You might also like
- Studio Ghibli Beginner Piano BookDocument192 pagesStudio Ghibli Beginner Piano BookAidan Coffey94% (16)
- Studio Ghibli Beginner Piano BookDocument192 pagesStudio Ghibli Beginner Piano BookAidan Coffey94% (16)
- Studio Ghibli Beginner Piano BookDocument192 pagesStudio Ghibli Beginner Piano BookAidan Coffey94% (16)
- USMLE Images For The BoardsDocument297 pagesUSMLE Images For The BoardsMulham Etki100% (3)
- Aap 2009Document538 pagesAap 2009toniassaf100% (1)
- Caries Risk AssessmentDocument33 pagesCaries Risk AssessmentSomya Jain100% (1)
- Schizophrenia Case StudyDocument14 pagesSchizophrenia Case Studyapi-593859653No ratings yet
- World Congress Integrative Medicine & Health 2017: Part TwoDocument65 pagesWorld Congress Integrative Medicine & Health 2017: Part TwoGabrielAbarcaNo ratings yet
- My Neighbor TotoroDocument7 pagesMy Neighbor TotoroPaul NguyenNo ratings yet
- Acupuncture For Children With Autism Spectrum DisorderDocument3 pagesAcupuncture For Children With Autism Spectrum DisorderPaul NguyenNo ratings yet
- Lymphedema BrochureDocument8 pagesLymphedema BrochureJose MiaNo ratings yet
- Health Teaching Plan: Learning Objectives Content Strategy Strategy Rationale Time Venue Date Resources EvaluationDocument4 pagesHealth Teaching Plan: Learning Objectives Content Strategy Strategy Rationale Time Venue Date Resources EvaluationMae EstilloreNo ratings yet
- Integrative Cancer Therapies: The Impact of Healing Touch On Pediatric Oncology PatientsDocument7 pagesIntegrative Cancer Therapies: The Impact of Healing Touch On Pediatric Oncology PatientsAlina GheNo ratings yet
- Use of and Attitudes Toward Complementary and Alternative Medicine Among Nurse-Midwives in IsraelDocument7 pagesUse of and Attitudes Toward Complementary and Alternative Medicine Among Nurse-Midwives in IsraelEndahNo ratings yet
- Dietary Supplement Use in Ambulatory Cancer Patients: A Survey On Prevalence, Motivation and AttitudesDocument9 pagesDietary Supplement Use in Ambulatory Cancer Patients: A Survey On Prevalence, Motivation and AttitudespilarerasoNo ratings yet
- Journal Club: Dr. Md. Tanvir AhammedDocument20 pagesJournal Club: Dr. Md. Tanvir AhammedTanvir AhammedNo ratings yet
- Stiripentol in Severe Myoclonic Epilepsy in Infancy: A Randomised Placebo-Controlled Syndrome-Dedicated TrialDocument5 pagesStiripentol in Severe Myoclonic Epilepsy in Infancy: A Randomised Placebo-Controlled Syndrome-Dedicated TrialRaisa ZnNo ratings yet
- High Usage of Complementary and Alternative Medicine Among Turkish Asthmatic ChildrenDocument6 pagesHigh Usage of Complementary and Alternative Medicine Among Turkish Asthmatic Childrensri suryaningsihNo ratings yet
- Supportive Care in Pediatric Oncology: A Practical Evidence-Based ApproachFrom EverandSupportive Care in Pediatric Oncology: A Practical Evidence-Based ApproachJames H. FeusnerNo ratings yet
- Use of Alternative - Complementary-Medicine (CAM) in Calabrian ChildrenDocument6 pagesUse of Alternative - Complementary-Medicine (CAM) in Calabrian ChildrenaimansajjadNo ratings yet
- Parenting in The Face of Serious Illness Childhood Cancer - 2019Document9 pagesParenting in The Face of Serious Illness Childhood Cancer - 2019AnaBMonteiroNo ratings yet
- CAM Methods Used by Pediatric Cancer PatientsDocument24 pagesCAM Methods Used by Pediatric Cancer PatientsErwan AutretNo ratings yet
- Jurnal Ca KulitDocument10 pagesJurnal Ca Kulitilham darnoNo ratings yet
