sue B. (CDC/DDID/NCIRD/ID)
FW: Ask a statistician
\VaccinationvsNaturallmmunityaStates_ MMWR_290ct2021.pdf
Hi, Sue
{see you were a co-author. | haven't read the article but any quick responses to the questions below?
Hope all is well. Any word on the DHOP position?
Andrew
From: Gurbaxani, Brian M. (COC/DDPHSS/0S/OT!)
Sent: Tuesday, 2 November, 2021 11:47
To: Hill, Andrew (CDC/DDID/NCHHSTP/DTE)
Ce: Glasser, John (CDC/DDID/NCIRD/DVD)
Subject: Fw: Ask a statistician
See my stats question below, and Betsy's tentative response. Has become even more pressing
due to that this is one of the most news covered MMWR's (attached) in a while...
Would appreciate some feedback. OT
it OHS)
Brian
From: Gunnels, Betsy (CDC/DDID/NCHHSTP/DHP)
Sent: Friday, October 29, 2021 2:27 PM
: Gurbaxani, Brian M. (CDC/ODPHSS/0S/0TI)
Sent: Friday, October 29, 2021 2:04 PM
To: Gunnels, Betsy (CDC/DDID/NCHHSTP/OHP)
Subject: Ask a statistician
HI Betsy!
Itwas great to talk to you the other day! Please keep me in mind as a resource for modeling,
engineering, or anything else | can be helpful with.
Anyway, | would like to ask you a hopefully quick q about stats. Attached and fascinating
MMWR just came out today, and honestly (my immunologist hat is on) | am surprised at the
magnitude of the results, so | looked into them. The aOR for reinfection is pretty big ~5.5, even
though the crude OR ~1.8, I'm not used to adjustments making that big of a difference. So!
looked at it and, well, the age profiles are quite different between groups, which could have a
big impact -- many more elderly in the vaccinated group. The aOR for the 65+ group is
19.6! But the crude OR for that group is also ~1.7, so the adjustments must be making an
impact somewhere else. | have no problem with the vaccine being better than natural
immunity but the odds ratios look really big. | suppose I should compare them to other
diseases where similar comparisons are possible.
Sorry, maybe these are amateur questions but perhaps you could help me to understand.
Thanks in advance! -- Brian
Centers for Disease Control and Prevention
Morbidity and Mortality Weekly Report
Early Release / Vol. 70
October 29, 2021
Laboratory-Confirmed COVID-19 Among Adults Hospitalized with
COVID-19-Like Illness with Infection-Induced or mRNA Vaccine-Induced
SARS-CoV-2 Immunity — Nine States, January-September 2021
Catherine 1. Bozi, PAD; Shaun J. Grannis, MD? Alison L. Naleway, PhD; Toan C. Ong, PRDS: Kristen A. Butterfield, MPH:
Malini B DeSilva, MD?; Karthik Natarsjan, PADSS. Duck-Hye Vang, PADS; Suchita Rao, MBBS Nicola ® Klein, MD, PhD,
Stephanie A. Ising MHS Brian E. Dion, PAD?!; Kristin Datcomb, MD, PhD!
Charlene McEvoy, MD; Juga Han; Sarah E, Rese, PHD% Ned Levis, MPH; Willan E. Fae, Pl
5, Kharbands, MDM: Pack K. Mitchell, ScD® Kristin Goddard, MPH:
Kempapua Murthy MBBS: Jil Ferinands, PRD!s Anupa
hia Lizo MPH(, Sue Reynolds, PAD:
st, Nancy Grisel, MPP;
PeeerJ-Embi, MD®™; Julie Arndorer, MPH!2; Chandni Raiyani, MPH": Palak Patel, MBRS!: Elizabeth A. Rowiey, DrPH®, Bruce Fireman, MA:
\Nimish R. Vali, DiPH, MBBS2; Eric P Griggs, MPH: Matthew F. Ley, PRD® Ousseny Zerbo, PhD; Rachael M. Porer, MPH:
Rebeeca J Bitch, MPH; Lenee Blawon, MPH! Sarah W. Ball, SeD® Andrea Steffens, MPH; Nazalie Olson, MPH! Jeremiah Willams, MPH
Monica Dickerson,
PH; Meredith MeMorrowe, MD; Stephanie |. Schrag, DPhil Jennifer. Versni, MD!> Alicis M. Ey, MD!
Eduardo Aziz Baumgartner, MD!; Michelle Baron, MD?; Manjusha Caplan, MBBS!2; Mark G. Thompson, PhD; Edward Stenehjem, MD!2
Previous infection with SARS-CoV-2 (the virus that causes
COVID-19) or COVID-19 vaccination can provide immu-
nity and protection from subsequent SARS-CoV-2 infection,
and illness. CDC used data from the VISION Network” to
examine hospitalizations in adults with COVID-19-like illness,
and compared the odds of receiving a positive SARS-CoV-2.
test result, and thus having laboratory-confirmed COVID-19,,
between unvaccinated patients with a previous SARS-CoV-2,
infection occurring 90-179 days before COVID-19-like illness,
hospitalization, and patients who were fully vaccinaved with an
mRNA COVID-19 vaccine 90-179 days before hospitaliza-
tion with no previous documented SARS-CoV-2 infection.
Hospitalized adults aged 218 years with COVID-19-like
illness were included if they had received testing atleast ewice:
once associated with a COVID-19-like illness hospitalization,
during January—September 2021 and at least once earlier (since
February 1, 2020, and 214 days before that hospitalization).
Among COVID-19-like illness hospitalizations in persons
‘whose previous infection or vaccination occurred 90-179 days:
carer, the odds of laboratory-confirmed COVID-19 (adjusted,
for sociodemographic and health characteris
unvaccinated, previously infected adults were
“Funded by CDG. the VISION Neework includes Columbia Universe ving
“Medial Center (New York), HeathParinets (Minnesota and Wisconsin,
Inuermountin Healthcare (Ua), Kaiser Permanente Northern California
(California), Kaiser Permanente Noschwest (Oregon and Washington),
Regent Inia ladiana), and University of Colorado (Colorado)
m4 aire
the odds among fully vaccinated recipients of an mRNA.
COVID-19 vaccine with no previous documented infection
(adjusted odds ratio [4OR] = 5.495 95% confidence interval
[Cl] = 2.75-10.99). These findings suggest that among hos-
pitalized adults with COVID-19-like illness whose previous
infection or vaccination occurred 90-179 days earlier, vaccine-
induced immunity was more protective than infectioninduced
immunity against laboratory-confirmed COVID-19. All
cligible persons should be vaccinated against COVID-19 as
soon as possible, including unvaccinated persons previously
infected with SARS-CoV-2,
“To compare the early protection against COVID-19 con-
ferred by SARS-CoV-2 infection and by receipt of mRNA.
COVID-19 vaccines (i.e. 90-179 days after infection or
vaccination), the VISION Network collected data from
187 hospitals across nine states during January~September
2021 (J). Bligible hospitalizations were defined as those
among adults aged 218 years who had received SARS-CoV-2
molecular testing (from 14 days before to 72 hours after admis-
sion) and had a COVID-19-like illness discharge diagnosis!
‘ Mdical evens with discharge code consistent with COVID-19-ike ils
vere induded, COVID-19+like inet diagnoses incaded acute respiratory
hes (eq, COVID-19,respestony ila, or pneumonia related signs oF
sympeome (cough eer, dyspnes, vomiting, or arth) using diagnosis codes
from he International Claaeton of Dies. Noh Revision and Iteration
(Clacton of Dis, Tenth Revi,
USS. Department of Health and Human Services
Centers for Disease Control and Prevention
Early Release
during January-September 2021. Eligible patients had also
been tested at least once since February 1, 2020. To limit the
analysis to patients with access to SARS-CoV-2 testing before
hospitalization, patients who did not receive SARS-CoV-2
testing 214 days before hospitalization were excluded.
‘Two exposure groups were defined based on COVID-19
vaccination status and previous SARS-CoV-2 infection.
‘Vaccination status was documented in electronic health
records and immunization registries. Previous infection was,
ascertained based on SARS-CoV-2 testing from rapid antigen,
tests or molecular assays (e.g, real-time reverse cranscription—
polymerase chain reaction) performed before mRNA vaccina-
tion and 214 days before admission; testing performed after
February 2020 was primarily within network partners’ medical
facilities. Adults were considered unvaccinated with a previous
SARS-CoV-2 infection if ne COVID-19 vaccine doses were
received and if the most recent positive SARS-CoV-2 test
result occurred 290 days before hospitalization. Adults were
considered fully vaccinated with an mRNA COVID-19 vaccine
with no previous documented infection if the second dose of
Pizer-BioNTech (BNT162b2) or Moderna (mRNA-1273)
mRNA vaccine was received 214 days before the index test
ddateS and if they had been tested since February 1, 2020,
and had no positive test results 214 days before hospitaliza-
tion. Patients were excluded if they had received 1 mRNA
vaccine dose only, received the second dose <14 days before
index test date, or received the Janssen Johnson & Johnson,
[Ad26.COV2}) vaccine (because of sparse data). To reduce
the chance thac the hospitalization was related co an ongoing
SARS-CoV-2 infection, patients were also excluded from the
previous infection group if their most recent previous positive
test result occurred 14-89 days before hospitalization.
‘The outcome of laboratory-confirmed
defined as COVID-19-like illness and a positive SARS-CoV-2.
result from molecular testing. Among patients hospitalized with,
COVID-19-like illness whose previous infection or comple
tion of vaccination occurred 90-179 days earlier, the odds of
Laboracory-confirmed COVID-19 were compared between pre
viously infected persons and fully vaccinated mRNA COVID-19,
vaccine recipients. ORs and 95% Cls were calculated using
multivariable logistic regression, adjusted for age, geographic
region, calendar time (days from January 1 to hospitalization),
and local virus circulation, and weighted based on propensity
to be in the vaccinated category (1,2). Established methods
were used to calculate weights to account for differences in
Tinton est date was deine athe date: of respiratory specimen collection
‘seociated with the most recent positive or negative SARS-CoV? fx elt
tefore the hosptalieation or the beoptalization date i tating only cocured
after admission,
‘raptor cde gfcoronavitws2019-ncoviphpinvese-criteria hem]
2 MMWR / October 29,2021 / Vo.70
sociodemographic and health characteristics berween groups
(9). Separate weights were calculated for each model, aORs were
stratified by mRNA vaccine product and age group.
Three secondary analyses wete also conducted. First, the
impact of whether and how the time interval since previous infec
tion or fll vaccination was adjusted was examined, Specifically,
any time since either previous infection or completion of vac-
ination was considered. Then, previously infected patients were
limited to those with more recent infections (i.e. 90-225 days,
before hospitalization [the lowest two tertiles of number of days,
since infection), and fully vaceinated patients were limited to
those with the longest interval since completion of vaccination
(ce. receipt of second mRNA vaccine dose 45-213 days before
hospitalization [the highest two tertiles of number of days since
vaccination). Thea, number of days sinee previous infection
‘or completion of vaccination, rather than calendar time, was
adjusted in the model. For the next secondary analysis, ORs for
hospitalizations thac occurred before and during SARS-CoV-2
B.1.617.2 (Delta) variant predominance (June-September
2021) were compared, beginning on the date the Delta vari-
ant accounted for >50% of sequenced isolates in each medical
facilty’s sate (2). Finally, effect modification was assessed by
mRNA vaccine product or by age group: p-values <0.2 were
considered indicative of a statistically significant difference in
aOR by produce or age, similar to previous modeling studies of
effect modification (4). All analyses were conducted using SAS
(version 9.45 SAS Institute) and R (version 4.0.2; R Foundation).
“This activity was reviewed by CDC and was conducted consis-
tent with applicable federal law and CDC policy.**
During January 1-September 2, 2021, a total of 201,269
hospitalizations for COVID-19-fike illness were identified:
139,655 (69.4%) patients were hospitalized after COVID-19
vaccines were generally available to persons in their age
‘group within their geographic region, Molecular testing for
SARS-CoV-2 was performed for 94,264 (67.5%) patients
with COVID-19-like illness hospitalizations. Among these
patients, 7,348 (7.8%) had at least one other SARS-CoV-2
test result 214 days before hospitalization and met eriteria for
cither of the two exposure categories: 1,020 hospitalizations
‘were among previously infected and unvaccinated persons, and
6,328 were among fully vaccinated and previously uninfected,
patients (Table 1)
Laboratory-confirmed SARS-CoV-2 infection was identi-
fied among 324 (5.19) of 6,328 fully vaccinated persons and
among 89 of 1,020 (8.7%) unvaccinated, previously infected
persons. A higher proportion of previously infected than vac~
cinated patients were aged 18-49 years (31% versus 9%), Black,
(10% versus 796), and Hispanic (19% versus 1296).
S35 GER pare 46:21 GER pare 6.
