You might also like
- SECURITIES INDUSTRY ESSENTIALS EXAM STUDY GUIDE 2021 + TEST BANKFrom EverandSECURITIES INDUSTRY ESSENTIALS EXAM STUDY GUIDE 2021 + TEST BANKRating: 5 out of 5 stars5/5 (1)
- Cellular ManufacturingDocument61 pagesCellular Manufacturingapi-3852736100% (1)
- Unit DNI Candidate Guidance v51612018191423Document14 pagesUnit DNI Candidate Guidance v51612018191423Carla Baraybar100% (1)
- FREE BioGeometry Emitter PhotoDocument5 pagesFREE BioGeometry Emitter PhotoNisha Joshi75% (8)
- Carbon TaxDocument24 pagesCarbon Taxasofos100% (1)
- SIP Registation Form-With One Time MandateDocument4 pagesSIP Registation Form-With One Time MandatePrince ANo ratings yet
- TATA NACH FORM (5)Document1 pageTATA NACH FORM (5)vanshjainNo ratings yet
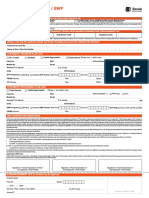
- Sip Registration / Renewal Form: Debit Mandate Form Nach (One Time Mandate - Otm)Document1 pageSip Registration / Renewal Form: Debit Mandate Form Nach (One Time Mandate - Otm)Sanjay PatilNo ratings yet
- Sip Enrollment DetailsDocument2 pagesSip Enrollment DetailsDBCGNo ratings yet
- Sole / First Applicant Second Applicant Third ApplicantDocument2 pagesSole / First Applicant Second Applicant Third ApplicantAnkur KaushikNo ratings yet
- One Time Mandate Registration Form/ Debit Mandate Form NACH/ ECS/ Direct DebitDocument2 pagesOne Time Mandate Registration Form/ Debit Mandate Form NACH/ ECS/ Direct DebitAnand KopareNo ratings yet
- Sip Registration Cum Mandate Form: For Investment Through NACH/Direct DebitDocument2 pagesSip Registration Cum Mandate Form: For Investment Through NACH/Direct DebitAbhijit patraNo ratings yet
- PAN BASED NACH MANDATE CUM SIP REGISTRATIONDocument2 pagesPAN BASED NACH MANDATE CUM SIP REGISTRATIONDevesh SinghNo ratings yet
- Unit Holder Information: Web FormDocument2 pagesUnit Holder Information: Web FormDibyaranjan SahooNo ratings yet
- Birla SIP Cum NACH FormDocument6 pagesBirla SIP Cum NACH FormarunimaapkNo ratings yet
- Application Form For Existing Investors: My DetailsDocument8 pagesApplication Form For Existing Investors: My Detailsvikas9saraswatNo ratings yet
- Jm Finance Mf_sip NachDocument1 pageJm Finance Mf_sip NacharunimaapkNo ratings yet
- SIP1018 Kotak - CDRDocument1 pageSIP1018 Kotak - CDRNikesh MewaraNo ratings yet
- Sip Cum Nach FormDocument8 pagesSip Cum Nach FormAmit GuptaNo ratings yet
- Sip Multiple FormDocument2 pagesSip Multiple FormAmit SharmaNo ratings yet
- Common Transaction Form Financial Transaction Kk3i5z51Document8 pagesCommon Transaction Form Financial Transaction Kk3i5z51Balraj SinghNo ratings yet
- JM Equity Tax Saver FundDocument4 pagesJM Equity Tax Saver Funddrashti.investments1614No ratings yet
- One Time Debit Mandate Form NACH / Auto Debit: Mutual FundsDocument2 pagesOne Time Debit Mandate Form NACH / Auto Debit: Mutual FundsNothing NothingNo ratings yet
- Baroda BNP Paribas SIP Form 127Document2 pagesBaroda BNP Paribas SIP Form 127custodian.archiveNo ratings yet
- SLF017 ShortTermLoanRemittanceForm V02Document2 pagesSLF017 ShortTermLoanRemittanceForm V02Marites Paragua75% (4)
- Tata - Transaction Slip-NO CODEDocument1 pageTata - Transaction Slip-NO CODEsudeshna palitNo ratings yet
- Family Solutions Transaction FormDocument2 pagesFamily Solutions Transaction FormSelva KumarNo ratings yet
- HDFC Sip Nach FormDocument6 pagesHDFC Sip Nach FormPraveen KumarNo ratings yet
- Existing Investor'S Folio Number Unit Holding Options: Transaction Charges ORDocument4 pagesExisting Investor'S Folio Number Unit Holding Options: Transaction Charges ORraj tripathiNo ratings yet
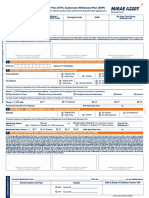