- Knowledge, Attitudes and Practice Survey About Antimicrobial Resistance and Prescribing Among Physicians in A Hospital Setting in Lima, PeruDocument8 pagesKnowledge, Attitudes and Practice Survey About Antimicrobial Resistance and Prescribing Among Physicians in A Hospital Setting in Lima, PeruShiuMan LimNo ratings yet
- SIOP22 - EPoster ViewingDocument1,855 pagesSIOP22 - EPoster ViewingmgNo ratings yet
- HERO Results From The HERO Study - Treatment-Related Characteristics of The PopulationDocument14 pagesHERO Results From The HERO Study - Treatment-Related Characteristics of The PopulationLaboriusNo ratings yet
- Dan - Patinet ReluctanceDocument6 pagesDan - Patinet Reluctanceamandeep khuranaNo ratings yet
- Dawczak Debicka 2022 Complementary and Alternative TheraDocument15 pagesDawczak Debicka 2022 Complementary and Alternative Therabisak.j.adelaNo ratings yet
- BMC Complementary and Alternative MedicineDocument8 pagesBMC Complementary and Alternative MedicineudupisonyNo ratings yet
- Research Article: Self-Medication in University Students From The City of Mansoura, EgyptDocument7 pagesResearch Article: Self-Medication in University Students From The City of Mansoura, EgyptyunitakajahNo ratings yet
- Research TopicsDocument7 pagesResearch TopicsWillium ThomasNo ratings yet
- 2017 - BABY BLUESDocument2 pages2017 - BABY BLUESPatrícia BodoniNo ratings yet
- Knowledge, Attitudes, and Acceptability of A Human Papillomavirus Vaccine Among Healthcare ProvidersDocument9 pagesKnowledge, Attitudes, and Acceptability of A Human Papillomavirus Vaccine Among Healthcare ProvidersannisaNo ratings yet
- HOMEOPATHYANDCANCERDocument6 pagesHOMEOPATHYANDCANCERAshok Sinha100% (1)
- Validating the Children’s Medicines Use Questionnaire in AustraliaDocument9 pagesValidating the Children’s Medicines Use Questionnaire in AustraliadidiNo ratings yet
- SDOM Promising TherapiesDocument16 pagesSDOM Promising TherapiesdarlingcarvajalduqueNo ratings yet
- Angelina Alphonce JohoDocument80 pagesAngelina Alphonce JohoMerlina WijayawatiNo ratings yet
- Patient Reported BarriesDocument14 pagesPatient Reported Barriesdani catriaNo ratings yet
- Introduction To Complementary Alternative and Trad PDFDocument10 pagesIntroduction To Complementary Alternative and Trad PDFAazie ZonaNo ratings yet
- Use of Micronutrients and Alternative Drugs by Children With Acute Lymphoblastic LeukemiaDocument4 pagesUse of Micronutrients and Alternative Drugs by Children With Acute Lymphoblastic LeukemiaionaiobidzeNo ratings yet
- Predicting Adherence To Antiretroviral Therapy Among Pregnant Women in Guyana: Utility of The Health Belief ModelDocument10 pagesPredicting Adherence To Antiretroviral Therapy Among Pregnant Women in Guyana: Utility of The Health Belief ModelRiska Resty WasitaNo ratings yet
- Factors influencing nutritional status of Kenyan children with cancerDocument18 pagesFactors influencing nutritional status of Kenyan children with cancerpopongNo ratings yet
- tmp27B4 TMPDocument6 pagestmp27B4 TMPFrontiersNo ratings yet
- Patient and Family Engagement During Treatment Change To Emicizumab - 2019 - BloDocument2 pagesPatient and Family Engagement During Treatment Change To Emicizumab - 2019 - BloMichael John AguilarNo ratings yet
- Knowledge, Perceptions and Attitudes Toward Complementary and Alternative Therapies Among Kuwaiti Medical and Pharmacy StudentsDocument5 pagesKnowledge, Perceptions and Attitudes Toward Complementary and Alternative Therapies Among Kuwaiti Medical and Pharmacy StudentsMSshy RPhNo ratings yet
- Accepted Manuscript: Complementary Therapies in Clinical PracticeDocument30 pagesAccepted Manuscript: Complementary Therapies in Clinical PracticeCamilaPazNo ratings yet