Early Release
‘TABLE 1. Characteristics of COVID-19-like illness hospitalizations* among unvaccinated adults with a SARS-CoV-2 infection occurring 90-179,
days before the index test date’ and among adults who were fully vaccinated? 90-179 days before the index test date" without a previous
documented SARS:CoV-2 infection — nine states,*
nuary-September 2021
‘Unvaccinated with previous
SARS-CoV? infection
Characteristic
‘No. (coun 8)
Fully vaccinated without Standardized mean or
previous documented infection proportion cfference™>
‘Al hospitalizations with COVID-T9-ke ness
SARS-CoV. tast result associated with COVID-19-like illness hospitalization
Postive
Negative
Sex
Male
Female
‘Age group. yes
18
50-64
65-74
75.84
285
Race, respective of ethnilty
Woite
Black
Other!*
Unknown
Ethnicity imespective of race
Hispanic
Non-Hispanic
Unknown
Month ofindextest date!
January
Febrasty
ares
Apri
May
ine
aly
August
September
71020(100) 328 100) NA
3919) x45) on
331191) 6004.85)
405 40) 2905 46) on
15 60) 342364)
31360 50009) ova
243 (20) 955 (4)
207 20) 1757 08)
wry 201862)
3018) 112808),
4.35669) oz
45207)
686 (11)
834(03)
89119) 756012) 020
695 68) 445870)
136113) anna)
no om) 210
a) om)
macnn ray
245 28) 600)
29409) 235 (8)
‘se 18 130021)
59110) 2731083)
3113) 2.0932)
110 70)
See abe footnotes on the nO PAGE
Among COVID-19-like illness hospitalizations in persons
whose previous infection or vaccination occurred 90-179 days
calie, the odds of laboratory-confirmed COVID-19 were higher
among previously infected, unvaccinated patients than among
fully vaccinated patients (aOR = 5.49; 95% CI = 2.75-10.99)
(Table 2). In secondary analyses, the aORs that examined the
impact of whether and how time since infection or yaccina-
tion was adjusted and that stratified hospitalizations before
and during Delta variant predominance were all similar co the
primary aOR estimate. For product- and age group-specific
estimates, sparse data limited the precision of these aORs.
However, an assessment of effect modification indicated the
aOR of laboratory-confirmed COVID-19 was higher for previ-
ously infected patients compared with patients vaccinated with
‘Moderna (aOR = 7.30) than compared with patients vaccinated,
with Pfizer-BioN Tech (aOR = 5.11) during January-Seprember
(p=0.02). Similarly; the interaction term for exposure group by
age indicated that the aOR was higher for patients aged 265 years,
(2OR = 19.57) than for those aged 18-64 years (aOR = 2.57)
(interaction term, p = 0.05).
Discussion
In his mukistateanalyss of hospitalizations for COVID-19-lke
illness among adults aged 218 years during January-September
2021 whose previous infection or vaccination occurred 90-179 days
earlier, the adjusted odds of laboratory-confirmed COVID-19
"were higher among unvaccinated and previously infected patients,
than among those who were fully vaccinated with 2-doses of an
mRNA COVID-19 vaccine without previous documentation of
SARS-CoV-2 infection, Secondary analyses that did not adjust for
time since infection or vaccination or adjusted time since infection
or vaccination differently as well as before and during Delta
variant predominance produced similar results. These findings are
consistent with evidence that neutralizing antibody tersafter receipt
oF 2 doses of mRNA COVID-19 vaccine are high (5.6); however,
these findings differ from those of a retrospective records-based,
DMAKWR / October29,2021 / Vol. 70 3
Early Release
‘TABLE 1. (Continued) Characteristics of COVID-19-likellness hosptalizations* among unvaccinated adults with a SARS-CoV--2 infection occurring
90-179 days before the index test date’ and among adults who were fully vaccinated® 90-179 days before the index test date’ without 3
previous documented SARS-CoV-2 infection — nine states, January September 2021
Tio. (cokamn
‘Unvaccinatedwith previous Fully vaccinated without Standardized mean or
Characteristic SARS-CoV-Zinfection previous documented infection proportion diference”™
site
Columbia University 39 23818) 073
HealthParners 20 3401)
Intermountain Healthcare nan 45407)
Kaiser Permanente Norther California 254 25) 3614057)
Kaiser Permanente Northwest, 303) 250 (8)
Regenstie institute 300138) 1145.08)
University of Colorado 154105) 5336)
Time since either previous SARS-CoV. infection o fullmRNA vaccination until COVID-19-Lke illness index test date days
90-119 367 36) 3325 (53) oa
120-149 35335) 210163)
150-179 30029) ‘02104)
CCOVID-19 vaccination status
Unvaccnated 11020 100) 0) NA
Pier SiiVTech(BNT16262) oO 3736158)
Moderna (mniNA-1273) om 2592141)
‘Abbreviation: NA =not applicable,
* Medical events with decharge cod consstent with COVID-10-ke ines were included, COMID-19-Ike ines diagnoses included acute espatory ines (2,
COVID-19,resprtory alr oF pneumonia or related signs or symptoms (cough fever dyspnea, vomiting ore) using dlegnosiscodesfrom the ntemetione)
Clastieation f Diseases nth Revision and Internationa Cleeafetion of Diseases, Tenth Revision Cimisan ordered molecular assays (e. realtime reverse
‘wansciption-polymerase chain reaction for SARS-CoV'2 occurring =14 days before to <72 hous after hospital admission were included
"Inde test date wae defined a the date of respiratory specimen colectionasaciated withthe most racent poave or negative SARS-CoVe? test result before the
hospitalization or the hospitalization date if testing only occured after he admission.
Ss Ful vaccination was defined a receipt ofthe second dose a Pier ioNTach or Madera mRNA vaccine »14 days before the index test date
‘Partners contributing hospitalizations were in Calfornia, Colorado, Indiana, Minnesota and Wisconsin, Oregon and Washington, Utah and NewYork
‘In comparing characteristics between unvaccinated aduls with 2 previous infection and full vaccinated adults without a previous documented infection, @
Standardized mean or proportion diference 0.2 was considered noteworthy, After balancing characteristics thot fered between the two compotion groups,
the standardized mean or proportion differences were <0.6.
“Other race includes Asian Hawallan or Othe Paci slander, American Indian or Alaskan Native, Other not sted and multiple races.
cohort study in Isae,"* which did noc find higher protection for
vaccinated adults compared with those with previous infection
during period of Delta variant circulation, This variation s possibly
relared to differences in the outcome of interest and restrictions on
the timing of vaccination. The Israeli cohort study assessed any
positive SARS-CoV-2 test result, whereas this study examined
Inboratory-confirmed COVID-19 among hospitalized patients
‘The Israeli cohort study also only examined vaccinations that had
cccurted 6 months earlier, so the benefit of more recent vaccination,
‘was not examined. This report focused on the early protection
fiom infection-induced and vaccine-induced immunity, hough ic
ispossble that estimates could be affected by time, Understanding
Infection-induced and vaccine-induced immunity over time is
important, particularly for fururescudies to consider.
In this study, the benefit of vaccination compared with infec-
tion without vaccination appeared to be higher for recipients
of Moderna than Pfizer-BioN Tech vaccine, which is consistent
with a recent study that found higher vaccine effectiveness
against COVID-19 hospitalizations for Moderna vaccine recip
ients than for Pfizer-BioNTech vaccine recipients (7). In this,
TW inepalTowwanedoaicory/comtenc/10.1101/2021.08.24.2126241501
4 MMWR / October 29,2021 / Vo.70
study, the protective effec of vaccination also trended higher
for adults aged 265 years than for those aged 18-64 years
However, considering the limited data by both product type
and age, additional research is needed on the relative protec-
tion of vaccination versus infection without vaccination across
demographic groups and vaccine products, as well as vaccina-
tion in previously infected persons.
“The findings in this report are subject to at east seven limita-
tions, First, although this analysis was designed to compare two
groups with different sources of immunity, patients might have
been misclassified. IF SARS-CoV-2 testing occurred outside of
network partners’ medical facilities or if vaccinated persons
are les likely to seek testing, some positive SARS-CoV2 test
results mighthave been missed and thus some patients classified
as vaccinated and previously uninfected might also have been
infected. In addition, despite the high specificity of COVID-19.
‘vaccination status from these data sources, misclassification is
possible. Second, the aOR could not be further stratified by
time since infection or vaccination because of sparse data and.
limited ability to control for residual confounding that could,
be magnified within shorter intervals, The aOR that did not
adjust for time might also be subject to residual confounding,
Early Release
TABLE 2. Adjusted odds ratios* of laboratory-confirmed COVID-19 among hospitalizations in adults with COVID-19-tike illness comparing
tunvaccinated adults with a SARS-CoV-2 infection occurring 90-179 days before the index test date and adults who were fully vaccinated
90-179 days before the Index test date without a previous documented SARS-CoV-2 infection — nine states, January-September 2021
No. row of
SARS COV'2. Adjusted odés ratio
outcome Totalna,_postvetetresuts (95%
‘Aad faged 218 yor) any COVID-19 RNA voccine
Any mRNA vaccine
Faly vacated without previous documented infection 632832415) fet
Unvacinated wth a previous SARS-CoV? infection Yoo “8908 549 (275-1099)
Any mRNA vaccine no restiton of time since previous infection or completion of vaccination
Faly vacated without prevous documented infection we37 54200) fe
{range of ie since vacation ~ 0-713 days tore hospitalization
Unwacinoted wth a reviou SARS-CoV 2inecton 2005 130462) 275(190-398)
{range of me since prevosinfstion - 50-94 days before hosetalation)
‘ny mRNA vaccine examining the potential influence of ime since prevousinfcton or completion of vaccination
Fully vaccinated” without previous documented nection limited to those wih ongestpeiog 12231 458(3.7 ref
Sincevacination ange of tnesince vocation = 45-213 dys belorehosptalation
Unvacnated witha previous SARS-CoV2 infection imied to those with marerecent infections 1388107 7.71 396(249-635)
{range of ime since prevousinfection - 50-225 days before osptalaton)
‘Any mRNA vaccine adjusting fr time since previous infection or completion of vaccination n model
Fall vochated witout pes documented infection 6028 324651) fet
Unvacenated wth a previous SARS-COV"? infection Yoo 89087) 322(168-620)
8 time relative to SARS-CoV-28.1.6172 (Det) varant predominance
Before Dela predominance January-June 2021)
Fal vaccinated without previous documented infection as 808) te
Unvacnated wth a prewous SARS-CoV fection on 70184) an 28-1316
During Det predominance UuneSeptember 2021)"
Falyvaccsted’ witout pevous documented infection 5230655) fe
Unvaceated wth a previous SARS-CoV? infection 1 191100) 755 045-1652
By mRNA vacine product?
Piizer BioN Tech (BNT16262)
Fully vaccinated! without previous documented nection 373815658) fet
Unvacinated wth a previous SARS-Co¥? infection yoo “89087) 511 283-1029)
Moderna mRNA-1275)
Ful vacated without prevous documented infection 252109442) ff
Unvaccnated witha previous SARS-CoV? infection 100 85087) 7.30(640-1560)
By age group, yst
rest
Ful vaccinated? without previous documented infection 125 7150) fe
Unvecinated wth a previous SARS-CoV? infection 5649488) 27014-4165)
365
Fully vacated” without previous documented infection aos 253152) fe
Unvaccnated witha preous SARS-CoV? fection as 0186) 1957 (634-4591
‘Abbreviations: CI= confidence interval ref = referent group,
* Odds flios were adjusted forage, geographic region, calendar tine (days since January 1, 2027), and lca vts culation (percentage of SARS-CoV2 postive
results rom testing within the counties surrounding the fcity on the date ofthe hospitalization) and balanced using mverse weights on characteristics thet
Gere between the we groups (calculated separately or each odds ato mode! using faclity characteristics, sociodemographic characterises and underying
‘medical conditions. Cardiovascular dlgease was also adjusted n the main model and in the model for PizerBioNTech. Any Ikelyimmunesuppression was also
Included inthe model for Modema, Neuromuscular and rsptatory conitons were ako adjusted inthe model for adults aged 265 years Number of days since
previous infection or completion of vaccination instead of clend time, was adjusted in the model within the stated secondary analysis
{Full vaccination was defined as receipt of the second dose of Pfr SioNTech or Madera mfINA vaccine =14 days before the index test date
{3 Pwaluefrom assessment of effect modiiation by mRNA product was 402,
{1Pwaluefor interaction term for exposure group by age group was 005.
= SARS-CaV.2B 1617 2 (Delta variant predominance began on the date the Delt variant accounted for >50%of sequenced isolates in each meta fait’ state
ttpsfdoLorg/10.1888Smmvitmmn7037e2
particularly related co waning of both types of immunity. Third,
selection bias might be possible if vaccination status influences
likelihood of testing and if previous infection influences the
likelihood of vaccination, Previous work from the VISION net-
work did not identify systematic bias in testing by vaccination,
status, based on data through May 2021 (1), Fourth, residual
confounding might exist because the study did not measure
‘or adjust for behavioral differences berween the comparison
‘groups that could modify the risk of che outcome. Fifth, these
results might not be generalizable co nonhospitalized patients,
who have different access to medical care or different health
‘eare-secking behaviors, particularly outside of the nine states
DMAKWR / October29,2021 / Vol. 70 5
Early Release
covered, Sixth, the statistical model incorporated the use of a
weighted propensity score method which is subject to biases,
in estimates or standard errors if the propensity score model,
is misspecified. Numerous techniques were used to reduce
potential suboptimal specification of the model, including buc
not limited to including a large set of covariates for machine
learning estimation of propensity scores, including covariates in
both regression and propensity models, ensuring large sample
sizesand checking stability of weights, and conducting second-
ary analyses to assess robustness of results. Finally, the study
assessed COVID-19 mRNA vaccines onlys findings should
not be generalized to the Janssen vaccine.
