You might also like
- ATSP Booklet 2023Document26 pagesATSP Booklet 2023Savanthi Carmaline de SilvaNo ratings yet
- Internship ManualDocument29 pagesInternship ManualJigsNo ratings yet
- BHRUT Endoscopy Induction Pack v1.5 (Final)Document17 pagesBHRUT Endoscopy Induction Pack v1.5 (Final)vlad910No ratings yet
- Advanced Cardiac Life SupportDocument37 pagesAdvanced Cardiac Life SupportRoy Acosta GumbanNo ratings yet
- ECMO and Right Ventricular FailureDocument9 pagesECMO and Right Ventricular FailureLuis Fernando Morales JuradoNo ratings yet
- Drugs in Cardiac EnmergenciesDocument94 pagesDrugs in Cardiac EnmergenciesVijayan VelayudhanNo ratings yet
- Vascular Responses to PathogensFrom EverandVascular Responses to PathogensFelicity N.E. GavinsNo ratings yet
- Antrim ED Handbook 2019Document238 pagesAntrim ED Handbook 2019Chris Jardine LiNo ratings yet
- Ineffective Coping - Nursing Diagnosis & Care Plan - NurseslabsDocument13 pagesIneffective Coping - Nursing Diagnosis & Care Plan - NurseslabsLester MooreNo ratings yet
- Scape Vs FospeDocument5 pagesScape Vs FospeDr. FarhanNo ratings yet
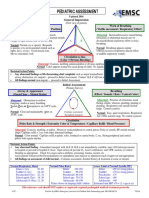
- PEDIATRIC ASSESSMENT OVERVIEWDocument2 pagesPEDIATRIC ASSESSMENT OVERVIEWAghnia Nafila100% (1)
- ATSP (Asked To See Patient) BookletDocument24 pagesATSP (Asked To See Patient) BookletCindy WongNo ratings yet
- Cardiac/Cardiogenic Shock: Clinical Practice GuidelinesDocument3 pagesCardiac/Cardiogenic Shock: Clinical Practice GuidelinesAnonymous Yo0mStNo ratings yet
- Management of Arterial LineDocument16 pagesManagement of Arterial LineFarcasanu Liana GeorgianaNo ratings yet
- Heart and Neck AssessmentDocument3 pagesHeart and Neck AssessmentKiara Ash BeethovenNo ratings yet
- A3 - ABCDE Algorithms PDFDocument63 pagesA3 - ABCDE Algorithms PDFteguhNo ratings yet
- 5 Shock PPT EnglishDocument77 pages5 Shock PPT EnglishKessi VikaneswariNo ratings yet
- @anesthesia Books 2013 Critical PDFDocument4,361 pages@anesthesia Books 2013 Critical PDFJa AlNo ratings yet
- Travis: Blaser, RNDocument1 pageTravis: Blaser, RNapi-540097476No ratings yet
- MN105613 PICU2022 Book ProofDocument60 pagesMN105613 PICU2022 Book ProofErwin Dela GanaNo ratings yet
- Textbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersFrom EverandTextbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersNo ratings yet
- Pulmo ThromboembolismDocument34 pagesPulmo ThromboembolismAlexander Santiago ParelNo ratings yet
- ACLS Algorithms Adult 2010 Revised May 31 2011Document12 pagesACLS Algorithms Adult 2010 Revised May 31 2011arturschander3614No ratings yet
- 10 GP ConsultationsDocument4 pages10 GP ConsultationsDev KumarNo ratings yet
- Nursing Care of PlanDocument16 pagesNursing Care of PlanDbyNo ratings yet
- Rass and Cam-IcuDocument3 pagesRass and Cam-Icuأمينةأحمد100% (1)
- ICU Registered Nurse Resume Brick RedDocument2 pagesICU Registered Nurse Resume Brick RedAngelNo ratings yet
- Medical-Surgical Nursing Review Flashcards - QuizletDocument14 pagesMedical-Surgical Nursing Review Flashcards - QuizletNursyNurse100% (1)
- Nutrition Support in Critically Ill Patients - An Overview - UpToDateDocument23 pagesNutrition Support in Critically Ill Patients - An Overview - UpToDateduong tien truongNo ratings yet
- Physical Examination Techniques and ManueversDocument160 pagesPhysical Examination Techniques and ManueversMa-anJaneDiamosNo ratings yet
- American Heart Association Guidelines For CPR 2015: Christopher RyalinoDocument50 pagesAmerican Heart Association Guidelines For CPR 2015: Christopher RyalinoLightNo ratings yet
- PALS 2015 Update - Nursing Grand RoundsDocument22 pagesPALS 2015 Update - Nursing Grand RoundshatsuneNo ratings yet
- Normal Ranges Vital Signs 2017Document2 pagesNormal Ranges Vital Signs 2017Elvis Nguyen100% (1)
- IV PDFDocument63 pagesIV PDFelbagouryNo ratings yet
- Burns Assessment and ManagementDocument33 pagesBurns Assessment and ManagementErina Erichan Oto100% (1)
- ACC/AHA STEMI GuidelinesDocument94 pagesACC/AHA STEMI GuidelinesDika DekokNo ratings yet
- Physical ExaminationDocument55 pagesPhysical Examinationdakshpanchal26369No ratings yet
- Critical Event ChecklistsDocument25 pagesCritical Event ChecklistsarisyiNo ratings yet
- Wellbeing For The ResuscitationistDocument142 pagesWellbeing For The Resuscitationistibeardsell1100% (1)
- Dysrhythmia TestsDocument3 pagesDysrhythmia TestsKimberly WhitesideNo ratings yet
- Fluid and Electrolyte Balance in ICUDocument46 pagesFluid and Electrolyte Balance in ICUtapas_kbNo ratings yet
- Poster 10 PALS 01 01 ENG V20100927 PDFDocument1 pagePoster 10 PALS 01 01 ENG V20100927 PDFAndy XiaoNo ratings yet
- OBGYN HistoryDocument1 pageOBGYN Historysgod34No ratings yet
- Essential Cases for GP TraineesDocument3 pagesEssential Cases for GP TraineesTahir AliNo ratings yet
- How To Treat: Septic ShockDocument6 pagesHow To Treat: Septic ShockmeeandsoeNo ratings yet
- Lung Transplant PathwayDocument39 pagesLung Transplant PathwayMohana Preethi MNo ratings yet
- Diabetes and Complications: When Documenting Diabetes, It's Important To Note The FollowingDocument2 pagesDiabetes and Complications: When Documenting Diabetes, It's Important To Note The Followingmeikaizen100% (1)
- BLS Study Guide 020620013Document38 pagesBLS Study Guide 020620013R RatheeshNo ratings yet
- Mock CodeDocument4 pagesMock CodeKrezielDulosEscobarNo ratings yet
- Chest Pain: Jean J. Chatham, MDDocument40 pagesChest Pain: Jean J. Chatham, MDYermia RashaquatNo ratings yet
- Total Parenteral Nutrition Guideline-4 - 2Document38 pagesTotal Parenteral Nutrition Guideline-4 - 2Henry M. BarberenaNo ratings yet
- Treatment of Resistant and Refractory HypertensionDocument21 pagesTreatment of Resistant and Refractory HypertensionLuis Rodriguez100% (1)
- Assessment Algorithm For Sedated Adult ICU Patients: No YesDocument18 pagesAssessment Algorithm For Sedated Adult ICU Patients: No YeshendraNo ratings yet