You might also like
- 2021VAERSDATA of 4-30-2021 - 410 Deaths of Age 59 and Under - Published by College of Scripting Music and Science On 5-8-2021Document32 pages2021VAERSDATA of 4-30-2021 - 410 Deaths of Age 59 and Under - Published by College of Scripting Music and Science On 5-8-2021CollegeOfScriptingNo ratings yet
- ObyGyn - OSCE (FG2)Document23 pagesObyGyn - OSCE (FG2)roorian100% (1)
- 2021 Va Ers DataDocument1,788 pages2021 Va Ers DataasdasdasdNo ratings yet
- TIVA Pocket Reference 2nd Edition (June 2013)Document42 pagesTIVA Pocket Reference 2nd Edition (June 2013)Charlene TanNo ratings yet
- Elizabeth Wettlaufer - Agreed Statement of FactsDocument57 pagesElizabeth Wettlaufer - Agreed Statement of FactsNick Westoll100% (3)
- NCM 114 Care For Older Adults MODULE 5Document5 pagesNCM 114 Care For Older Adults MODULE 5Meryville JacildoNo ratings yet
- CASE SCENARIO AppendicitisDocument6 pagesCASE SCENARIO AppendicitisJacob Estrada0% (1)
- Nail StructureDocument3 pagesNail StructureEdwin Baysa100% (1)
- Mumbai DoctorsDocument2 pagesMumbai DoctorsArthavruddhi CapitalNo ratings yet
- GW Investor Deck June 2018Document29 pagesGW Investor Deck June 2018medtechyNo ratings yet
- German q18 Chronic QuestionnaireDocument5 pagesGerman q18 Chronic Questionnairetobey adityaNo ratings yet
- Needs of Newborn MicroteachingDocument11 pagesNeeds of Newborn MicroteachingAnjali DasNo ratings yet
- The Essential Guide to Prescription Drugs, Update on RemdesivirFrom EverandThe Essential Guide to Prescription Drugs, Update on RemdesivirNo ratings yet
- Elc As590-1 Persuasive SpeechDocument5 pagesElc As590-1 Persuasive SpeechAwiBurhanuddinNo ratings yet
- 1-12 Visit Notes LibrerosDocument5 pages1-12 Visit Notes Libreroskphelps6523No ratings yet
- 1 s2.0 S105913111600011X MainDocument3 pages1 s2.0 S105913111600011X MainNicolas LondoñoNo ratings yet
- Titt El: R/MentDocument3 pagesTitt El: R/MentLakshmidevi.R.M R.MNo ratings yet
- Covid 19Document1 pageCovid 19J GRNo ratings yet
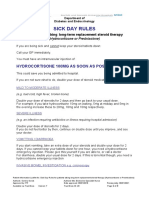
- Sick Day Rules 7.1Document3 pagesSick Day Rules 7.1Neranga SamaratungeNo ratings yet
- Quercetin For Covid19 1196Document2 pagesQuercetin For Covid19 1196Diego SantanaNo ratings yet
- Health Screening Form Burhan Ullah KhanDocument1 pageHealth Screening Form Burhan Ullah KhanFareed KhanNo ratings yet
- KardexDocument2 pagesKardexkimtalaNo ratings yet
- Heart Attacks Reported Following Covid VaccineDocument64 pagesHeart Attacks Reported Following Covid VaccineJosh SingerNo ratings yet
- MX Protocol Book FinalDocument42 pagesMX Protocol Book FinalPawan ChoudharyNo ratings yet
- COVID-19 Vaccine Info SheetDocument8 pagesCOVID-19 Vaccine Info SheetShabin ShabiNo ratings yet
- Case Study 3 CancerDocument4 pagesCase Study 3 Cancerhoneylemon.coNo ratings yet
- SP Checklist: Institute Name Case NameDocument6 pagesSP Checklist: Institute Name Case Namexx_caligurl_93xxNo ratings yet
- WB Covid Protocol Book 25.09 .20 (1)Document49 pagesWB Covid Protocol Book 25.09 .20 (1)El MirageNo ratings yet