In this U.S.-based epidemiologic analysis of patients hospi-
talized with COVID-19-like illness whose previous infection,
or vaccination occurred 90-179 days earlier, vaceine-induced
immunity was more protective than infection-induced immunity
against laboratory-confirmed COVID-19, inchiding during a
petiod of Delta variant predominance. All eligible persons should,
be vaccinated against COVID-19 as soon as possible, including
unvaccinated persons previously infected with SARS-CoV-2.
‘Acknowledgments
Jeffenon Jones, Claire Midgley, Ruth Link-Glks, Sharon Saydab,
Jerome Tos, Adi Gundlapall, Natalie Thornburg Aga Shefr, John
Kool, Erin Tromble, Meissa Caer, Cory Kokko, Stephanie Weaver,
Kushali Muthumalaippan, Bio-Ping Zhu, Roumiana Boneva, CDC.
‘Coneapondng author: Caterne H, Bono, 7@ede pu
TEDE COVID-I9 Response Team: Center for Biomedical Informatics
Regenatit Insitute Indianapolis, Indiana; diana University School of
“Maticns, Indianapolis, India, "Center for Eleth Reseach, Kater Petmanente
‘Nanhses, Portland, Oxgon Deparment of Medicine, Univesity of Colorado,
‘Anachate Medical Campus, Aurora, Colorado “West, Rockville, Marland:
"earners faite, Minneapolis Mins Depurtmenc of Brome
Iaformatics, Columbia Universi, New Yor, New Yorks °New York Prbyteian
Hospital, New Vrk ity, New York Kaiser ermanente Verne Stn Center,
Keser Permanente Northern Caloris, Oakland, California: Finks Schoo
‘of Public Health, Indiana University Indianapolis, Indiana; ?Divsion of
Infectious Dace and Clinical Epidemiology Iermoantin Healthcare, Salt
Lake iy Uh, Baylor Scot 8 White Health, Teas ASM University College
‘of Medicine. Temple. Teas; Childress Minasoa, Minneapolis, Minnesota
"Regen Ines, Indnspalis Indian
All authors have completed and submitted the International
Commixtee of Medical Journal Editors form for disclosure of
potential conflicts of interest. Stephanie A. Irving reports support
from Westat to Kaiser Permanente Northwest Center for Health
Research. Nicola P. Klein reports support from Pfizer to Kaiser
Permanente, Northern California for COVID-19 vaccine clinical
trials, and institutional support from Merck, GlaxoSmithKline, and
Sanofi Pasteur outside the current study. Charlene McEvoy reports,
support fiom AstraZeneca o HealthPartnes Institue for COVID-19
vaccine tras. Alison L. Naleway reports Pfizer Research funding to
‘summary
‘What i aleady known about this topic?
Previous infection with SARS-CoV-2 or COVID-19 vaccination
‘can provide immunity and protection against subsequent
‘SARS,CoV’2 infection and illness.
‘Whatis added by this report?
Among COVID-19-tke illness hospitalizations among adults
‘aged =18 years whose previous infection or vaccination.
‘occured 90-179 days earlier, the adjusted odds of laboratory-
‘confirmed COVID-19 among unvaccinated adults with previous
‘SARS-CoV'2 infection were 5.49-fld higher than the odds,
‘among fully vaccinated recipients ofan mRNA COVID-19
‘vaccine who had no previous documented infection (95%
‘confidence interval= 2.75-10.99).
What are the implications for public heath practice?
Alleligible persons should be vaccinated against COVID-19 as
‘soon 25 possible, including unvaccinated persons previously
infected with SARS-CoV-2,
Kaiser Permanente Northwes for unrelated study of meningococcal B
vaccine safety during pregnancy. Suchitra Rao reports grants from
GlaxoSmithKline and Biofire Diagnostics. No other potential
conflicts of interest were disclosed.
References
1. ThompsonMMG, Senchjam E, Grams eal Eevee of Covi 19 vaccines
in ambulatory and inpatient cae serting: N Engl J Med 2021:385:1355-71
PRID'34496194 pds on 10.1056) NEJMes21 10362
annis SJ, Rowley EA, Ong TC, etal: VISION Nerwork. Ines
‘estimates of COVID-19 vaccine effectiveness against COVID-19-
associated emergency department or urgent care clinical encounters and
hospitalizations among adults during SARS-CoV.2 B.L.617.2 (Del)
variant predomninance—-nine states, June-August 2021. MMWR Mor
Moreal Wly Rep 2021:70:1291-3. PMID:34529642 hurpst/doi
‘ong/10.15585 ramon 7037e2
3. Mansion R, Joe MM, Sun W, Hennesy S. On the estimation and use of
propensity scores in catecoattol and eac-cohore sie. Am J Epidemiol
2047 :166'382-9, PMID:17504780 haps. op, 1093/69
Maraall SW. Power for tests of iteration: effet of taxing the Type 1
‘error rate. Epidemiol Perspect Innov 2007%4r4, PMID:17578572 hep)
ddoj.ory/10-1186)1742-5573-4-4
5, Bdars VV, Hudson WH, Xie X, Ahmed Ry Suthar MS, Neutrlising
antibodies against SARS-CaV2 variants after infection and vaccination,
JAMA 20213325:1896-8, PMID:33739374 hepefd.org10 1001)
jama.2021.4388
6 dara WV, Pinsky BA, Suchar MS, etal, fection and vaesine induced
rewraliing-antibody responses to the SARS-CaV’2 B.1.617 variants
N Engl } Med 2021;385:664-6, PMID:34233096 heeps! do,
‘rg/10.1056/NEJMc2107799
7. Self WH, Tenforde MW, Rhoads J ca; IVY Neework. Comparative
celfeciveness of Moderna, Pizer BioN Tec, and Janssen Johnson 8
Johnson) vaccines in preventing COVID- 19 hospitalizations among adults
{without immunocompromining conditions-—United States, March~
‘August 2021. MMWR Morb Moctal Wkly Rep 2021,70:1337—43.
PMUD:34555004 hueps:/doiog/10.15385/mmwemun7038el
Readers who have difficulty accessing this PDF file may access the HTML file at hurps/#www.cdegov/mmv/volumes/70¢vwr/mm7044e1
hhum’s_cidemm7044el_v. Address all inquiries about the MMWR Series, including material to be considered for publication, to Editor,
‘MMUWR Series, Mailstop V25~
6 MMWR / October 29,2021 / Vo.70
CDG, 1600 Glifon Rd, N.E. Atlanta, GA 30329-4027 or co mmwrrq@edc.gov.
From: Dunworth, Soumya (CDC/DDPHSS/CSELS/OD)
Sent: Fri, 29 Oct 2022 14:51:41 +0000
To: Bozio, Catherine H. (CDC/DDID/NCIRD/ID)
Subject: FW: MMWR Embargoed eBooks for 10/29 Early Release
Attachments: MMWR ER - October 29, 2021 - Laboratory-Confirmed COVID-19 Among Adults
Hospitalized with COVID-1S-Like Illness with Infection-Induced or mRNA Vaccine-Induced SARS-CoV-2
Immunity — Nine States, January-September 2021.pdf
From: MMWR Communications (CDC)
Sent: Friday, October 29, 2021 10:51 AM
‘To: MMWR Communications (CDC) ; CDC MMWR ER Ebook
Subject: MMWR Embargoed eBooks for 10/29 Early Release
MMWR fac
Morbidity and Mortality Weekly Report
The MMWR is embargoed until 1 PM ET Friday, October 29, 2021
Please find the eBooks for today’s MMWR Early Release attached.
Laboratory-Confirmed COVID-19 Among Adults Hospitalized with COVID-19-Like Iliness
with Infection-Induced or mRNA Vaccine-Induced SARS-CoV-2 Immunity — Nine States,
January-September 2021
Link when live
https: //www.cdc.gov/mmwr/volumes/70/wr/mm7044e1.htm?s_cid=mm7044e1_w
A study of hospitalized patients with symptoms
similar to COVID-19* found...
Unvaccinated people with a previous infection were
*
*
* 5x *
more likely to have a positive COVID-19 test
compared to vaccinated peoplet
“ome enaeene mame cen enn
Get vaccinated
as soon as possible
bietnmnwnoeser MWR
The Advisory Committee on Immunization Practices’ Interim Recommendations for
Additional Primary and Booster Doses of COVID-19 Vaccines — United States, 2021
Link when live:
https: //www.cde.gov/mmwr/ volumes /70/wr/mm7044e2.htm?s_cid=mm7044e2_w
Best,
lan
fan Branam, MA
Health Communication Specialist
Center for Surveillance, Epidemiology, and Laboratory Services
Centers for Disease Control and Prevention
0: 404-639-9316 | M: 404-275-3133 | E: ibranam@cdc.gov
Centers for Disease Control and Prevention
Morbidity and Mortality Weekly Report
Early Release / Vol. 70
October 29, 2021
Laboratory-Confirmed COVID-19 Among Adults Hospitalized with
COVID-19-Like Illness with Infection-Induced or mRNA Vaccine-Induced
SARS-CoV-2 Immunity — Nine States, January-September 2021
Catherine 1. Bozi, PAD; Shaun J. Grannis, MD? Alison L. Naleway, PhD; Toan C. Ong, PRDS: Kristen A. Butterfield, MPH:
Malini B DeSilva, MD?; Karthik Natarsjan, PADSS. Duck-Hye Vang, PADS; Suchita Rao, MBBS Nicola ® Klein, MD, PhD,
Stephanie A. Ising MHS Brian E. Dion, PAD?!; Kristin Datcomb, MD, PhD!
Charlene McEvoy, MD; Juga Han; Sarah E, Rese, PHD% Ned Levis, MPH; Willan E. Fae, Pl
5, Kharbands, MDM: Pack K. Mitchell, ScD® Kristin Goddard, MPH:
Kempapua Murthy MBBS: Jil Ferinands, PRD!s Anupa
hia Lizo MPH(, Sue Reynolds, PAD:
st, Nancy Grisel, MPP;
PeeerJ-Embi, MD®™; Julie Arndorer, MPH!2; Chandni Raiyani, MPH": Palak Patel, MBRS!: Elizabeth A. Rowiey, DrPH®, Bruce Fireman, MA:
\Nimish R. Vali, DiPH, MBBS2; Eric P Griggs, MPH: Matthew F. Ley, PRD® Ousseny Zerbo, PhD; Rachael M. Porer, MPH:
Rebeeca J Bitch, MPH; Lenee Blawon, MPH! Sarah W. Ball, SeD® Andrea Steffens, MPH; Nazalie Olson, MPH! Jeremiah Willams, MPH
Monica Dickerson,
PH; Meredith MeMorrowe, MD; Stephanie |. Schrag, DPhil Jennifer. Versni, MD!> Alicis M. Ey, MD!
Eduardo Aziz Baumgartner, MD!; Michelle Baron, MD?; Manjusha Caplan, MBBS!2; Mark G. Thompson, PhD; Edward Stenehjem, MD!2
Previous infection with SARS-CoV-2 (the virus that causes
COVID-19) or COVID-19 vaccination can provide immu-
nity and protection from subsequent SARS-CoV-2 infection,
and illness. CDC used data from the VISION Network” to
examine hospitalizations in adults with COVID-19-like illness,
and compared the odds of receiving a positive SARS-CoV-2.
test result, and thus having laboratory-confirmed COVID-19,,
between unvaccinated patients with a previous SARS-CoV-2,
infection occurring 90-179 days before COVID-19-like illness,
hospitalization, and patients who were fully vaccinaved with an
mRNA COVID-19 vaccine 90-179 days before hospitaliza-
tion with no previous documented SARS-CoV-2 infection.
Hospitalized adults aged 218 years with COVID-19-like
illness were included if they had received testing atleast ewice:
once associated with a COVID-19-like illness hospitalization,
during January—September 2021 and at least once earlier (since
February 1, 2020, and 214 days before that hospitalization).
Among COVID-19-like illness hospitalizations in persons
‘whose previous infection or vaccination occurred 90-179 days:
carer, the odds of laboratory-confirmed COVID-19 (adjusted,
for sociodemographic and health characteris
unvaccinated, previously infected adults were
“Funded by CDG. the VISION Neework includes Columbia Universe ving
“Medial Center (New York), HeathParinets (Minnesota and Wisconsin,
Inuermountin Healthcare (Ua), Kaiser Permanente Northern California
(California), Kaiser Permanente Noschwest (Oregon and Washington),
Regent Inia ladiana), and University of Colorado (Colorado)
m4 aire
the odds among fully vaccinated recipients of an mRNA.
COVID-19 vaccine with no previous documented infection
(adjusted odds ratio [4OR] = 5.495 95% confidence interval
[Cl] = 2.75-10.99). These findings suggest that among hos-
pitalized adults with COVID-19-like illness whose previous
infection or vaccination occurred 90-179 days earlier, vaccine-
induced immunity was more protective than infectioninduced
immunity against laboratory-confirmed COVID-19. All
cligible persons should be vaccinated against COVID-19 as
soon as possible, including unvaccinated persons previously
infected with SARS-CoV-2,
“To compare the early protection against COVID-19 con-
ferred by SARS-CoV-2 infection and by receipt of mRNA.