- 2018 - Baraki Et AlDocument8 pages2018 - Baraki Et AlazeemathmariyamNo ratings yet
- Ni Hms 574605Document17 pagesNi Hms 574605circe5690No ratings yet
- Homeopathic Preparations For Preventing and Treating Acute Upper Respiratory Tract Infections in Children: A Systematic Review and Meta-AnalysisDocument10 pagesHomeopathic Preparations For Preventing and Treating Acute Upper Respiratory Tract Infections in Children: A Systematic Review and Meta-AnalysisCarlos Arturo Vera VásquezNo ratings yet
- AFP MAY Research Von ConradyDocument10 pagesAFP MAY Research Von Conradychaitanya gNo ratings yet
- Implications of Self-Medication Among Medical Students-A DilemmaDocument6 pagesImplications of Self-Medication Among Medical Students-A Dilemmasky.blueNo ratings yet
- Leblanc 2018Document8 pagesLeblanc 2018Eunice BarrosNo ratings yet
- Palo Ebj 2ndrot PDFDocument7 pagesPalo Ebj 2ndrot PDFAyen PaloNo ratings yet
- JMCP 2023 29 1 58Document11 pagesJMCP 2023 29 1 58Javier Martin Bartolo GarciaNo ratings yet
- Saudi Pharmaceutical JournalDocument5 pagesSaudi Pharmaceutical JournalVictor TabuncicNo ratings yet
- Complementary Cancer CuresDocument15 pagesComplementary Cancer CuresPJ McKennaNo ratings yet
- 1365-Article Text-8141-1-4-20210610Document16 pages1365-Article Text-8141-1-4-20210610Maabena AsanteNo ratings yet
- Does mHealth increase adherence to medication? A systematic reviewDocument24 pagesDoes mHealth increase adherence to medication? A systematic reviewVirgo WNo ratings yet
- ST Gallen 2021 A OncologyDocument20 pagesST Gallen 2021 A OncologyJorge Apolo PinzaNo ratings yet
- Goh2009 PDFDocument10 pagesGoh2009 PDFekaNo ratings yet
- Medicine American Journal of Hospice and PalliativeDocument6 pagesMedicine American Journal of Hospice and Palliativem1k0eNo ratings yet
- Hospitalization For Community-AcquiredDocument10 pagesHospitalization For Community-AcquiredJuwita PratiwiNo ratings yet
- Prevalence and Factors Associated With Self Medication With Antibiotics Among University Students in Moshi Kilimanjaro TanzaniaDocument7 pagesPrevalence and Factors Associated With Self Medication With Antibiotics Among University Students in Moshi Kilimanjaro TanzaniaSamia RoshdyNo ratings yet
- Knowledge attitude and practice on and willingness to pay for human papillomavirus vaccine a cross-sectional study in Hanoi VietnamDocument11 pagesKnowledge attitude and practice on and willingness to pay for human papillomavirus vaccine a cross-sectional study in Hanoi Vietnamk61.2214520016No ratings yet
- Infantile Hypertrophic Pyloric Stenosis at A TertiDocument7 pagesInfantile Hypertrophic Pyloric Stenosis at A TertiVașadi Razvan CristianNo ratings yet
- 2015 Article 516Document12 pages2015 Article 516Mukhtar TarNo ratings yet
- Is There A Role of Homeopathy in CancerDocument7 pagesIs There A Role of Homeopathy in CancerAndrea CastañoNo ratings yet
- Improving Medication Safety: Development and Impact of A Multivariate Model-Based Strategy To Target High-Risk PatientsDocument13 pagesImproving Medication Safety: Development and Impact of A Multivariate Model-Based Strategy To Target High-Risk PatientstotoksaptantoNo ratings yet
- Routine Amoxicillin For Uncomplicated Severe Acute Malnutrition in ChildrenDocument10 pagesRoutine Amoxicillin For Uncomplicated Severe Acute Malnutrition in ChildrenMc'onethree BrownNo ratings yet
- T2DM Treatment Costs in MumbaiDocument2 pagesT2DM Treatment Costs in MumbaiRoxana SlujitoruNo ratings yet
