You might also like
- Discover the training secrets of legendary bodybuildersDocument129 pagesDiscover the training secrets of legendary bodybuildersfatmir100% (7)
- KetamineDocument37 pagesKetamineRajesh Reddy Chintakunta100% (1)
- Drugs in ICUDocument83 pagesDrugs in ICUJennifer DixonNo ratings yet
- Stanley - Your Voice (1957) PDFDocument396 pagesStanley - Your Voice (1957) PDFŠašavi Sam MajmunNo ratings yet
- The Strange ICA Stones of PeruDocument31 pagesThe Strange ICA Stones of PeruRoman Aleshkevich100% (1)
- Traits and BehaviorDocument8 pagesTraits and BehaviorNorwafa Cariga EspinosaNo ratings yet
- Passenger Ship SubdivisionDocument6 pagesPassenger Ship SubdivisionPunit Pandey100% (2)
- Intravenous Induction AgentsDocument59 pagesIntravenous Induction Agentsroundnumber100% (1)
- Local Anesthetics and Nerve Blocks HannanDocument57 pagesLocal Anesthetics and Nerve Blocks Hannanpriya_edwinNo ratings yet
- DCM601A51 - Technical DataDocument405 pagesDCM601A51 - Technical Datathanhthuan100% (1)
- 2016 Pharmacology of Sedative-HypnoticDocument46 pages2016 Pharmacology of Sedative-HypnoticFansisca SiallaganNo ratings yet
- Ibsen in PracticeDocument17 pagesIbsen in PracticevictorkalkaNo ratings yet
- Induction AgentsDocument100 pagesInduction AgentsSulfikar TknNo ratings yet
- 6 DLL HOPE 3 2019-2020 JulyDocument2 pages6 DLL HOPE 3 2019-2020 JulyCelia BautistaNo ratings yet
- IV Induction Agents UMAIDDocument63 pagesIV Induction Agents UMAIDUmaid Mirza100% (1)
- Pharma ChartsDocument33 pagesPharma ChartsNooreen Hussain100% (1)
- Intravenous Anesthetic Agents: by Miss Maidah MehtabDocument49 pagesIntravenous Anesthetic Agents: by Miss Maidah MehtabLuqman QadirNo ratings yet
- BD 1050 PartesDocument26 pagesBD 1050 PartesFelipe RojasNo ratings yet
- AntiepilepticiDocument29 pagesAntiepilepticiIskraNo ratings yet
- Drug Presentation: Manisha M.Sc. Nursing 1 Year Con IlbsDocument57 pagesDrug Presentation: Manisha M.Sc. Nursing 1 Year Con IlbsManisha ShakyaNo ratings yet
- DR DR Pramod Pramod K Sharma K SharmaDocument77 pagesDR DR Pramod Pramod K Sharma K SharmaSaurabh Gautam100% (1)
- Intravenous Anesthetics: JRRMMC PGI Regalado, Trina Elisse TDocument18 pagesIntravenous Anesthetics: JRRMMC PGI Regalado, Trina Elisse THoneylynNo ratings yet
- Antiepileptics (Autosaved)Document57 pagesAntiepileptics (Autosaved)vishal singhNo ratings yet
- Basic Pharmacology of Anesthesia DrugsDocument42 pagesBasic Pharmacology of Anesthesia Drugsansuh22100% (1)
- Intravenous AnestheticsDocument95 pagesIntravenous AnestheticsEmilio JacintoNo ratings yet
- Ketamine ?Document42 pagesKetamine ?Shaik NisaNo ratings yet
- Sedative/ Hypnotics: Silim, Miriam Grace DDocument29 pagesSedative/ Hypnotics: Silim, Miriam Grace DDeloria, Alma J.No ratings yet
- 08 .麻醉用藥 - 邱全秀Document62 pages08 .麻醉用藥 - 邱全秀kenny631653No ratings yet
- Toxicology of Drugs of Abuse: Robert Paul S. Lim, RPHDocument71 pagesToxicology of Drugs of Abuse: Robert Paul S. Lim, RPHƉarwin Lopez ObelNo ratings yet
- IV Induction Agents Slides For Podcast UpdatedDocument59 pagesIV Induction Agents Slides For Podcast UpdateddsfdsfNo ratings yet
- AntiepilepticsDocument16 pagesAntiepilepticsDivyaNo ratings yet
- Local Anaesthetic Agents (3) 2Document38 pagesLocal Anaesthetic Agents (3) 2MaleehaNo ratings yet
- Malignan HipertermiaDocument10 pagesMalignan HipertermiaAstrid Ghea GayatriNo ratings yet
- Intravenous AnestheticsDocument5 pagesIntravenous AnestheticsPM Basiloy - AloNo ratings yet