COVID-19 vaccines (i.e. 90-179 days after infection or
vaccination), the VISION Network collected data from
187 hospitals across nine states during January~September
2021 (J). Bligible hospitalizations were defined as those
among adults aged 218 years who had received SARS-CoV-2
molecular testing (from 14 days before to 72 hours after admis-
sion) and had a COVID-19-like illness discharge diagnosis!
‘ Mdical evens with discharge code consistent with COVID-19-ike ils
vere induded, COVID-19+like inet diagnoses incaded acute respiratory
hes (eq, COVID-19,respestony ila, or pneumonia related signs oF
sympeome (cough eer, dyspnes, vomiting, or arth) using diagnosis codes
from he International Claaeton of Dies. Noh Revision and Iteration
(Clacton of Dis, Tenth Revi,
USS. Department of Health and Human Services
Centers for Disease Control and Prevention
Early Release
during January-September 2021. Eligible patients had also
been tested at least once since February 1, 2020. To limit the
analysis to patients with access to SARS-CoV-2 testing before
hospitalization, patients who did not receive SARS-CoV-2
testing 214 days before hospitalization were excluded.
‘Two exposure groups were defined based on COVID-19
vaccination status and previous SARS-CoV-2 infection.
‘Vaccination status was documented in electronic health
records and immunization registries. Previous infection was,
ascertained based on SARS-CoV-2 testing from rapid antigen,
tests or molecular assays (e.g, real-time reverse cranscription—
polymerase chain reaction) performed before mRNA vaccina-
tion and 214 days before admission; testing performed after
February 2020 was primarily within network partners’ medical
facilities. Adults were considered unvaccinated with a previous
SARS-CoV-2 infection if ne COVID-19 vaccine doses were
received and if the most recent positive SARS-CoV-2 test
result occurred 290 days before hospitalization. Adults were
considered fully vaccinated with an mRNA COVID-19 vaccine
with no previous documented infection if the second dose of
Pizer-BioNTech (BNT162b2) or Moderna (mRNA-1273)
mRNA vaccine was received 214 days before the index test
ddateS and if they had been tested since February 1, 2020,
and had no positive test results 214 days before hospitaliza-
tion. Patients were excluded if they had received 1 mRNA
vaccine dose only, received the second dose <14 days before
index test date, or received the Janssen Johnson & Johnson,
[Ad26.COV2}) vaccine (because of sparse data). To reduce
the chance thac the hospitalization was related co an ongoing
SARS-CoV-2 infection, patients were also excluded from the
previous infection group if their most recent previous positive
test result occurred 14-89 days before hospitalization.
‘The outcome of laboratory-confirmed
defined as COVID-19-like illness and a positive SARS-CoV-2.
result from molecular testing. Among patients hospitalized with,
COVID-19-like illness whose previous infection or comple
tion of vaccination occurred 90-179 days earlier, the odds of
Laboracory-confirmed COVID-19 were compared between pre
viously infected persons and fully vaccinated mRNA COVID-19,
vaccine recipients. ORs and 95% Cls were calculated using
multivariable logistic regression, adjusted for age, geographic
region, calendar time (days from January 1 to hospitalization),
and local virus circulation, and weighted based on propensity
to be in the vaccinated category (1,2). Established methods
were used to calculate weights to account for differences in
Tinton est date was deine athe date: of respiratory specimen collection
‘seociated with the most recent positive or negative SARS-CoV? fx elt
tefore the hosptalieation or the beoptalization date i tating only cocured
after admission,
‘raptor cde gfcoronavitws2019-ncoviphpinvese-criteria hem]
2 MMWR / October 29,2021 / Vo.70
sociodemographic and health characteristics berween groups
(9). Separate weights were calculated for each model, aORs were
stratified by mRNA vaccine product and age group.
Three secondary analyses wete also conducted. First, the
impact of whether and how the time interval since previous infec
tion or fll vaccination was adjusted was examined, Specifically,
any time since either previous infection or completion of vac-
ination was considered. Then, previously infected patients were
limited to those with more recent infections (i.e. 90-225 days,
before hospitalization [the lowest two tertiles of number of days,
since infection), and fully vaceinated patients were limited to
those with the longest interval since completion of vaccination
(ce. receipt of second mRNA vaccine dose 45-213 days before
hospitalization [the highest two tertiles of number of days since
vaccination). Thea, number of days sinee previous infection
‘or completion of vaccination, rather than calendar time, was
adjusted in the model. For the next secondary analysis, ORs for
hospitalizations thac occurred before and during SARS-CoV-2
B.1.617.2 (Delta) variant predominance (June-September
2021) were compared, beginning on the date the Delta vari-
ant accounted for >50% of sequenced isolates in each medical
facilty’s sate (2). Finally, effect modification was assessed by
mRNA vaccine product or by age group: p-values <0.2 were
considered indicative of a statistically significant difference in
aOR by produce or age, similar to previous modeling studies of
effect modification (4). All analyses were conducted using SAS
(version 9.45 SAS Institute) and R (version 4.0.2; R Foundation).
“This activity was reviewed by CDC and was conducted consis-
tent with applicable federal law and CDC policy.**
During January 1-September 2, 2021, a total of 201,269
hospitalizations for COVID-19-fike illness were identified:
139,655 (69.4%) patients were hospitalized after COVID-19
vaccines were generally available to persons in their age
‘group within their geographic region, Molecular testing for
SARS-CoV-2 was performed for 94,264 (67.5%) patients
with COVID-19-like illness hospitalizations. Among these
patients, 7,348 (7.8%) had at least one other SARS-CoV-2
test result 214 days before hospitalization and met eriteria for
cither of the two exposure categories: 1,020 hospitalizations
‘were among previously infected and unvaccinated persons, and
6,328 were among fully vaccinated and previously uninfected,
patients (Table 1)
Laboratory-confirmed SARS-CoV-2 infection was identi-
fied among 324 (5.19) of 6,328 fully vaccinated persons and
among 89 of 1,020 (8.7%) unvaccinated, previously infected
persons. A higher proportion of previously infected than vac~
cinated patients were aged 18-49 years (31% versus 9%), Black,
(10% versus 796), and Hispanic (19% versus 1296).
S35 GER pare 46:21 GER pare 6.
Early Release
‘TABLE 1. Characteristics of COVID-19-like illness hospitalizations* among unvaccinated adults with a SARS-CoV-2 infection occurring 90-179,
days before the index test date’ and among adults who were fully vaccinated? 90-179 days before the index test date" without a previous
documented SARS:CoV-2 infection — nine states,*
nuary-September 2021
‘Unvaccinated with previous
SARS-CoV? infection
Characteristic
‘No. (coun 8)
Fully vaccinated without Standardized mean or
previous documented infection proportion cfference™>
‘Al hospitalizations with COVID-T9-ke ness
SARS-CoV. tast result associated with COVID-19-like illness hospitalization
Postive
Negative
Sex
Male
Female
‘Age group. yes
18
50-64
65-74
75.84
285
Race, respective of ethnilty
Woite
Black
Other!*
Unknown
Ethnicity imespective of race
Hispanic
Non-Hispanic
Unknown
Month ofindextest date!
January
Febrasty
ares
Apri
May
ine
aly
August
September
71020(100) 328 100) NA
3919) x45) on
331191) 6004.85)
405 40) 2905 46) on
15 60) 342364)
31360 50009) ova
243 (20) 955 (4)
207 20) 1757 08)
wry 201862)
3018) 112808),
4.35669) oz
45207)
686 (11)
834(03)
89119) 756012) 020
695 68) 445870)
136113) anna)
no om) 210
a) om)
macnn ray
245 28) 600)
29409) 235 (8)
‘se 18 130021)
59110) 2731083)
3113) 2.0932)
110 70)
See abe footnotes on the nO PAGE
Among COVID-19-like illness hospitalizations in persons
whose previous infection or vaccination occurred 90-179 days
calie, the odds of laboratory-confirmed COVID-19 were higher
among previously infected, unvaccinated patients than among
fully vaccinated patients (aOR = 5.49; 95% CI = 2.75-10.99)
(Table 2). In secondary analyses, the aORs that examined the
impact of whether and how time since infection or yaccina-
tion was adjusted and that stratified hospitalizations before
and during Delta variant predominance were all similar co the
primary aOR estimate. For product- and age group-specific
estimates, sparse data limited the precision of these aORs.
However, an assessment of effect modification indicated the
aOR of laboratory-confirmed COVID-19 was higher for previ-
ously infected patients compared with patients vaccinated with
‘Moderna (aOR = 7.30) than compared with patients vaccinated,
with Pfizer-BioN Tech (aOR = 5.11) during January-Seprember
(p=0.02). Similarly; the interaction term for exposure group by
age indicated that the aOR was higher for patients aged 265 years,
(2OR = 19.57) than for those aged 18-64 years (aOR = 2.57)
(interaction term, p = 0.05).
Discussion
In his mukistateanalyss of hospitalizations for COVID-19-lke
illness among adults aged 218 years during January-September
2021 whose previous infection or vaccination occurred 90-179 days
earlier, the adjusted odds of laboratory-confirmed COVID-19
"were higher among unvaccinated and previously infected patients,
than among those who were fully vaccinated with 2-doses of an
mRNA COVID-19 vaccine without previous documentation of
SARS-CoV-2 infection, Secondary analyses that did not adjust for
time since infection or vaccination or adjusted time since infection
or vaccination differently as well as before and during Delta
variant predominance produced similar results. These findings are
consistent with evidence that neutralizing antibody tersafter receipt
oF 2 doses of mRNA COVID-19 vaccine are high (5.6); however,
these findings differ from those of a retrospective records-based,
DMAKWR / October29,2021 / Vol. 70 3
Early Release
‘TABLE 1. (Continued) Characteristics of COVID-19-likellness hosptalizations* among unvaccinated adults with a SARS-CoV--2 infection occurring
90-179 days before the index test date’ and among adults who were fully vaccinated® 90-179 days before the index test date’ without 3
previous documented SARS-CoV-2 infection — nine states, January September 2021
Tio. (cokamn
‘Unvaccinatedwith previous Fully vaccinated without Standardized mean or
Characteristic SARS-CoV-Zinfection previous documented infection proportion diference”™
site
Columbia University 39 23818) 073
HealthParners 20 3401)
Intermountain Healthcare nan 45407)
Kaiser Permanente Norther California 254 25) 3614057)
Kaiser Permanente Northwest, 303) 250 (8)
Regenstie institute 300138) 1145.08)
University of Colorado 154105) 5336)
Time since either previous SARS-CoV. infection o fullmRNA vaccination until COVID-19-Lke illness index test date days
90-119 367 36) 3325 (53) oa
120-149 35335) 210163)
150-179 30029) ‘02104)
CCOVID-19 vaccination status
Unvaccnated 11020 100) 0) NA
Pier SiiVTech(BNT16262) oO 3736158)
Moderna (mniNA-1273) om 2592141)
‘Abbreviation: NA =not applicable,
* Medical events with decharge cod consstent with COVID-10-ke ines were included, COMID-19-Ike ines diagnoses included acute espatory ines (2,
COVID-19,resprtory alr oF pneumonia or related signs or symptoms (cough fever dyspnea, vomiting ore) using dlegnosiscodesfrom the ntemetione)
Clastieation f Diseases nth Revision and Internationa Cleeafetion of Diseases, Tenth Revision Cimisan ordered molecular assays (e. realtime reverse
‘wansciption-polymerase chain reaction for SARS-CoV'2 occurring =14 days before to <72 hous after hospital admission were included
"Inde test date wae defined a the date of respiratory specimen colectionasaciated withthe most racent poave or negative SARS-CoVe? test result before the
hospitalization or the hospitalization date if testing only occured after he admission.
Ss Ful vaccination was defined a receipt ofthe second dose a Pier ioNTach or Madera mRNA vaccine »14 days before the index test date
‘Partners contributing hospitalizations were in Calfornia, Colorado, Indiana, Minnesota and Wisconsin, Oregon and Washington, Utah and NewYork
‘In comparing characteristics between unvaccinated aduls with 2 previous infection and full vaccinated adults without a previous documented infection, @
Standardized mean or proportion diference 0.2 was considered noteworthy, After balancing characteristics thot fered between the two compotion groups,
the standardized mean or proportion differences were <0.6.
“Other race includes Asian Hawallan or Othe Paci slander, American Indian or Alaskan Native, Other not sted and multiple races.
cohort study in Isae,"* which did noc find higher protection for
vaccinated adults compared with those with previous infection
during period of Delta variant circulation, This variation s possibly
relared to differences in the outcome of interest and restrictions on
the timing of vaccination. The Israeli cohort study assessed any
positive SARS-CoV-2 test result, whereas this study examined
Inboratory-confirmed COVID-19 among hospitalized patients
‘The Israeli cohort study also only examined vaccinations that had
cccurted 6 months earlier, so the benefit of more recent vaccination,
‘was not examined. This report focused on the early protection
fiom infection-induced and vaccine-induced immunity, hough ic
ispossble that estimates could be affected by time, Understanding
Infection-induced and vaccine-induced immunity over time is
important, particularly for fururescudies to consider.
