You might also like
- 011 Leave Application FormDocument1 page011 Leave Application FormSolehah OthmanNo ratings yet
- Leave Application FormDocument2 pagesLeave Application FormPurchase DeptNo ratings yet
- Leave FormDocument1 pageLeave FormBlitzkrieg ZNo ratings yet
- FORM 6 - BlankDocument3 pagesFORM 6 - BlankmisomarjorieNo ratings yet
- Application of Leave CSC Form No. 6 : Revised 1985Document7 pagesApplication of Leave CSC Form No. 6 : Revised 1985Cherry Mae Morales BandijaNo ratings yet
- Request For LeaveDocument1 pageRequest For LeaveJanine O'shea DoloresNo ratings yet
- CLFORMDocument3 pagesCLFORMleaf856231No ratings yet
- Format Cuti PerusahaanDocument5 pagesFormat Cuti Perusahaanamelia sakinahNo ratings yet
- To Ensure That You Are Settled On Time, Please Adhere To The Following Guidelines When Submitting Your Timesheet Relating TheretoDocument2 pagesTo Ensure That You Are Settled On Time, Please Adhere To The Following Guidelines When Submitting Your Timesheet Relating TheretoHennyWAstutiNo ratings yet
- Leave Form 6 NewDocument2 pagesLeave Form 6 NewROMELYN A. ESTOMATANo ratings yet
- Application For Leave: Republic of The PhilippinesDocument3 pagesApplication For Leave: Republic of The PhilippinesEva MaeNo ratings yet
- Medical and Earn Leave Letter NewDocument2 pagesMedical and Earn Leave Letter Newusiaf007No ratings yet
- CSC - FORM - NO - 6-Revised-2020-DEPED-MISOR-FIELD-2-1Document2 pagesCSC - FORM - NO - 6-Revised-2020-DEPED-MISOR-FIELD-2-1Gizellen GuiboneNo ratings yet
- Leave Application Form (Masud Karim Khan) UpdatDocument1 pageLeave Application Form (Masud Karim Khan) UpdatSECBD 2023No ratings yet
- E. L.Document5 pagesE. L.tarunsharmasujokNo ratings yet
- Department of Education: Application For LeaveDocument2 pagesDepartment of Education: Application For LeaveJocelyn BuslotanNo ratings yet
- Application For Leave 2. NAME: (Last) (First) (Middle) : 3. Date of Filing 4. Position Teacher I 5. SalaryDocument2 pagesApplication For Leave 2. NAME: (Last) (First) (Middle) : 3. Date of Filing 4. Position Teacher I 5. SalaryRejane Haro Ganuhay TorillaNo ratings yet
- Newform 6Document14 pagesNewform 6maniquezcarenNo ratings yet
- Form 6 Below 60 DaysDocument2 pagesForm 6 Below 60 DaysRegine Rave Ria IgnacioNo ratings yet
- Blank Application For LeaveDocument2 pagesBlank Application For Leavelumayadjust12No ratings yet
- CSC FORM 6 North Teaching and Non Teaching 20 To 60 CALENDAR DAYSDocument2 pagesCSC FORM 6 North Teaching and Non Teaching 20 To 60 CALENDAR DAYSSyra CantoNo ratings yet
- Leave Application FormatDocument1 pageLeave Application FormatdeobittuvermaNo ratings yet
- Leave Application FormDocument1 pageLeave Application FormHalifi MuhamadNo ratings yet
- Leave FormDocument1 pageLeave FormJoy Pelagio BuenoNo ratings yet
- Philippine Span Asia Carrier Corp.: From RF14 Engineering Dept. DateDocument10 pagesPhilippine Span Asia Carrier Corp.: From RF14 Engineering Dept. DateJezrell JaravataNo ratings yet
- CSC FORM 6 North TEACHING 19 DAYS AND BELOWDocument2 pagesCSC FORM 6 North TEACHING 19 DAYS AND BELOWCyrenz Jean PantonialNo ratings yet
- 2021 Form 6 NewDocument1 page2021 Form 6 NewCiscy TorcinoNo ratings yet
- Leave FormDocument5 pagesLeave FormMariecriz Balaba BanaezNo ratings yet
- Leave Application Form (Annexure-VI)Document1 pageLeave Application Form (Annexure-VI)Mohit SharmaNo ratings yet
- New Leave Form Form 6Document2 pagesNew Leave Form Form 6Sheila Bliss Goc-ongNo ratings yet
- Leave Revised 2020Document2 pagesLeave Revised 2020Butch NorielNo ratings yet
- EDR 16 Leave W Out PayDocument2 pagesEDR 16 Leave W Out PayDonnie SalazarNo ratings yet
- Fitbase Cancellation FormDocument1 pageFitbase Cancellation FormMarley HarrisNo ratings yet
- ClearanceDocument1 pageClearancehumacadeyt12No ratings yet
- Checklist For The Application of Repair - Repainting PermitDocument1 pageChecklist For The Application of Repair - Repainting PermitTimothy John DicheNo ratings yet
- DL JodhpurDocument1 pageDL JodhpursantoshaiimsNo ratings yet