- MoH COVID 19 Protocol - V1.2Document8 pagesMoH COVID 19 Protocol - V1.2Khaled EltoukhyNo ratings yet
- FAQs For Doctors-PEDIADocument11 pagesFAQs For Doctors-PEDIAzzNo ratings yet
- Pre Vaccination Screening FormDocument6 pagesPre Vaccination Screening FormAndre3893No ratings yet
- Pfizer Health Declaration Screening Form Eng June 9 2021Document1 pagePfizer Health Declaration Screening Form Eng June 9 2021Kim GomezNo ratings yet
- Folder #1 Robert Bellarmine Pari b21Document65 pagesFolder #1 Robert Bellarmine Pari b21manideepNo ratings yet
- 3612 DequinaDocument1 page3612 DequinaTirth PatelNo ratings yet
- Medical Cannabinoids in Children and Adolescents: A Systematic ReviewDocument18 pagesMedical Cannabinoids in Children and Adolescents: A Systematic ReviewjosetelhadoNo ratings yet
- PM10 April 2015Document9 pagesPM10 April 2015Jennifer londoño arangoNo ratings yet
- Morning Report: Date: Thursday, 8 April 2021Document3 pagesMorning Report: Date: Thursday, 8 April 2021Firdha RositaNo ratings yet
- Periorbital Cellulitis CA4024v3Document5 pagesPeriorbital Cellulitis CA4024v3John M. HemsworthNo ratings yet
- Home Isolation For Covid Care FinalDocument9 pagesHome Isolation For Covid Care FinalAmy LalringhluaniNo ratings yet
- Msic Consensus Statement: Corticosteroids For Covid-19: 27 January 2021Document4 pagesMsic Consensus Statement: Corticosteroids For Covid-19: 27 January 2021Syed Shahrul Naz SyedNo ratings yet
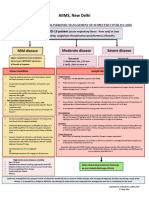
- AIIMS Syndromic ApproachDocument1 pageAIIMS Syndromic ApproachRagul VNo ratings yet
- Graves Pós VacinaDocument3 pagesGraves Pós VacinaViviani ReisNo ratings yet
- Shambom Michael Shee Shiii ShooDocument25 pagesShambom Michael Shee Shiii ShooMichael VladislavNo ratings yet
- Query 1 Modified Systematic ApproachDocument3 pagesQuery 1 Modified Systematic ApproachAntoNo ratings yet
- Treatment and Vaccination For COVID-19Document66 pagesTreatment and Vaccination For COVID-1993612340hkNo ratings yet
- Pharmacy Daily For Fri 07 Apr 2017 - NZ Reconsiders Codeine, FDA Biosimilar Guidance, Inova Bids Below Expectations, Events Calendar and Much MoreDocument3 pagesPharmacy Daily For Fri 07 Apr 2017 - NZ Reconsiders Codeine, FDA Biosimilar Guidance, Inova Bids Below Expectations, Events Calendar and Much MorepharmacydailyNo ratings yet
- Pfizer Under 17 Years Adverse Events Reported To CDCDocument149 pagesPfizer Under 17 Years Adverse Events Reported To CDCWilliam BanksNo ratings yet
- Evidence Check Steroid Use Post COVID 19 VaccinationDocument8 pagesEvidence Check Steroid Use Post COVID 19 Vaccinationbastian fNo ratings yet
- Tetanus Case StudyDocument4 pagesTetanus Case StudyKervy Jay AgraviadorNo ratings yet
- - مستند من D - Bedoor ElgebalyDocument108 pages- مستند من D - Bedoor Elgebalysarah elalfyNo ratings yet
- Summary Antimicrobial Prescribing Guidance - July 21 For BNFDocument31 pagesSummary Antimicrobial Prescribing Guidance - July 21 For BNFbarcanbiancaNo ratings yet
- KRDXDocument3 pagesKRDXMark John Dela CruzNo ratings yet
- COVID-19 AstraZeneca Vaccine AdminDocument13 pagesCOVID-19 AstraZeneca Vaccine AdminKyaw MinNo ratings yet