In this study, the benefit of vaccination compared with infec-
tion without vaccination appeared to be higher for recipients
of Moderna than Pfizer-BioN Tech vaccine, which is consistent
with a recent study that found higher vaccine effectiveness
against COVID-19 hospitalizations for Moderna vaccine recip
ients than for Pfizer-BioNTech vaccine recipients (7). In this,
TW inepalTowwanedoaicory/comtenc/10.1101/2021.08.24.2126241501
4 MMWR / October 29,2021 / Vo.70
study, the protective effec of vaccination also trended higher
for adults aged 265 years than for those aged 18-64 years
However, considering the limited data by both product type
and age, additional research is needed on the relative protec-
tion of vaccination versus infection without vaccination across
demographic groups and vaccine products, as well as vaccina-
tion in previously infected persons.
“The findings in this report are subject to at east seven limita-
tions, First, although this analysis was designed to compare two
groups with different sources of immunity, patients might have
been misclassified. IF SARS-CoV-2 testing occurred outside of
network partners’ medical facilities or if vaccinated persons
are les likely to seek testing, some positive SARS-CoV2 test
results mighthave been missed and thus some patients classified
as vaccinated and previously uninfected might also have been
infected. In addition, despite the high specificity of COVID-19.
‘vaccination status from these data sources, misclassification is
possible. Second, the aOR could not be further stratified by
time since infection or vaccination because of sparse data and.
limited ability to control for residual confounding that could,
be magnified within shorter intervals, The aOR that did not
adjust for time might also be subject to residual confounding,
Early Release
TABLE 2. Adjusted odds ratios* of laboratory-confirmed COVID-19 among hospitalizations in adults with COVID-19-tike illness comparing
tunvaccinated adults with a SARS-CoV-2 infection occurring 90-179 days before the index test date and adults who were fully vaccinated
90-179 days before the Index test date without a previous documented SARS-CoV-2 infection — nine states, January-September 2021
No. row of
SARS COV'2. Adjusted odés ratio
outcome Totalna,_postvetetresuts (95%
‘Aad faged 218 yor) any COVID-19 RNA voccine
Any mRNA vaccine
Faly vacated without previous documented infection 632832415) fet
Unvacinated wth a previous SARS-CoV? infection Yoo “8908 549 (275-1099)
Any mRNA vaccine no restiton of time since previous infection or completion of vaccination
Faly vacated without prevous documented infection we37 54200) fe
{range of ie since vacation ~ 0-713 days tore hospitalization
Unwacinoted wth a reviou SARS-CoV 2inecton 2005 130462) 275(190-398)
{range of me since prevosinfstion - 50-94 days before hosetalation)
‘ny mRNA vaccine examining the potential influence of ime since prevousinfcton or completion of vaccination
Fully vaccinated” without previous documented nection limited to those wih ongestpeiog 12231 458(3.7 ref
Sincevacination ange of tnesince vocation = 45-213 dys belorehosptalation
Unvacnated witha previous SARS-CoV2 infection imied to those with marerecent infections 1388107 7.71 396(249-635)
{range of ime since prevousinfection - 50-225 days before osptalaton)
‘Any mRNA vaccine adjusting fr time since previous infection or completion of vaccination n model
Fall vochated witout pes documented infection 6028 324651) fet
Unvacenated wth a previous SARS-COV"? infection Yoo 89087) 322(168-620)
8 time relative to SARS-CoV-28.1.6172 (Det) varant predominance
Before Dela predominance January-June 2021)
Fal vaccinated without previous documented infection as 808) te
Unvacnated wth a prewous SARS-CoV fection on 70184) an 28-1316
During Det predominance UuneSeptember 2021)"
Falyvaccsted’ witout pevous documented infection 5230655) fe
Unvaceated wth a previous SARS-CoV? infection 1 191100) 755 045-1652
By mRNA vacine product?
Piizer BioN Tech (BNT16262)
Fully vaccinated! without previous documented nection 373815658) fet
Unvacinated wth a previous SARS-Co¥? infection yoo “89087) 511 283-1029)
Moderna mRNA-1275)
Ful vacated without prevous documented infection 252109442) ff
Unvaccnated witha previous SARS-CoV? infection 100 85087) 7.30(640-1560)
By age group, yst
rest
Ful vaccinated? without previous documented infection 125 7150) fe
Unvecinated wth a previous SARS-CoV? infection 5649488) 27014-4165)
365
Fully vacated” without previous documented infection aos 253152) fe
Unvaccnated witha preous SARS-CoV? fection as 0186) 1957 (634-4591
‘Abbreviations: CI= confidence interval ref = referent group,
* Odds flios were adjusted forage, geographic region, calendar tine (days since January 1, 2027), and lca vts culation (percentage of SARS-CoV2 postive
results rom testing within the counties surrounding the fcity on the date ofthe hospitalization) and balanced using mverse weights on characteristics thet
Gere between the we groups (calculated separately or each odds ato mode! using faclity characteristics, sociodemographic characterises and underying
‘medical conditions. Cardiovascular dlgease was also adjusted n the main model and in the model for PizerBioNTech. Any Ikelyimmunesuppression was also
Included inthe model for Modema, Neuromuscular and rsptatory conitons were ako adjusted inthe model for adults aged 265 years Number of days since
previous infection or completion of vaccination instead of clend time, was adjusted in the model within the stated secondary analysis
{Full vaccination was defined as receipt of the second dose of Pfr SioNTech or Madera mfINA vaccine =14 days before the index test date
{3 Pwaluefrom assessment of effect modiiation by mRNA product was 402,
{1Pwaluefor interaction term for exposure group by age group was 005.
= SARS-CaV.2B 1617 2 (Delta variant predominance began on the date the Delt variant accounted for >50%of sequenced isolates in each meta fait’ state
ttpsfdoLorg/10.1888Smmvitmmn7037e2
particularly related co waning of both types of immunity. Third,
selection bias might be possible if vaccination status influences
likelihood of testing and if previous infection influences the
likelihood of vaccination, Previous work from the VISION net-
work did not identify systematic bias in testing by vaccination,
status, based on data through May 2021 (1), Fourth, residual
confounding might exist because the study did not measure
‘or adjust for behavioral differences berween the comparison
‘groups that could modify the risk of che outcome. Fifth, these
results might not be generalizable co nonhospitalized patients,
who have different access to medical care or different health
‘eare-secking behaviors, particularly outside of the nine states
DMAKWR / October29,2021 / Vol. 70 5
Early Release
covered, Sixth, the statistical model incorporated the use of a
weighted propensity score method which is subject to biases,
in estimates or standard errors if the propensity score model,
is misspecified. Numerous techniques were used to reduce
potential suboptimal specification of the model, including buc
not limited to including a large set of covariates for machine
learning estimation of propensity scores, including covariates in
both regression and propensity models, ensuring large sample
sizesand checking stability of weights, and conducting second-
ary analyses to assess robustness of results. Finally, the study
assessed COVID-19 mRNA vaccines onlys findings should
not be generalized to the Janssen vaccine.
In this U.S.-based epidemiologic analysis of patients hospi-
talized with COVID-19-like illness whose previous infection,
or vaccination occurred 90-179 days earlier, vaceine-induced
immunity was more protective than infection-induced immunity
against laboratory-confirmed COVID-19, inchiding during a
petiod of Delta variant predominance. All eligible persons should,
be vaccinated against COVID-19 as soon as possible, including
unvaccinated persons previously infected with SARS-CoV-2.
‘Acknowledgments
Jeffenon Jones, Claire Midgley, Ruth Link-Glks, Sharon Saydab,
Jerome Tos, Adi Gundlapall, Natalie Thornburg Aga Shefr, John
Kool, Erin Tromble, Meissa Caer, Cory Kokko, Stephanie Weaver,
Kushali Muthumalaippan, Bio-Ping Zhu, Roumiana Boneva, CDC.
‘Coneapondng author: Caterne H, Bono, 7@ede pu
TEDE COVID-I9 Response Team: Center for Biomedical Informatics
Regenatit Insitute Indianapolis, Indiana; diana University School of
“Maticns, Indianapolis, India, "Center for Eleth Reseach, Kater Petmanente
‘Nanhses, Portland, Oxgon Deparment of Medicine, Univesity of Colorado,
‘Anachate Medical Campus, Aurora, Colorado “West, Rockville, Marland:
"earners faite, Minneapolis Mins Depurtmenc of Brome
Iaformatics, Columbia Universi, New Yor, New Yorks °New York Prbyteian
Hospital, New Vrk ity, New York Kaiser ermanente Verne Stn Center,
Keser Permanente Northern Caloris, Oakland, California: Finks Schoo
‘of Public Health, Indiana University Indianapolis, Indiana; ?Divsion of
Infectious Dace and Clinical Epidemiology Iermoantin Healthcare, Salt
Lake iy Uh, Baylor Scot 8 White Health, Teas ASM University College
‘of Medicine. Temple. Teas; Childress Minasoa, Minneapolis, Minnesota
"Regen Ines, Indnspalis Indian
All authors have completed and submitted the International
Commixtee of Medical Journal Editors form for disclosure of
potential conflicts of interest. Stephanie A. Irving reports support
from Westat to Kaiser Permanente Northwest Center for Health
Research. Nicola P. Klein reports support from Pfizer to Kaiser
Permanente, Northern California for COVID-19 vaccine clinical
trials, and institutional support from Merck, GlaxoSmithKline, and
Sanofi Pasteur outside the current study. Charlene McEvoy reports,
support fiom AstraZeneca o HealthPartnes Institue for COVID-19
vaccine tras. Alison L. Naleway reports Pfizer Research funding to
‘summary
‘What i aleady known about this topic?
Previous infection with SARS-CoV-2 or COVID-19 vaccination
‘can provide immunity and protection against subsequent
‘SARS,CoV’2 infection and illness.
‘Whatis added by this report?
Among COVID-19-tke illness hospitalizations among adults
‘aged =18 years whose previous infection or vaccination.
‘occured 90-179 days earlier, the adjusted odds of laboratory-
‘confirmed COVID-19 among unvaccinated adults with previous
‘SARS-CoV'2 infection were 5.49-fld higher than the odds,
‘among fully vaccinated recipients ofan mRNA COVID-19
‘vaccine who had no previous documented infection (95%
‘confidence interval= 2.75-10.99).
What are the implications for public heath practice?
Alleligible persons should be vaccinated against COVID-19 as
‘soon 25 possible, including unvaccinated persons previously
infected with SARS-CoV-2,
Kaiser Permanente Northwes for unrelated study of meningococcal B
vaccine safety during pregnancy. Suchitra Rao reports grants from
GlaxoSmithKline and Biofire Diagnostics. No other potential
conflicts of interest were disclosed.
References
1. ThompsonMMG, Senchjam E, Grams eal Eevee of Covi 19 vaccines
in ambulatory and inpatient cae serting: N Engl J Med 2021:385:1355-71
PRID'34496194 pds on 10.1056) NEJMes21 10362
annis SJ, Rowley EA, Ong TC, etal: VISION Nerwork. Ines
‘estimates of COVID-19 vaccine effectiveness against COVID-19-
associated emergency department or urgent care clinical encounters and
hospitalizations among adults during SARS-CoV.2 B.L.617.2 (Del)
variant predomninance—-nine states, June-August 2021. MMWR Mor
Moreal Wly Rep 2021:70:1291-3. PMID:34529642 hurpst/doi
‘ong/10.15585 ramon 7037e2
3. Mansion R, Joe MM, Sun W, Hennesy S. On the estimation and use of
propensity scores in catecoattol and eac-cohore sie. Am J Epidemiol
2047 :166'382-9, PMID:17504780 haps. op, 1093/69
Maraall SW. Power for tests of iteration: effet of taxing the Type 1
‘error rate. Epidemiol Perspect Innov 2007%4r4, PMID:17578572 hep)
ddoj.ory/10-1186)1742-5573-4-4
5, Bdars VV, Hudson WH, Xie X, Ahmed Ry Suthar MS, Neutrlising
antibodies against SARS-CaV2 variants after infection and vaccination,
JAMA 20213325:1896-8, PMID:33739374 hepefd.org10 1001)
jama.2021.4388
6 dara WV, Pinsky BA, Suchar MS, etal, fection and vaesine induced
rewraliing-antibody responses to the SARS-CaV’2 B.1.617 variants
N Engl } Med 2021;385:664-6, PMID:34233096 heeps! do,
‘rg/10.1056/NEJMc2107799
7. Self WH, Tenforde MW, Rhoads J ca; IVY Neework. Comparative
celfeciveness of Moderna, Pizer BioN Tec, and Janssen Johnson 8
Johnson) vaccines in preventing COVID- 19 hospitalizations among adults
{without immunocompromining conditions-—United States, March~
‘August 2021. MMWR Morb Moctal Wkly Rep 2021,70:1337—43.
PMUD:34555004 hueps:/doiog/10.15385/mmwemun7038el
Readers who have difficulty accessing this PDF file may access the HTML file at hurps/#www.cdegov/mmv/volumes/70¢vwr/mm7044e1
hhum’s_cidemm7044el_v. Address all inquiries about the MMWR Series, including material to be considered for publication, to Editor,
‘MMUWR Series, Mailstop V25~
6 MMWR / October 29,2021 / Vo.70
CDG, 1600 Glifon Rd, N.E. Atlanta, GA 30329-4027 or co mmwrrq@edc.gov.