- Application Form: Systematic Transfer Plan (STP), Systematic Withdrawal Plan (SWP)Document2 pagesApplication Form: Systematic Transfer Plan (STP), Systematic Withdrawal Plan (SWP)Gargi ShuklaNo ratings yet
- Common Application Form: For Holding Units in Demat ModeDocument6 pagesCommon Application Form: For Holding Units in Demat ModevasucristalNo ratings yet
- Transaction Form For Financial Transactions - CL04059Document4 pagesTransaction Form For Financial Transactions - CL04059Professional positiveNo ratings yet
- STP and SWP Form May17 FillPrintDocument2 pagesSTP and SWP Form May17 FillPrintRohan KapoorNo ratings yet
- Sip Enrolment FormDocument1 pageSip Enrolment FormYankit SoniNo ratings yet
- Short-Term Loan Remittance Form (STLRF) : HQP-SLF-017Document2 pagesShort-Term Loan Remittance Form (STLRF) : HQP-SLF-017Jo Sh100% (1)
- Application Form: Systematic Transfer Plan (STP), Systematic Withdrawal Plan (SWP)Document2 pagesApplication Form: Systematic Transfer Plan (STP), Systematic Withdrawal Plan (SWP)Chintan JainNo ratings yet
- SIP Auto Debit Form 2011Document4 pagesSIP Auto Debit Form 2011Anirudha MohapatraNo ratings yet
- Micro SIP Auto Debit 140110Document2 pagesMicro SIP Auto Debit 140110Harneet SinghNo ratings yet
- SIP Application FormDocument3 pagesSIP Application FormspeedenquiryNo ratings yet
- SIP & SIP Top-up Registration FormDocument1 pageSIP & SIP Top-up Registration Formraj tripathiNo ratings yet
- Mirae SIP FormDocument5 pagesMirae SIP FormdurgeshNo ratings yet
- Trade Ticket FormDocument2 pagesTrade Ticket FormRenee Barian RomeroNo ratings yet
- HDFC Retirement Savings Fund: First/ Sole Applicant/ Guardian Third Applicant Second ApplicantDocument7 pagesHDFC Retirement Savings Fund: First/ Sole Applicant/ Guardian Third Applicant Second ApplicantAltamash FaridNo ratings yet
- Application Form For Sip & Flex SipDocument3 pagesApplication Form For Sip & Flex SipNikesh MewaraNo ratings yet
- Application Form STP / SWP: Distributor InformationDocument1 pageApplication Form STP / SWP: Distributor InformationSatya Prakash TrivediNo ratings yet
- Equity SIP Application Form April 2022Document8 pagesEquity SIP Application Form April 2022Selva KumarNo ratings yet
- AXIS-New Common Application Form 2023 1Document4 pagesAXIS-New Common Application Form 2023 1Brahmbhatt ConsultancyNo ratings yet
- Mirae Sip FormDocument2 pagesMirae Sip Formitkahs120No ratings yet
- Power Finance Corporation LTDDocument4 pagesPower Finance Corporation LTDAritra BhattacharjeeNo ratings yet
- Scan1 PDFDocument2 pagesScan1 PDFshaumyaNo ratings yet
- NFO Form - Edelweiss Focused Equity SchemeDocument3 pagesNFO Form - Edelweiss Focused Equity SchemeAvinashNo ratings yet
- Systematic Investment Plan (SIP) / Micro SIP Form: 1. Applicant InformationDocument2 pagesSystematic Investment Plan (SIP) / Micro SIP Form: 1. Applicant InformationAnonymous MAQrYFQDzVNo ratings yet
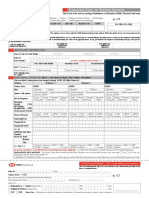
- Common Application FormDocument5 pagesCommon Application FormNeeraj KumarNo ratings yet
- Transaction Form For Existing InvestorsDocument4 pagesTransaction Form For Existing InvestorsRRKNo ratings yet
- Apply for Samco Mutual FundDocument4 pagesApply for Samco Mutual FundRavindraNo ratings yet
- Axis CTF FillableDocument1 pageAxis CTF FillablemayankNo ratings yet
- SIP Form DebtDocument6 pagesSIP Form DebtNilesh MahajanNo ratings yet
- Common Transaction SlipDocument3 pagesCommon Transaction Slipabdriver2000No ratings yet
- SBI SIP Registration FormDocument3 pagesSBI SIP Registration FormPrakash JoshiNo ratings yet