- Dept - Farmakologi & Terapeutik Fak - Kedokteran U S U Medan: Prof - Dr.H.Aznan Lelo PHD - SPFK DR - Datten Bangun MSC, SPFKDocument62 pagesDept - Farmakologi & Terapeutik Fak - Kedokteran U S U Medan: Prof - Dr.H.Aznan Lelo PHD - SPFK DR - Datten Bangun MSC, SPFKAnonymous zZrGTONhNo ratings yet
- Obat-Obat Emergency: DR T. Mamfaluti, SPPDDocument36 pagesObat-Obat Emergency: DR T. Mamfaluti, SPPDIqbal AminNo ratings yet
- KetamineDocument24 pagesKetamineMalik Arif UllahNo ratings yet
- Local Anaesthetics: Essential Guide to Properties and MechanismsDocument17 pagesLocal Anaesthetics: Essential Guide to Properties and MechanismsaliNo ratings yet
- Anti-Epilepsy Agents: DR Gareth NobleDocument50 pagesAnti-Epilepsy Agents: DR Gareth NoblekundagolNo ratings yet
- Iv Induction Agents: DR Afreen Department of Anaesthesiology Chettinad Hospital and Research CentreDocument59 pagesIv Induction Agents: DR Afreen Department of Anaesthesiology Chettinad Hospital and Research CentreKannan GNo ratings yet
- Psychotropic Substance Hallucinogens and Dissociatives_compressedDocument39 pagesPsychotropic Substance Hallucinogens and Dissociatives_compressedshuyuichewNo ratings yet
- ICU Pharmacology: Sedatives Analgesics Paralytics PressorsDocument51 pagesICU Pharmacology: Sedatives Analgesics Paralytics Pressorsdevi trismiaNo ratings yet
- Pharma Drug Tables - 1st ShiftingDocument29 pagesPharma Drug Tables - 1st ShiftingHei LeeNo ratings yet
- 6 AnesthesiaDocument55 pages6 AnesthesiaSarah MehyarNo ratings yet
- LOCAL ANAESTHETIC DRUGS: PROPERTIES AND TOXICITYDocument35 pagesLOCAL ANAESTHETIC DRUGS: PROPERTIES AND TOXICITYmealiella omarNo ratings yet
- Antiepileptics PD 501Document27 pagesAntiepileptics PD 501SidraNo ratings yet
- Intrvenous Induction Agents: DR - Keerthi Rekha Dept. of AnaesthesiologyDocument33 pagesIntrvenous Induction Agents: DR - Keerthi Rekha Dept. of Anaesthesiologykeerthi_keshapagaNo ratings yet
- General AnestDocument35 pagesGeneral AnestMauz AshrafNo ratings yet
- CardiotropicsDocument4 pagesCardiotropicsbeans taralaNo ratings yet
- Intravenous Anesthetic Agent NewDocument17 pagesIntravenous Anesthetic Agent NewDr RabbiNo ratings yet
- Naloxone and Flumazenil for Opioid and Benzodiazepine OverdoseDocument3 pagesNaloxone and Flumazenil for Opioid and Benzodiazepine OverdoseDanial HadiNo ratings yet
- ICU Pharmacology Guide: Sedatives, Analgesics, Paralytics & PressorsDocument52 pagesICU Pharmacology Guide: Sedatives, Analgesics, Paralytics & Pressorscoolboy1990No ratings yet
- AnestesiDocument59 pagesAnestesiJeffrey EkaNo ratings yet
- Neurohumoral Transmission, Parasympatholytics, PS MimeticsDocument51 pagesNeurohumoral Transmission, Parasympatholytics, PS MimeticsrajeswariNo ratings yet
- Status Epilepticus GuideDocument10 pagesStatus Epilepticus GuideGladys MainaNo ratings yet
- Local Anesthetics and Nerve Blocks HannanDocument57 pagesLocal Anesthetics and Nerve Blocks Hannanpriya_edwinNo ratings yet
- Obat SimpatomimetikDocument42 pagesObat SimpatomimetiknatinlalaNo ratings yet
- PROPOFOLDocument22 pagesPROPOFOLAnusha PradeepNo ratings yet
- Pharmacology Reporting-1Document32 pagesPharmacology Reporting-1Mj TalentNo ratings yet
- ICU PharmacologyDocument18 pagesICU PharmacologyIrsani FeniliaNo ratings yet
- Uia 13 DELAYED AWAKENING OR EMERGENCE FROM ANAESTHESIADocument3 pagesUia 13 DELAYED AWAKENING OR EMERGENCE FROM ANAESTHESIAsunny kumarNo ratings yet