- Cash AdvanceDocument2 pagesCash Advancegreenapple015100% (1)
- Form 6Document2 pagesForm 6Jasper Lynne VillanuevaNo ratings yet
- Leave Form NewDocument1 pageLeave Form NewPia Mae GregorioNo ratings yet
- Leave Revised 2020Document2 pagesLeave Revised 2020Jessica BelisarioNo ratings yet
- Leave Form: Total Days of Leave or Absence FROM (Month, Day, Year) UNTIL (Month, Day, Year)Document1 pageLeave Form: Total Days of Leave or Absence FROM (Month, Day, Year) UNTIL (Month, Day, Year)shayne rosanes100% (1)
- Application For Leave: Deped - Gigaquit Lasicam-Perral Nhs - 6. Details of ApplicationDocument4 pagesApplication For Leave: Deped - Gigaquit Lasicam-Perral Nhs - 6. Details of ApplicationAlfie LumpayNo ratings yet
- CS Form 6Document2 pagesCS Form 6Fidel AbellanaNo ratings yet
- FORM 6 BlankDocument2 pagesFORM 6 Blankrieza camanchoNo ratings yet
- Job Application Form For AssistantDocument4 pagesJob Application Form For AssistantabsamNo ratings yet
- Leave Application: Type of Leave (Put Tick Mark in Appropriate Colum)Document1 pageLeave Application: Type of Leave (Put Tick Mark in Appropriate Colum)santosh meenaNo ratings yet
- Leave Application New FormDocument1 pageLeave Application New FormNathaniel Gutierez MangubatNo ratings yet
- Application Form For Earned Leave or Extension of LeaveDocument1 pageApplication Form For Earned Leave or Extension of LeaveTia Moore0% (1)
- Leave Form Revised 2021 TeachingDocument2 pagesLeave Form Revised 2021 TeachingRosalie Sison100% (1)
- Application For Leave: CSC Form No. (Revised 1985)Document3 pagesApplication For Leave: CSC Form No. (Revised 1985)Jereille GayasoNo ratings yet
- Application For Leave of Absence (Afloa) : Check The Appropriate BoxesDocument1 pageApplication For Leave of Absence (Afloa) : Check The Appropriate BoxesFelix Jr CojenNo ratings yet
- COPY Leave FormDocument1 pageCOPY Leave Formg5.spsbbg1No ratings yet
- Leave-Revised-2020 - Marivi CaparosoDocument17 pagesLeave-Revised-2020 - Marivi CaparosoLea Mae ArintokNo ratings yet
- CS Form 6 NewDocument2 pagesCS Form 6 NewMICHAEL ANGELO MAYORDONo ratings yet
- Application For Leave CSC Form 6 New 2024Document8 pagesApplication For Leave CSC Form 6 New 2024GLADYS SARAELNo ratings yet
- Form 6 TemplateDocument3 pagesForm 6 TemplateZoe R. CaneNo ratings yet
- AAL Leave FormDocument1 pageAAL Leave FormDlone ZhuangNo ratings yet
- Application For Leave: Republic of The PhilippinesDocument2 pagesApplication For Leave: Republic of The PhilippinesRey Mark OrdillanoNo ratings yet
- Leave FormDocument7 pagesLeave FormCasey Del Gallego EnrileNo ratings yet
- Muniba NaseemDocument2 pagesMuniba NaseemMuniba NasimNo ratings yet
- Staff Asst Sponsorship FormDocument1 pageStaff Asst Sponsorship FormMuniba NasimNo ratings yet
- Fee Structure 2021-22Document1 pageFee Structure 2021-22Muniba NasimNo ratings yet
- Doacs Final PPT-2Document23 pagesDoacs Final PPT-2Muniba NasimNo ratings yet
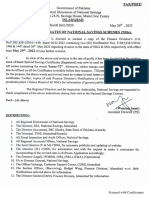
- 2023 - 05 - 26 Revision in Rates of NSSDocument4 pages2023 - 05 - 26 Revision in Rates of NSSMuniba NasimNo ratings yet
- IDSA and CPE CertificateDocument3 pagesIDSA and CPE CertificateMuniba NasimNo ratings yet
- High Alert Peads DosingDocument2 pagesHigh Alert Peads DosingMuniba NasimNo ratings yet
- ACC List of High and Middle Low Income CountriesDocument5 pagesACC List of High and Middle Low Income CountriesMuniba NasimNo ratings yet
- Insulin Guide (Type, Route, Dose)Document1 pageInsulin Guide (Type, Route, Dose)Muniba NasimNo ratings yet
- CA ALA C11b Isotonic Solutions 1Document1 pageCA ALA C11b Isotonic Solutions 1Muniba NasimNo ratings yet
- 6 Days Skardu CorollaDocument4 pages6 Days Skardu CorollaMuniba NasimNo ratings yet
- CAP ManagementDocument1 pageCAP ManagementMuniba NasimNo ratings yet
- DubaiDocument3 pagesDubaiMuniba NasimNo ratings yet
- Medication Refill ProcessDocument1 pageMedication Refill ProcessMuniba NasimNo ratings yet
- ColistinDocument1 pageColistinMuniba NasimNo ratings yet
- Anticoagulation OverviewDocument62 pagesAnticoagulation OverviewMuniba NasimNo ratings yet