- 22 Common Application Form Invesco - HTMLDocument3 pages22 Common Application Form Invesco - HTMLyogeshmongiayahoo.comNo ratings yet
- L&T Mutual Fund Application FormDocument5 pagesL&T Mutual Fund Application FormnanduvermaNo ratings yet
- SIP Facility Appl Form V 1Document4 pagesSIP Facility Appl Form V 1DBCGNo ratings yet
- Av Birla Sip FormDocument1 pageAv Birla Sip FormVikas RaiNo ratings yet
- Sip Pause Form: (For Investment Through ECS (Debit Clearing) /direct Debit Facility /standing Instruction/NACH)Document2 pagesSip Pause Form: (For Investment Through ECS (Debit Clearing) /direct Debit Facility /standing Instruction/NACH)SANJEEV SANGAINo ratings yet
- Syllabus For ETABSDocument2 pagesSyllabus For ETABSSandgrouse RajNo ratings yet
- Selected Questions Revised 20200305 2HRDocument3 pagesSelected Questions Revised 20200305 2HRTimmy LeeNo ratings yet
- 2018-03-23 Tier 25 Register of SponsorsDocument1,910 pages2018-03-23 Tier 25 Register of SponsorsAnonymous TjeiW5No ratings yet
- Title of Training Presentation: Presented by Your NameDocument14 pagesTitle of Training Presentation: Presented by Your NameJudy UnreinNo ratings yet
- Insurance - Unit 3&4Document20 pagesInsurance - Unit 3&4Dhruv GandhiNo ratings yet
- ENGG378 - 948 HydroPower-Lecture - 1 - 2019 PDFDocument34 pagesENGG378 - 948 HydroPower-Lecture - 1 - 2019 PDFJ CNo ratings yet
- Assessment Rubric Coach Manual Oct 11 - FinalDocument9 pagesAssessment Rubric Coach Manual Oct 11 - Finalapi-246218373No ratings yet
- 1 A Simulation Based Model For The BerthDocument9 pages1 A Simulation Based Model For The Berthmonu_vitsNo ratings yet
- DQFAQsDocument8 pagesDQFAQsBhagyashree kawaleNo ratings yet
- Lubricated Coupling TrainingDocument47 pagesLubricated Coupling TrainingTheerayootNo ratings yet
- Fire and Ice by Robert FrostDocument2 pagesFire and Ice by Robert Frostapi-561976496No ratings yet
- Iron Deficiency Anemia in ChildrenDocument27 pagesIron Deficiency Anemia in ChildrenAde Dinda WulandariNo ratings yet
- Master Gardener Home Vegetable Guide: Chapter 1 - Gardening BasicsDocument30 pagesMaster Gardener Home Vegetable Guide: Chapter 1 - Gardening BasicsAmr M. SaidNo ratings yet
- 5.1 Quadratic Functions: 344 Learning ObjectivesDocument15 pages5.1 Quadratic Functions: 344 Learning ObjectiveskhadijaNo ratings yet
- Bamuoingaythienquan NguyenduynhienDocument9 pagesBamuoingaythienquan NguyenduynhienFLed NguyenNo ratings yet
- Domain Logic and SQLDocument23 pagesDomain Logic and SQLatifchaudhryNo ratings yet
- Chapter OneDocument36 pagesChapter Onepretoria agreement21No ratings yet
- CancioneroDocument7 pagesCancioneroJocelyn Almaguer LariosNo ratings yet
- UNI National Education Advances EnglishDocument6 pagesUNI National Education Advances EnglishJose BancesNo ratings yet
- 2020 FMGT 1013 - Financial Management RevisedDocument9 pages2020 FMGT 1013 - Financial Management RevisedYANIII12345No ratings yet
- ECT ModelDocument12 pagesECT Modelhii_bhartiNo ratings yet
- Centered Nursing Process Approach (9th Ed.) - St. Louis, MO: ElsevierDocument1 pageCentered Nursing Process Approach (9th Ed.) - St. Louis, MO: ElsevierfaizaNo ratings yet
- Lippo Karawaci Review 30 September 2019 FINAL PDFDocument149 pagesLippo Karawaci Review 30 September 2019 FINAL PDFAndy AghastaNo ratings yet
- VKS INFRA DPR Submission for NHAI Bihar ProjectDocument1 pageVKS INFRA DPR Submission for NHAI Bihar ProjectamirNo ratings yet
- Letter of RecommendationDocument2 pagesLetter of RecommendationnaveenNo ratings yet
- Reedisha Spinning LTD - Industrial ReportDocument112 pagesReedisha Spinning LTD - Industrial ReportShuvashish Chakma100% (4)