Christopher Funk (CENSUS/NPC FED)
Fri, § Nov 2021 14:12:41 +0000
Bozio, Catherine H. (CDC/DDID/NCIRD/ID)
Subject: Fw: New CDC Study: Vaccination Offers Higher Protection than Previous
Infection
Hello,
Ihave been directed to ask you questions regarding a study the CDC is using to promote the
covid vaccine. The study appears to contradict several other studies that have been completed
this year,
Question: The study in question states that 7.348 patients met the criteria for either exposure
category. Of the 7,348 patients, 1,020 were previously infected and unvaccinated, and 6,328
were fully vaccinated. One would reason that this study indicates that individuals who are fully
vaccinated are 6 times more likely to be hospitalized from Covid-19 like illness than those who
were previously infected and unvaccinated.
‘Would someone like to comment on this?
One other point, Laboratory confirmed Covid-19 infection was identified among 324 fully
ated patients, and 89 unvaccinated previously infected patients. This would also indicate
that fully vaccinated patients are being hospitalized from laboratory confirmed Covid-19 at a rate
that's 4 times greater than those who were previously infected and unvaccinated,
Would someone like to comment on this?
Chris Funk
Supervisor, Facilities Management
Support Services Branch
US. Census Bureau
Office: 812-218-3440
Christopher.funk@census.gov
Census.gov
From: MM\WR Questions (CDC)
Sent: Friday, November 5, 2021 10:01 AM
To: Christopher Funk (CENSUS/NPC FED)
Subject: New CDC Study: Vaccination Offers Higher Protection than Previous Infection
Thank you for contacting MMWR, Please contact the corresponding author Catherine H.
Bozio, ise7@cdc.gov. , for your concerns
Best,
MMWR
New CDC Study: Vaccination Offers Higher Protection than Previous COVID-19 Infection
CDC Online Newsroom | CDC
Laboratory-Confirmed COVID-19 Among Adults Hospitalized with COVID-19-Like Illness
with Infection-Induced or mRNA Vaccine-Induced SARS-CoV-2 Immunity — Nine States,
January-September 2021 | MMWR (cde.gov)
Question: The study in question states that 7,348 patients met the criteria for either exposure
category, Of the 7,348 patients, 1,020 were previously infected and unvaccinated, and 6,328
were fully vaccinated. One would reason that this study indicates that individuals who are fully
vaccinated are 6 times more likely to be hospitalized from Covid-19 like illness than those who
were previously infected and unvaccinated. Would someone like to comment on this?
One other point. Laboratory confirmed Covid-19 infection was identified among 324 fully
vaccinated patients, and 89 unvaccinated previously infected patients. This would also indicate
that fully vaccinated patients are nearly 4 times as likely to have a hospitalization from
laboratory confirmed Covid-19 than those who were previously infected and unvaccinated,
‘Would someone like to comment on this?
Chris Funk
Supervisor, Facilities Management
Support Services Branch
U.S. Census Bureau
Office: 812-218-3440
Christopher.funk@census.gov
Census. gov
From: CDCInfo
Sent: Wednesday, November 3, 2021 10:58 AM
To: Christopher Funk (CENSUS/NPC FED)
Subject: CDC-INFO; Topic New CDC Study: Vaccination Offers Higher Protection than Previous
Infection; [CDC-2148313-H3Y 1C7] CRM:09155124
‘Thank you for your inquiry to CDC-INFO.
So CDC can verify the most current information and best respond to your inquiry, would you
please more specifically cite what new CDC study you were referring to, perhaps the title, and
where you saw it (document, Web link, ete.) This information will help us respond to your
inquiry,
CDC-INFO is a service of the Centers for Disease Control and Prevention (CDC) and the
Agency for Toxic Substances and Disease Registry (ATSDR). This service is provided by the
Verizon and MAXIMUS contract with CDC and ATSDR
Original Message
Se
From: General Public
Subject: New CDC Study: Vaccination Offers Higher Protection than Previous Infection
11/3/2021
Email Address: christopher.funk@census.gov
Question: The study in question states that 7,348 patients met the criteria for either exposure
category. Of the 7,348 patients, 1,020 were previously infected and unvaccinated, and 6,328
were fully vaccinated. One would reason this study indicates that individuals who are fully
vaccinated are 6 times more likely to be hospitalized ftom Covid-19 like illness than those who
were previously infected and unvaccinated. Would someone like to comment on this?
One other point. Laboratory confirmed Covid-19 infection was identified among 324 fully
vaccinated patients, and 89 unvaccinated previously infected patients. This would also indicate
that fully vaccinated patients are nearly 4 times as likely to have a hospitalization from
laboratory confirmed Covid-19 than those who were previously infected and unvaccinated.
Would someone like to comment on this?
Thank you,
Chris Funk
Optional Information
Name: Chris Funk
Title: Facilities
Organization: Census Bureau
Phone: 8122183440
Other Email: christopher.funk@census.gov
Address:
PI Extraction:
Bozio, Catherine H. (CDC/DDID/NCIRD/ID)
Sat, 30 Oct 2021 00:51:38 +0000
Choban, Ana (CDC/DDID/NCIRD/ID)
Subject: FW: Laboratory-Confirmed COVID-19 Among Adults Hospitalized with COVID-
19-Like Illness with Infection-Induced or mRNA Vaccine-Induced SARS-CoV-2 Immunity — Nine States,
January-September 2021
Best,
Catherine
Original Messay
From: GERALD A SANTULLI mer
Sent: Friday, October 29, 2021 8:45 PMT
To: Bozio, Catherine H. (CDC/DDIDINCIRDIID)
Subject: Laboratory-Confirmed COVID-19 Among Adults Hospitalized with COVID-19-Like Ilness with
Infection-Induced or mRNA Vactine-Induced SARS-CoV-2 Immunity — Nine States, January-September 2021
Good evening Dr. Bozio,
ve read with interest the article you co-authored and released today.
Thave a couple of questions that woutd help clarify your study and it’s conclusions for me,
1. “The outcome of laboratory-confirmed COVID-19 was defined as COVID-19-like illness and a positive SARS-
CoV-2 result from molecular testing.
Could you provide additional information on the PCR tests for both the natural immunity group and the vaccinated
group? Were the same CT eycles used for both the natural immunity and vaccinated groups and what were the CT
eycles used in your study’?
2. Would it be possible to show your calculations for the adjusted odds ratio [aOR] and how you derived $.49? Itis
rot explained in the article,
‘Thanks very much,
Gerald Santulli, DMD
Mali Ross
Thu, 4 Nov 2022 15:59:00 +0000
Bozio, Catherine H. (CDC/DDID/NCIRD/ID)
Help w/Calculation
Good Morning Ms. Bozio,
| read your study on the CDC website that concluded that unvaccinated people with a previous
infection were 5x more likely to have a positive COVID-19 test, Laboratory-Confirmed COVID-19
Among Adults Hospitalized with COVID-19-Like Illness with Infection-Induced or mRNA
Vaccine-Induced SARS-CoV-2 Immunity — Nine States, January~September 2021 | MMWR
(cde.gov)
When | scrolled down to the numbers used for the study, I could not figure out how you came
up with that figure of 5x more likely. I'm sure you are very busy, but is there any way you could
have someone walk me through this?
Much appreciated,
Amalia Ross
EPIX Update (CDC)
Fri, 29 Oct 2022 13:36:40 -0400
Bozlo, Catherine H. (CDC/DDID/NCIRD/ID)
Subject: Important: MMWR Early Release: Laboratory-Confirmed COVID-19 Among
Adults Hospitalized with COVID-19-Like illness with Infection-Induced or mRNA Vaccine-Induced SARS-
CoV-2 Immunity — Nine States, Jan-Sep 2021
The Epidemic
Information Exchange
Check Epi-X for an Important Report
MMWR Early Release: Laboratory-Confirmed COVID-19 Among Adults Hospitalized with COVID-19-Like
Ilness with Infection-Induced or mRNA Vaccine-Induced SARS-CoV-2 Immunity — Nine States, Jan-Sep
2021
Alleligible persons should be vaccinated against COVID-19 as soon as possible, including unvaccinated
persons previously infected with SARS-CoV-2. This MMWR is available through this posting or here.
hitpsi//epix2, cdc.goviv2/Reports/Display.aspx?id=411994
HOW TO CONTACT Epi-x
For technical issues, contact the Help Desk:
iXHel
(877) 438-3749
For help with preparing or posting a report, contact the Editor on Call;
EpixEditor@cde.gov
(877) 862-2392 (toll free within the United States)
HOW TO MANAGE Epi-X NOTIFICATIONS
‘Manage your notifications
ABOUT THIS E-MAIL
You have received this message because you are an authorized Epi-X user.
Information In this message must be used only In accordance With the Epi-X User Agreement.
CDC IMS 2019 NCOV Response STLT Partner Engagement
Thu, 28 Oct 2022 19:39:55 +0000
CDC IMS 2019 NCOV Response STLT Partner Engagement; Briggs-Hagen, Melissa
(COC/ODID/NCIRD/DVD); Taylor, Christopher A. (CDC/DDID/NCIRD/DVD); Bozio, Catherine H
(CDC/DDID/NCIRO/ID); Neatherlin, John C. (CDC/DDPHSIS/CGH/DGHP); Budzyn, Samantha
(CDC/ODPHSS/CSELS/OHIS) (CTR); Routh, Janell A. (CDC/ODID/NCIRD/DVD); Wojno, Abbey
(COC/ODID/NCEZID/OGMAQ); Galloway, Summer (CDC/DDID/NCIRO/ID}; Noelte, Kate
(COC/DDPHSIS/CPR/DStR); Limbago, Brandi (CDC/DDID/NCIRD/OD); Laufer Halpin, Alison S.
(CDC/DDID/NCEZID/DHAP); Haller, Elizabeth (CDC/DDID/NCHHSTP/DASH); Hall, Aron
(CDC/DDID/NCIRD/DVD); Burton, Deron (CDC/DDID/NCHHSTP/OD); Brooks, John T.
(COC/DDID/NCHHSTP/OHP); Hicks, Lauri (COC/ODID/NCEZID/DHAP); Mahon, Barbara
(CDC/DDID/NCIRO/OD)
ce: Honein, Margaret (Peggy) (CDC/ODID/NCEZID/OPEI); Weakland, Aliki P
(CDC/DDID/NCEZID/DPE!); Walker, Desiree (CDC/DDPHSIS/CPR/DSLR) (CTR); Montero, Jose
(COC/DDPHSIS/CSTLTS/OD); CDC IMS Response Coordinator -2; CDC IMS AV/Communications; CDC IMS
2019 NCOV Response Deputy Incident Manager; Johnson, Shyonna (CDC/DDNID/NCBDDD/DBDID) (CTR);
Daskalakis, Demetre (CDC/DDID/NCHHSTP/OHP); Dowell, Deborah (Debbie) (CDC/DDNID/NCIPC/DOP);
CDC IMS 2018 NCOV Response IM-PDIM Special Assts; Anderson, Mark (CDC/DDPHSIS/CGH/OGHP);,
Kingsbury, Keighlee (COC/DDNID/NCBDDD/DBDID) (CTR); Harris Sharpe, Bria
(CDC/DDNID/NCBDDD/DBDID); Auerbach, John (CDC/OD); Bautista, Lucia (CDC/DDID/NCIRD/OD) (CTR);
Kirby, Emily (CDC/NIOSH/OD); Fell, Tiffany K. (COC/DDNID/NCCOPHP/DHDSP); Fox, Kimberley
(CDC/ODID/NCIRD/DBO); Layden, Jennifer (COC/DOPHSS/0S/00); Barrios, Lisa C.
(COC/DDID/NCHHSTP/DASH); Thomas, Craig W. (CDC/DDNID/NCCDPHP/DPH); Mowbray, Amy L
(CDC/ODNID/NCEH/OLS); Braden, Chris (CDC/DDID/NCEZID/OD); Cohn, Amanda
(CDC/DDNID/NCBDDD/DBDID); Mueller, Trisha (CDC/DDNID/NCCDPHP/DRH); Remley, Karen
(COC/ODNID/NCBDDD/OD); Modi, Surbhi V. (CDC/DDPHSIS/CGH/DGHT); Peeples, Amy B.
(COC/DDNID/NCIPC/OD); MeCalla, Haley (COC/OD/OCS)
Subject: INTERNAL CDC All-State, Tribal, Local, and Territorial Update Call
Attachments: Standing Panelist and Task Force Zoom Links Updated 11.01.2021.docx,
11.01.2021 INTERNAL AIL-STLT Update Call Agenda F.docx
Panelist Inform:
yn: The All-STLT Update Call will now be held as a Zoom webinar. You will rec
Zoom “Panelist” link to login. This link is unique to you; you will use the same link for the remainder of
the calls for 2021. Do not share your link. If you share your link, the person that uses it will show up in
the Zoom meeting as your name which could create confusion. Your link is also listed in the attached
document.
Policy and public health partnerships will continue to keep an internal calendar invitation as
a placeholder on your calendar. We will share the agenda and the previous weeks’ notes there.