- Neuropharmacology Agents in Neuroscience NursingDocument36 pagesNeuropharmacology Agents in Neuroscience NursingDebika DasNo ratings yet
- Endocrinology Neuroendocrinology Neuropeptides: Proceedings of the 28th International Congress of Physiological Sciences, Budapest, 1980From EverandEndocrinology Neuroendocrinology Neuropeptides: Proceedings of the 28th International Congress of Physiological Sciences, Budapest, 1980E. StarkNo ratings yet
- Neurotransmission: Proceedings of the Sixth International Congress of PharmacologyFrom EverandNeurotransmission: Proceedings of the Sixth International Congress of PharmacologyLiisa AhteeNo ratings yet
- Physiology for General Surgical Sciences Examination (GSSE)From EverandPhysiology for General Surgical Sciences Examination (GSSE)S. Ali MirjaliliNo ratings yet
- 4140DE Data SheetDocument1 page4140DE Data SheetNabeel AmeerNo ratings yet
- Opening SpeechDocument1 pageOpening SpeechTaniușa SavaNo ratings yet
- Introducion To Load Cells UtilcellDocument22 pagesIntroducion To Load Cells UtilcellRifi MohamedNo ratings yet
- Smart medical system monitors dementia patients' medicationDocument9 pagesSmart medical system monitors dementia patients' medicationKresnaNo ratings yet
- Volcanic Eruption Types and ProcessDocument18 pagesVolcanic Eruption Types and ProcessRosemarie Joy TanioNo ratings yet
- Complementary Therapies in Clinical Practice: Effect of Aromatherapy On Post-Partum Complications: A Systematic ReviewDocument7 pagesComplementary Therapies in Clinical Practice: Effect of Aromatherapy On Post-Partum Complications: A Systematic ReviewAras PinantiNo ratings yet
- Low Noise Pseudomorphic HEMT Technical DataDocument4 pagesLow Noise Pseudomorphic HEMT Technical Datahendpraz88No ratings yet
- 4-Ingredient Vegan Easy Brownies - Minimalist Baker RecipesDocument2 pages4-Ingredient Vegan Easy Brownies - Minimalist Baker RecipespeteNo ratings yet
- Practicum HandbookDocument12 pagesPracticum HandbookChikezie NwankworNo ratings yet
- Master FormDocument62 pagesMaster FormsamsulNo ratings yet
- Non-Digestible Oligosaccharides: A Review: Solange I. Mussatto, Ismael M. MancilhaDocument11 pagesNon-Digestible Oligosaccharides: A Review: Solange I. Mussatto, Ismael M. MancilhaPatrícia Felix ÁvilaNo ratings yet
- Arthur Kleinman The Illness Narratives Suffering Healing and The Human ConditionDocument46 pagesArthur Kleinman The Illness Narratives Suffering Healing and The Human Conditionperdidalma62% (13)
- MEH B1 Video Book Answer KeyDocument6 pagesMEH B1 Video Book Answer KeyTru CallingNo ratings yet
- GER Bangladesh EngDocument12 pagesGER Bangladesh Engfarhan.anjum20032004No ratings yet
- 1-Well Completion I PDFDocument20 pages1-Well Completion I PDFHomam MohammadNo ratings yet
- Online Pharmacy: Customer ProfilingDocument6 pagesOnline Pharmacy: Customer ProfilingGeorge SebastianNo ratings yet
- Nikola Tesla Would Have Celebrated Christmas On January 7thDocument3 pagesNikola Tesla Would Have Celebrated Christmas On January 7thAnonymous DfeajF100% (1)
- Benign EntitiesDocument37 pagesBenign EntitiesleartaNo ratings yet
- Technical Data Sheet PDFDocument2 pagesTechnical Data Sheet PDFLuis VilelaNo ratings yet
- The Electrooculogram (EOG)Document34 pagesThe Electrooculogram (EOG)Prasidha PrabhuNo ratings yet
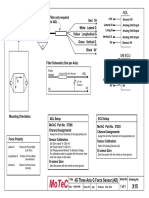
- Filter and wiring schematic for 3-axis ADL G-force sensorDocument1 pageFilter and wiring schematic for 3-axis ADL G-force sensorJuan Ramón Pérez LorenzoNo ratings yet