- Xylitol Syrup For The Prevention of Acute Otitis Media: PediatricsDocument9 pagesXylitol Syrup For The Prevention of Acute Otitis Media: PediatricsholaNo ratings yet
- SS1A - Exam 1 Study Guide SP 2015Document7 pagesSS1A - Exam 1 Study Guide SP 2015Paul NguyenNo ratings yet
- Possible Effect of Acupuncture in Autism Spectrum DisorderDocument3 pagesPossible Effect of Acupuncture in Autism Spectrum DisorderPaul NguyenNo ratings yet
- Merry Christmas Mr. LawrenceDocument5 pagesMerry Christmas Mr. LawrencePaul Nguyen100% (1)
- Guide to the history and physical exam for urologic patientsDocument39 pagesGuide to the history and physical exam for urologic patientsNendy OktariNo ratings yet
- Mosquito AuthorityDocument3 pagesMosquito AuthorityWACHNo ratings yet
- TOG 2023 Volume 25 Issue 3Document86 pagesTOG 2023 Volume 25 Issue 3saeed hasan saeedNo ratings yet
- 26 Lessons Learned As A NurseDocument2 pages26 Lessons Learned As A NurseAnthonyBernardoAbustanNo ratings yet
- District Health Profile DaduDocument52 pagesDistrict Health Profile DaduSyedAounRaza100% (1)
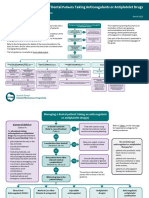
- Sdcep Anticoagulants Quick Reference Guide 2nd EditionDocument5 pagesSdcep Anticoagulants Quick Reference Guide 2nd EditionMeryem LahlouNo ratings yet
- Seminar: Amy K Winter, William J MossDocument11 pagesSeminar: Amy K Winter, William J MossM Dwi Ari NurhidayatNo ratings yet
- Managing Anxiety and Pain in Ovarian CancerDocument5 pagesManaging Anxiety and Pain in Ovarian CancerDanica CumlatNo ratings yet
- Remote Cardiology Consultations Using Advanced Medical TechnologyDocument193 pagesRemote Cardiology Consultations Using Advanced Medical TechnologywholenumberNo ratings yet
- Periodontology 2000, 56 TH VolumeDocument11 pagesPeriodontology 2000, 56 TH VolumeSmitha Kapani gowdaNo ratings yet
- CERTIFICATION IN ADVANCED HEART FAIlURE AND TRANSPlANT CARDIOlOGY - American Board of Internal MedicineDocument4 pagesCERTIFICATION IN ADVANCED HEART FAIlURE AND TRANSPlANT CARDIOlOGY - American Board of Internal MedicineabimorgNo ratings yet
- Clinical Approach in Generalized Pustular Psoriasis One Case Report 63a04e949936aDocument8 pagesClinical Approach in Generalized Pustular Psoriasis One Case Report 63a04e949936aThomas UtomoNo ratings yet
- Gestational Diabetus MellitusDocument28 pagesGestational Diabetus MellitusSanthosh.S.UNo ratings yet
- Cristian Colceriu - Elitele României - Prof. Dr. Ștefan Florian - Cluj Contemporary ElitesDocument15 pagesCristian Colceriu - Elitele României - Prof. Dr. Ștefan Florian - Cluj Contemporary Elitescristian colceriuNo ratings yet
- RasproDocument63 pagesRasprofany hertinNo ratings yet
- Hippocrates EnglishDocument4 pagesHippocrates EnglishOtilia GuliiNo ratings yet
- Pamphlet TemplateDocument2 pagesPamphlet TemplateZoe ColemanNo ratings yet
- Sorbion SachetsDocument3 pagesSorbion SachetsReil_InsulaNo ratings yet
- Pressure SoreDocument3 pagesPressure SoreGhadaNo ratings yet
- National Oral Health Program GuidelinesDocument21 pagesNational Oral Health Program GuidelinesAniket PotnisNo ratings yet
- Breast Reduction Techniques ExplainedDocument6 pagesBreast Reduction Techniques ExplainedMiguelito JohnsonNo ratings yet
- Occlusal Considerations in Periodontics: OcclusionDocument9 pagesOcclusal Considerations in Periodontics: OcclusionnathaliaNo ratings yet
- Jurnal ReadingDocument13 pagesJurnal Readingeliamegasari01No ratings yet
- Knowledge of Tetanus Disease and Vaccination Remains Low Among Women in PakistanDocument6 pagesKnowledge of Tetanus Disease and Vaccination Remains Low Among Women in Pakistankhalida yaqubNo ratings yet