‘Add the link to your calendar as a reoccurring weekly event: To add this link to your calendar, select
the “Add to Calendar” link within the email you receive. This will download the .ics file. Open the file and
save the event to your calendar. Please ensure that you set this invitation to reoccur weekly.
Each week you will receive a reminder email with your link.
Call Purpose: CDC's 2019 Novel Coronavirus (COVID-19) response team will host a national cal series
every Monday from 2:00 p.m. to 2:45 p.m. EST to provide state, tribal, local, and territorial partners
(STLT) with the latest information on the COVID-19 outbreak and U.S. preparedness efforts.
Invited call participants include STLT preparedness directors, epidemiologists, health officials, public
health laboratory directors, and nongovernmental partners. Participant information can be found
below.
CDC All-STLT Update Call Dates 2021
‘The All-STLT Update Call will be on Mondays from 2 to 2:45 PM EST except for the dates below where
the call will be on a Tuesday.
CDC All-STLT Update Call Task Force Links
Team Email Zoom Information.
STLT Support| Eocevent#2a@ede
Task Force gov
ChiefHealth | Eoceventaaam@ede
Equity Officer | gov
(CHEO)
‘Community Focevent357@cdc.
Interventions | gov
Critical
Populations
(CICP) Task Force
Data, Analytics, | Eocevent463@ede,
and gov
Visualizations
(av)
Epidemiology | Eocevent422i@cde.
and Surveillance | gov
Task Force
Global Migration | Eocevent213@cde
Task Force gov me
(ome)
Health Systems | Eocevent2i8@cde
and Worker | gov
Safety (HSWS)
International | Eocevent223@cde,
Task Force gov
Tolat eccliclead@cdeg
Information | ov
Center (IC)
Taboratoryand | Eocevent521@cde
Testing Task | gov
Force
Partnerships and | eocevent337@cde
Risk gov
‘Management
(Pam)
‘Vaccine Task | Eoceventai7@cdc
Force gov
Incident Eoceventag@edc.
Manager gov
Deputy Incident | eocevent259@ede
Manager ov
Chief Medical | Eocevent270@cde
Officer ov
CDC Panelist | Eocevent387i@cde,
(Non-covin | gov
Response
Update)
16
Standing Panelist Links
Standing Panelist
Email
Zoom information|
Barbara Mahon Bdma@cdegou
‘Mark Anderson Mes6@cde-gou
John T. Brooks zudd@cdegov
Debbie Dowell dov@edegov
‘aur Hick wus @cdcnov
os)
Pragna Patel
pips@edegov
Greta Masset u6@cdc.nov
‘Jose Montero Zan3@cdegov
Keighlee Kingsbury (Executive ans@edegov
Assistant for STLT TF leadership)
John Auerbach jxad@cdc gov
Chris Braden erbS@cdegov
‘Amy Mowbray himB@cdexov
Kate Noalte wis@edegov
‘Surbhi Modi DkU@adcigov
x)
Desi Alexander (IT support IM)
DiyS@cdenov
Rolled Off
‘Celeste Philip Wav@edcgov
William Carson PyeT@cdc gov
‘Cassie Sager Vied@cdegov
Emily Maz Pyo9@ede.gov
Jordan Moody Pyp2@ede.gov
Internal Agenda
CDC COVID-19 Al State, Tribal, Local, and Territorial (STLT) Update Call
Monday, November 1st, 2021 - 2:00 PM ~ 2:45 PM ET
@*Speakers please join at 1:45 PM for sound check
NOTE: The line will open to attendees at 1:55PM
Panelists received an email from STLT TF with their task force link
‘Please do not share your panelist link
Welcome and introductions: Kate Noelte, Senior-Advisor, STLT Support Task Force, CDC
Thank you for joining us today and welcome to those who are joining us for the first time.
The purpose of the call is to provide regular updates to state, local, Tribal and territorial
preparedness directors, epidemiologists and health officials; public health laboratory directors;
big city health coalitions; immunization services professionals; and nongovernmental partners
‘Asa reminder, this call s not for the media. If you are with the media, please disconnect now.
For those new to the call the call flow is as follows: CDC experts will share information on
several topics and there will be time for Q&A during the last portion of the call
© At any time during our call, we encourage you to put any questions you may have in
the Q&A box at the center bottom of the webinar window.
‘We want to remind you that the link you used to access today’s call is unique to you and is valid
for the duration of this call series ~so there is no need to re-register weekly. Simply save the
link and log in for the call each week.
Run of show for November 1":
MMWR: Severity of Disease Among Adults Hospitalized with Laboratory-Confirmed COVID-19
Before and During the Period of SARS-CoV-2 B.1.617.2 (Delta) Predominance — COVID-NET, 14
States, January-August 2021: Chris Taylor, COC
MMWR: Laboratory-Confirmed COVID-19 Among Adults Hospitalized with COVID-19-Like
Illness with Infection-Induced or mRNA Vaccine-Induced SARS-CoV-2 Immunity — Nine States,
January-September 2021: Catherine Bozio, COC
Updates to CDC Guidance for Institutions for Higher Education (IHE): John Neatherlin, CDC
Community of Practice: Kate Noelte, COC
Additional SMEs on for questions:
© $3: John Neatherlin, Elizabeth Haller
© Epi: Aron Hall and Deron Burton
© GMTF: Abbey Wojno
© Labs: Summer Galloway, Brandi Limbago, Allison Laufer Haplin, Melissa Carter
© VIF: Janell Routh
© CMO: Lauri Hicks
© Senior Science Advisor: John Brooks
(© Science Brief: SARS-CoV-2 Infection-induced and Vaccine-induced Immunity: John
Brooks, Melissa Briggs-Hagen
PPHP will place in chat at end of call:
© After the call additional questions can be directed to: eocevent424@cdc.gov.
© Upcoming All STLT Update Call: Monday, November 8
oxo)
Internal Agenda
CDC COVID-19 All State, Tribal, Local, and Territorial (STLT) Update Call
Monday, November 1st, 2021 - 2:00 PM ~ 2:45 PM ET
©)
EPI Update:
As of Monday, November 1"
Ene
‘Cumulative Total Daily 7-Day Dally Change from Prior 7- Cumulative 7-Day
Average DayPeriod Rate per 100K
‘cases? 53515386786 69.197 33% 1459
Hospital Admissions? 33239,473 4677 5137 104% 108
Deaths! 743,410 um 1108 28% 23
‘Test Volume! 622,802,391 1,398,516 21% 20928
‘Test Positivity! 75% 53% 55%
Response Update (NEM!)
xreo: HAS Protect. Additional information available on COU
D Data T¥a
or and in the DC COVID-19
Internal Agenda
CDC COVID-19 All State, Tribal, Local, and Territorial (STLT) Update Call
Monday, November 1st, 2021 - 2:00 PM ~ 2:45 PM ET
(Over 221.5 milin people or 66.7% of the population have received atleast 1 dose
“ee Grove Received at Least 1 Dose Fully Vaccinated
USOveral (6.2% (N = 221,520,153) '58.0% (N= 192,453,500)
12:17 Years of ge 59.0% (N= 13,430,186) 49.8% (N= 13,347,232)
212 Yeas of Age 780% (N=221,286 846) 67.8% (N= 192,317,895)
218 Years of Age 799% (N= 205,383,978) 69.6% (N= 179,729:970)
265 Years of Age 97.2% (N= 53,185,430) 85.3% (N= 46,665,304)
Dally(Hof Doses Current 7-Day Prior 7-Day Change rom Prior
Cumulative Total administred)* Dally Average Dally Average 7-Day Petiod
Doses Administered 22070088 ——«1A12416—NA)—+1:208517 768,503, 156.6%
First Doset 192453500 298686 (21.1%) 166,991 220,805 240%
Fully Vaccinated 221520353 208,573 (148%) 267,828 205,317 304%
Additional Doses 18,607,505 884,472(626%) 817,080 346,708, 11357%
uta of Oe 31, 2021, 060067
Seurces: ata Motoring and Reporting Seton, Vaccine Tsk Force COC COWD Tracker
ie Paved an 3, 290~ Oct 9,201 canted an pebble cae and eth Mumba recnaepering Sof 6. Agta od ath a
‘be nsnes in ~sat The tle he ae es 2 bers an ay eee ote toca eae ered ence here
‘unas we gen gre! oe npeoprte ne Of 130.84 strc enes eet retenne37 wee epareen he ne rece emer
‘dee L368 ne covet wel on 2608 mt pone 10.78 itr dered tent, weep en tbe mest eer
‘ee 2181 cen wed LIT te por we Aref tbe 2520, CO ogres copra COVE 9 cot ede et ea et
fevvsetng aay, sostnn 9 anode sag cette He
Te ped Aa 01, 2920-08221
"tne pra Mar OL, 220~Oe 2221: Tne peed tt ome 7 aeagead pent age Ot 2021 ~Oet 26,2021
“noe sto US ae OU eres, etre eta espace eta a abe" beh)
“unto incon tang on acer bf Sonn any cent ors hha fe preragey nae 10%
‘on e220 st reve ed parting estat n arth nd pts ata pry niente ED om no ened deca of 8783
Deployment Update
‘+ As of October 31, 2021, CDC has 17 field and remote teams deployed, including 66 deployers,
aiding states as they manage their response to the COVID-19 outbreak.
* CDC continues to deploy teams, as requested by states, to support epidemiology, data
management, case investigation and contact tracing, community mitigation, infection
prevention and control, health education and laboratory needs.
+ Teams also provide technical assistance for outbreaks in high-risk settings such as long-term care
and correctional facilities, as well as among at-risk populations.
Jurisdiction/Location | Team Deployment Start Deployment Mission
Date
Guam 10/29/2021 To investigate risk factors for COVID-19 transmission and severe
ase in Guam (despite high vaccination rates) to inform
strategies for testing, control and prevention of SARS-CoV-2
infection and guide the expansion of screening and laboratory
testing capacity in response the recent local surge in COVID-19
cases.
Internal Agenda
CDC COVID-19 All State, Tribal, Local, and Territorial (STLT) Update Call
Monday, November 1st, 2021 - 2:00 PM - 2:45 PM ET
10/25/2021
Evaluate the impact of modified quarantine strategies on
secondary transmission of SARS-Cov-2 among students,
teachers, and staff In the K-12 school setting in one Illinois
‘county: St. Clair County (east of St. Louls, MO). Specifically, one
field deployment team to travel to East St. Louis, IL from
October 25 through November 22, 2021.
Kentucky
10/25/2021
The mission of this deployment is to evaluate the impact of
modified quarantine strategies on secondary transmission of
SARS-Cov-2 among students, teachers, and staff in the K-12,
school setting in Lexington (Fayette County), Kentucky.
New Jersey
New Mexico
10/24/2021
10/25/2021
"The mission of this cruise ship inspections are to conduct on-site
inspections of passenger operating cruise ships to assess
‘compliance with CDC COVID-19 Operations Manual. Inspections
will ensure ships are properly mitigating risks of COVID-19
transmission amongst on board passengers and crew. On board
inspectional coverage will take place while the vessel is at the
port and/or while the vessel is underway. 2-5 inspectors will
participate in each inspection; port inspection will take ~8.
hours; underway inspections will last the duration of the sailing
voyage, typically between 2 and 3 days.
Evaluate the impact of modified quarantine (test-to-stay)
strategies on secondary transmission of SARS-Cov-2 among
students, teachers, and staffin the K-12 school setting in
‘Alamogordo, NM.
}
Internal Agenda
CDC COVID-19 Al State, Tribal, Local, and Territorial (STLT) Update Call
Monday, November 1st, 2021 - 2:00 PM ~ 2:45 PM ET
xs)
IV. Questions and answers
Internal Agenda
CDC COVID-19 All State, Tribal, Local, and Territorial (STLT) Update Call
Monday, November 1st, 2021 - 2:00 PM ~ 2:45 PM ET
$3: Elizabeth Haller
© Epi: Aron Hall and Deron Burton
© GMTF: Abbey Wojno
* Lab: Summer Galloway, Brandi Limbago, Allison Laufer Haplin Melissa Carter
© VIF: Janell Routh
© CMO: Lauri Hicks
* Senior Science Advisor: John Brooks
* Science Brief: SARS-CoV-2 Infection-induced and Vaccine-induced Immunity: John Brooks,
Melissa Briggs-Hagen
V. Speaker Panelist Links
[agenda Topic Breaker A
IMIMWR: Severity of Disease [chris Taylor
JAmong Adults Hospitalized
ith Laboratory-Confirmed
(OVID-19 Before and During
he Period of SARS-CoV-2
b.1.617.2 (Delta)
Predominance — COVID-NET,
ha States, January-August
021
IMIMWR: Laboratory-Confirmedkatherine Bozio
OVID-19 Among Adults
Hospitalized with COVID-19-
Like tlness with infection-
Iinduced or mRNA Vaccine-
Induced SARS-CoV-2 Immunity
- Nine States, January=
September 2021
[Updates to COC Guidance for ohn Neatherlin
Institutions for Higher
Education (HE)
oe)
Vi. Standing Panelist Links
Standing Panelist Emai Zoom information
Barbara Mahon ‘Bdm3@ede nov
(x6)
Internal Agenda
CDC COVID-19 All State, Tribal, Local, and Territorial (STLT) Update Call
Monday, November 1st, 2021 - 2:00 PM ~ 2:45 PM ET
‘Mark Anderson Mea6@cdegov
John T. Brooks wudi@edegou
Debbie Dowell ‘edo7@cdegov
{aur Hick auas@cdegou
Pragna Patel ‘pps @cdcgov
Greta Massetti aheG@ede gov (x6)
‘Jose Montero znn3@ede now
Keighlee Kingsbury ‘ons@edegov
(Executive Assistant for
STLTTF leadership)
John Auerbach pad@cdegov
Chris Braden ‘qb5@cdcgov
Internal Agenda
CDC COVID-19 All State, Tribal, Local, and Territorial (STLT) Update Call
Monday, November 1st, 2021 - 2:00 PM ~ 2:45 PM ET
‘Amy Mowbray him3@cdenov
Kate Noelte wiiB@edegov
‘Surbhi Modi bk@ede gov sia?