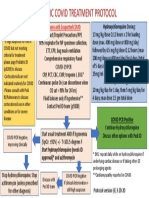
- COVID 19 Pediatric Treatment ProtocolDocument1 pageCOVID 19 Pediatric Treatment ProtocolSahil DhamijaNo ratings yet
- ED Heck: Editorial New Products ReviewDocument24 pagesED Heck: Editorial New Products ReviewEndeNo ratings yet
- TDH Return To School Algorithm Updated 1-5-2021Document1 pageTDH Return To School Algorithm Updated 1-5-2021WVLT NewsNo ratings yet
- COVID-19 Infection Guidelines - Rev4Document16 pagesCOVID-19 Infection Guidelines - Rev4Joshua HobsonNo ratings yet
- COVID-19 PKPD Treatment VietnamDocument27 pagesCOVID-19 PKPD Treatment VietnamNhanLiNo ratings yet
- An Approach To Treating Long COVID: First Line TherapiesDocument3 pagesAn Approach To Treating Long COVID: First Line TherapiesflorentinaNo ratings yet
- Screening QuestionnaireDocument2 pagesScreening QuestionnaireKarina RojasNo ratings yet
- Cannafest 2012 - Medical Cannabis in Israel v6Document39 pagesCannafest 2012 - Medical Cannabis in Israel v6cannajoyNo ratings yet
- FLCCC Ivermectin in The Prophylaxis and Treatment of COVID 19Document22 pagesFLCCC Ivermectin in The Prophylaxis and Treatment of COVID 19Juan Carlos Kuan HigueraNo ratings yet
- Kiss Covid VaccinationsDocument4 pagesKiss Covid VaccinationsMohamed Ali KalathingalNo ratings yet
- Serum Institute of India's Fact Sheet For Recipients of Covishield VaccineDocument2 pagesSerum Institute of India's Fact Sheet For Recipients of Covishield VaccineNDTV100% (2)
- 2002 Guidelines For The Use of Antimicrobial Agents in Neutropenic Patients With CancerDocument23 pages2002 Guidelines For The Use of Antimicrobial Agents in Neutropenic Patients With CancerzuricatitaNo ratings yet
- Moderna (Health Declaration Screening Form) Eng - June 18 2021Document1 pageModerna (Health Declaration Screening Form) Eng - June 18 2021Paulo Justin Tabangcora OropillaNo ratings yet
- The Vaccine Adverse Event Reporting System (VAERS)Document40 pagesThe Vaccine Adverse Event Reporting System (VAERS)Kraft DinnerNo ratings yet
- Clinical Translational Sci - 2022 - Arnold - The Safety and Efficacy of Low Oral Doses of Cannabidiol An Evaluation of TheDocument21 pagesClinical Translational Sci - 2022 - Arnold - The Safety and Efficacy of Low Oral Doses of Cannabidiol An Evaluation of TheDanielNo ratings yet
- A Comparison of Methylprednisolone and Dexamethasone in Intensive Care Patients With COVID-19Document22 pagesA Comparison of Methylprednisolone and Dexamethasone in Intensive Care Patients With COVID-19SupriNo ratings yet
- Model SOP Transfer Item Clarification2 TransferDocument2 pagesModel SOP Transfer Item Clarification2 TransfersrdsteseeNo ratings yet
- Corrigendum Slip No 2 121218Document4 pagesCorrigendum Slip No 2 121218srdsteseeNo ratings yet
- Corrigendum Slip No 1 To Model SOP 2018Document6 pagesCorrigendum Slip No 1 To Model SOP 2018srdsteseeNo ratings yet
- East Central RailwayDocument84 pagesEast Central RailwaysrdsteseeNo ratings yet
- Press Note Modification 7CPC Pensioners04052017Document4 pagesPress Note Modification 7CPC Pensioners04052017srdsteseeNo ratings yet
- Text Books VIMPDocument102 pagesText Books VIMPHarsh ParekhNo ratings yet
- Epidemiology ConceptDocument22 pagesEpidemiology ConceptRezha Hardian RNo ratings yet
- The Aksys Personal Hemodialysis SystemDocument3 pagesThe Aksys Personal Hemodialysis SystemNatik Bi IllahNo ratings yet
- IV Therapy ChecklistDocument3 pagesIV Therapy ChecklistJestoni SalvadorNo ratings yet
- Breastfeeding Promotion by Breastfeeding Promotion Group Kerala University of Health Sciences Kerala IndiaDocument7 pagesBreastfeeding Promotion by Breastfeeding Promotion Group Kerala University of Health Sciences Kerala Indiamrs raamNo ratings yet
- Colposcopy: Cervical Cancer Is Cancer of The Cervix (Lowermost Opening of The Uterus in TheDocument4 pagesColposcopy: Cervical Cancer Is Cancer of The Cervix (Lowermost Opening of The Uterus in TheMayuri SwamiNo ratings yet
- ENT Hospital in Kolhapur - ENT Specialist in Kolhapur - Ishan HospitalDocument9 pagesENT Hospital in Kolhapur - ENT Specialist in Kolhapur - Ishan HospitalChetan GhorpadeNo ratings yet
- Online CLOLAR Clofarabine Purchase With DiscountDocument4 pagesOnline CLOLAR Clofarabine Purchase With Discountcena heyNo ratings yet
- Glister Company LTD: Management StructureDocument6 pagesGlister Company LTD: Management StructureGirish P MehtaNo ratings yet
- Measles: The New Red Scare: by Oman YstrianykDocument20 pagesMeasles: The New Red Scare: by Oman YstrianykManuel AlbaNo ratings yet
- Subjective:: Assessment Nursing Diagnosis Planning Interventi ONS Rationale EvaluationDocument2 pagesSubjective:: Assessment Nursing Diagnosis Planning Interventi ONS Rationale EvaluationCuttie Anne GalangNo ratings yet
- Labour and Delivery 2019Document28 pagesLabour and Delivery 2019Heti PrastiwiningsihNo ratings yet
- Reading Skill Topic: Baby Blues: WorksheetDocument5 pagesReading Skill Topic: Baby Blues: WorksheetFaizatul AzimahNo ratings yet
- USAID Unsolicited ProposalDocument5 pagesUSAID Unsolicited Proposalthamiz nilaNo ratings yet
- Rome Alexander Culaton - Infomercial About Prevention Control of Substance Use Abuse Develop Resistance SkillsDocument2 pagesRome Alexander Culaton - Infomercial About Prevention Control of Substance Use Abuse Develop Resistance Skills레이reiNo ratings yet
- Hand InfectionsDocument30 pagesHand Infectionsvinayguru82No ratings yet
- Music Therapy in Dentistry: Its Application in Management of Anxious Dental Patients - Indian Journal of ResearchDocument2 pagesMusic Therapy in Dentistry: Its Application in Management of Anxious Dental Patients - Indian Journal of ResearchHindol DasNo ratings yet
- Anxiety - A Cancer of The Mind - Aneysha Bhat - TEDxUIUC - EnglishDocument14 pagesAnxiety - A Cancer of The Mind - Aneysha Bhat - TEDxUIUC - EnglishskullabyNo ratings yet
- Theories of Ageing: DR Prema BalusamyDocument19 pagesTheories of Ageing: DR Prema Balusamyprema balusamyNo ratings yet
- Health Litrecy ToolkitDocument227 pagesHealth Litrecy ToolkitAnonymous ibmeej9No ratings yet
- Traveller GreeceDocument2 pagesTraveller GreeceElefteriosNo ratings yet