Desi Alexander (TT DhyS@cdegov
support IM)
Vil, Task Force Links
Team Email Zoom Information,
STLT Support | Eoceventé?4@cdc gov
Task Force
ChiefHealth | Eoceventéaa@cde.gov
Equity Officer
(CHEO)
Community Focevent357@cde gov
Interventions
Critical
Populations
{CICP) Task Force
Data, Analytics, | Eocevent463@cde gov oe)
and
Visualizations
(av)
Epidemiology | Eocevent422@cdegov
and Surveillance
Task Force
Global Migration | Eocevent2i3@cdegov
Task Force
(MTF)
Internal Agenda
CDC COVID-19 All State, Tribal, Local, and Territorial (STLT) Update Call
Monday, November 1st, 2021 - 2:00 PM ~ 2:45 PM ET
Health Systems | Eocevent2i8@cdeov
and Worker
Safety (HSWS)
International | Cocevent223@cde gov
Task Force
Toit eocliclead@ede now
Information
Center (IC)
laboratory and | Eocevent521@cdegov
Testing Task
Force
Partnerships and | eocevent337@cde gov
Risk
‘Management
(PRM)
‘Vaccine Task | Eoceventdi7@cdc gov (x6)
Force
Incident Foceventsag@ede gov
Manager
Deputy Incident | eocevent259@ede.gov
Manager
Chief Medical | Eocevent270@cde gov
Officer
COCPanelist | Eocevent382@cdagov
(Non-covio
Response
Update)
Mahanna Gabrielli, Elizabeth
Tue, 2 Nov 2021 12:17:59 +0000
Bozio, Catherine H. (CDC/DDID/NCIRD/ID)
Subject: Laboratory-Confirmed COVID-19 Among Adults Hospitalized with COVID-19-
Like lliness with Infection-Induced or mRNA Vaccine-Induced SARS-CoV-2 Immunity — Nine States,
January-September 2021
Dear Dr. Bozio,
First, | thank you for undertaking this study and releasing the results. | have many patients who
have had prior infection and who are hesitant to take the vaccine. And we have a real paucity
of data comparing infection-induced immunity vs vaccine-induced immunity vs no prior
immunity. And it makes it very difficult to convince well educated and knowledable patients
that the vaccine will give them a meaninful reduction in the risk of severe covi
However for your study, | do wonder how clinically significant the findings are? | am an
intensivist who takes care of COVID patients and nonCOVID patients alike. For me, the chance
of being positive for COVID in both groups was clinically quite low: 5.1 vs 8.7 in vaccinated vs
prior-infection induced immunity. While clearly there is an increased risk for the subjects that
had prior infection-induced immunity, this doesn't mean much to me unless compared with the
group with no known immunity (neither infection-induced nor vaccine-induced). Since you
have this data, are you able to compare to this third group? If the infection-induced immunity
group does not have a statistically reduced risk of having a positive COVID test while the
vaccine-induced group does have a statistically reduced chance of having a positive COVID test,
now that is clinically significant.
I don't know if you can use the same database, but the other very clinically significant question |
have is, In patients with a current positive COVID-19 PCR results, do subjects with prior vaccine-
induced immunity have a clinically significant reduced risk of severe covid as compared to
subjects with prior infection-induced immunity?
Thank you for performing this very important research!
Warm regards,
Elizabeth
Elizabeth Mahanna Gabrielli, MD
Assistant Clinical Professor of Anesthesiology, Perioperative Medicine and Pain Management
Division chief, Geriatric Anesthesiology
Division of Geriatric anesthesiology, Neuroanesthesiology, and Critical Care Medicine
31611 NW 12th Ave; C307
Miami, FL 33336
Celt
&
I: exm1044@med.miami.eduy
LynchJames WJR
Mon, 1 Nov 2021 19:23:51 +0000
Bozio, Catherine H. (CDC/DDID/NCIRD/ID)
MMWR article
Catherine H. Bozio, PhD
Dear Dr. Bozio
| read with interest your lead author publication entitled “Laboratory-Confirmed COVID-19
Among Adults Hospitalized with COVID-19-Like lines with Infection-Induced or mRNA
Vaccine-induced SARS-CoV-2 Immunity — Nine States, January-September 202
As a medical oncologist who cares for patients with lymphoproliferative disorders, | follow this
area very closely as the mortality in my patients approaches 30% when diagnosed with Covid. |
had several questions that | hope you may help me with.
1, Do you have any data about the severity of the illnesses in the patients who were either
vaccinated or previously infected compared to those who presented with a covid-like
illness and tested positive without previous infection or vaccination. Intuitively | would
guess these patients would fair less well that those with previous exposure.
2. Do you have any data about the mortality among the 2 groups studied? | ask because
the raw percentages between those with previous infection versus vaccination were 8.7
and 5.1 respectively. While I realize that the aOR with your statistical corrections was
5.5, this does suffer from the caveats you mention, that such analyses are always
Potentially confounded by innocent biases and modeling errors. | there were any major
difference in mortality of the hospitalization, this would seem important and compelling
Thanks for taking the time to perform this important work. | hope you will be able to offer some
insight as we all think through these important topics.
Sincerely
Jw!
James W. Lynch Jr, MD
Professor of Hematology/Oncology
Assistant Dean for Admissions
University of Florida Academic Health Center
Bozio, Catherine H. (CDC/DDID/NCIRD/ID)
Fri, 29 Oct 2022 12:01:36 +0000
Briggs-Hagen, Melissa (CDC/DDID/NCIRD/OVD); Thompson, Mark
(CDC/DDID/NCIRD/ID)
Subject: RE: Articles on infection and vaccine induced immunity.
Here's the citation (with correct title);
Bozio CH, Grannis SJ, Naleway AL et al. Laboratory-confirmed COVID-19 among adults hospitalized with
COVID-19-like illness with infection-induced or mRNA vaccine-induced SARS-CoV-2 immunity—nine
states, January-September 2021. MMWR Morb Mortal Wkly Rep 2021;70. Epub October 29, 2021
MMUR is trying to see if the DO! URL at the end of the citation,
Best,
Catherine
From: Briggs-Hagen, Melissa (CDC/DDID/NCIRD/DVD)
Sent: Thursday, October 28, 2021 6:46 PM
To: Bozio, Catherine H. (CDC/DDID/NCIRD/ID) ; Thompson, Mark (CDC/DDID/NCIRD/ID)
Subject: RE: Articles on infection and vaccine induced immunity.
Thanks for the heads’ up. The science brief also received feedback, now requiring additional last-minute
edits. Happy to correct your citation whenever you have an updated one to send my way. | guess we'll
just have to see how tomorrow goes! Would appreciate not having this level of stress in any future
projects...
Best,
Melissa
From: Bozio, Catherine H. (CDC/DDID/NCIRD/ID)
Sent: Thursday, October 28, 2021 3:47 PM
To: Briggs-Hagen, Melissa (CDC/DDID/NCIRD/DVD) ; Thompson, Mark
(COC/DDID/NCIRO/ID)
Subject: RE: Articles on infection and vaccine induced immunity.
Hi Melissa,
I wanted to give you a heads-up that the MMWR title is getting slightly modified. \’m hoping to get it
finalized by tonight and will share with you once it is finalized. Would that give you enough time to
modify the citation in the brief? Sorry for the down-to-the-wire changes!
Best,
Catherine
From: Briggs-Hagen, Melissa (CDC/DDID/NCIRD/DVD)
Sent: Wednesday, October 27, 2021 2:39 AM
To: Bozio, Catherine H. (CDC/DDID/NCIRD/I0) ; Thompson, Mark (CDC/DDID/NCIRD/ID)
Subject: Re: Articles on infection and vaccine induced immunity.
Great, thanks! Will add it before posting.
Melissa
Get Outlook for 105
From: Bozio, Catherine H. (CDC/DDID/NCIRD/ID)
Sent: Tuesday, October 26, 2021 10:02:35 PM
To: Briggs-Hagen, Melissa (CDC/DDID/NCIRD/OVD) ; Thompson, Mark
(CDC/ODID/NCIRD/ID)
Subject: RE: Articles on infection and vaccine induced immunity.
Hi Melissa,
I wanted to share the tentative MMWR citation, in case it's helpful:
Bozio CH, Grannis SJ, Naleway AL, et al. Laboratory-confirmed COVID-19 among adults with
infection-induced and vaccine-induced SARS-CoV-2 immunity hospitalized with COVID-19-like
illness — nine states, January-September 2021. MMWR Morb Mortal Wkly Rep 2021;70:xx—xx.
Best,
Catherine
From: Hall, Aron (CDC/DDID/NCIRD/DVD)
Sent: Tuesday, October 26, 2021 10:40 AM
To: Briggs-Hagen, Melissa (CDC/DDID/NCIRD/DVD) ; Bozio, Catherine H
(CDC/DDID/NCIRD/ID) ; Thompson, Mark (CDC/DDID/NCIRD/ID)
Subject: RE: Articles on infection and vaccine induced immunity.
Thanks, Melissa. Looks good to me.
From: Briggs-Hagen, Melissa (CDC/DDID/NCIRD/DVD)
Sent: Tuesday, October 26, 2021 10:36 AM
To: Hall, Aron (COC/DDID/NCIRD/DVD) ; Borio, Catherine H. (CDC/DDID/NCIRD/ID)
; Thompson, Mark (CDC/DDID/NCIRD/ID)
Subject: RE: Articles on infection and vaccine induced immunity.
Thanks all
Please see revised statement below. Catherin: DE
OH)
wer Please advise if any
further concerns, Thanks!
Best,
Melissa
ons)
From: Hall, Aron (CDC/DDID/NCIRD/DVD)
Sent: Tuesday, October 26, 2021 10:03 AM
To: Briggs-Hagen, Melissa (CDC/DDID/NCIRD/DVD) ; Bozio, Catherine H,
(CDC/DDID/NCIRD/ID) ; Thompson, Mark (CDC/DDID/NCIRD/ID)
Cc: Mahon, Barbara (CDC/DDID/NCIRD/OD)
Subject: RE: Articles on infection and vaccine induced immunity.
'm not suggesting any greater depth or additional comparisons in the brief, but that we just state the
(xs)
From the results of the MMWR:
Among COVID-19-like illness hospitalizations whose prior infection or vaccination occurred
90-179 days beforehand, the odds of laboratory-confirmed COVID-19 were higher among
previously infected patients than among fully vaccinated patients (aOR = 5.49; 95% Cl = 2.75
10.99) (Table 2). In secondary analyses, the aORs that examined the impact of whether and how
timing of infection or vaccination exposure was adjusted and aORs that stratified hospitalizations
before and during Delta variant predominance were all similar to the primary aOR estimate.
OC)
Aron
From: Briggs-Hagen, Melissa (CDC/DDID/NCIRD/DVD)
Sent: Tuesday, October 26, 2021 9:54 AM
all, Aron (CDC/DDID/NCIRD/DVD) ; Bozio, Catherine H. (CDC/DDID/NCIRD/ID)
«ise7?@cdc.gov>; Thompson, Mark (CDC/DDID/NCIRD/ID)
You might also like
- CDC ContractDocument37 pagesCDC ContractwalkafyreNo ratings yet
- FBI FOIA D'Antuono Transfer DocsDocument10 pagesFBI FOIA D'Antuono Transfer DocswalkafyreNo ratings yet
- DOJ Donoghue FOIA DocsDocument114 pagesDOJ Donoghue FOIA DocswalkafyreNo ratings yet
- Crossfire Hurricane - FBI Binder Installment Part 5Document14 pagesCrossfire Hurricane - FBI Binder Installment Part 5walkafyreNo ratings yet
- Memo of Law Re Sussmann 10.12.21 Exhibits - Part 1Document420 pagesMemo of Law Re Sussmann 10.12.21 Exhibits - Part 1walkafyre100% (2)
- Crossfire Hurricane Binder - Part 2Document209 pagesCrossfire Hurricane Binder - Part 2walkafyreNo ratings yet
- Memo of Law Re Sussmann 10.12.21 Exhibits - Part 3Document426 pagesMemo of Law Re Sussmann 10.12.21 Exhibits - Part 3walkafyreNo ratings yet
- Memo of Law Re Sussmann 10.12.21 Exhibits - Part 2Document473 pagesMemo of Law Re Sussmann 10.12.21 Exhibits - Part 2walkafyre0% (1)
- Memo of Law Re Sussmann 10.12.21Document18 pagesMemo of Law Re Sussmann 10.12.21walkafyreNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)