You might also like
- Surgery Clerkship Oral Exam ReviewDocument18 pagesSurgery Clerkship Oral Exam Reviewpanther795100% (1)
- Nursing Care PlanDocument10 pagesNursing Care PlanZerica Andaca83% (6)
- First Aid and Basic Life Support CI PRINTINGDocument90 pagesFirst Aid and Basic Life Support CI PRINTINGTrisha Apillanes100% (2)
- ICU Checklist - TEN FASTHUGSSS v3.0Document35 pagesICU Checklist - TEN FASTHUGSSS v3.0gxjjsjejdu100% (3)
- Burns and The Reconstructive LaderDocument70 pagesBurns and The Reconstructive LaderAmit RamrattanNo ratings yet
- Sample Nursing Care PlansDocument18 pagesSample Nursing Care Planslaritza100% (3)
- James Notes For SurgeryDocument193 pagesJames Notes For SurgeryAnonymous w4lLoMd7No ratings yet
- Chapter 1-OMFS Interns 2020-Book Club (Corona Edition) PDFDocument49 pagesChapter 1-OMFS Interns 2020-Book Club (Corona Edition) PDFMGCNo ratings yet
- BurnsDocument38 pagesBurnsMark AlfabetoNo ratings yet
- 26) BurnsDocument35 pages26) BurnsMariam AntonyNo ratings yet
- Burn InjuryDocument80 pagesBurn InjuryQueena Neysa CalcarinaNo ratings yet
- Renal: Anatomy + PhysiologyDocument29 pagesRenal: Anatomy + PhysiologyAdriana ChasiguanoNo ratings yet
- Hematology 1 Mtap1Document70 pagesHematology 1 Mtap1Cyril Llego ManuelNo ratings yet
- Management of Burn Injuries: Dr. Lawal G.D Registrar, Dept. of Surgery, NHADocument53 pagesManagement of Burn Injuries: Dr. Lawal G.D Registrar, Dept. of Surgery, NHAawesome0% (1)
- Burn PPT ShashiDocument4 pagesBurn PPT ShashiSachin KonkaniNo ratings yet
- Thermal InjuriesDocument23 pagesThermal Injuriesadam NoheNo ratings yet
- Focus Review For ATIDocument16 pagesFocus Review For ATIphandrew0892% (50)
- "Cryotherapy": Presented ByDocument23 pages"Cryotherapy": Presented Byyaraa6805No ratings yet
- Thyroidectomy RadhDocument73 pagesThyroidectomy RadhradhikasreedharNo ratings yet
- Burn Managment: Ns Hamka, M.Kep., RN., WOC (ET) NDocument52 pagesBurn Managment: Ns Hamka, M.Kep., RN., WOC (ET) NNci Centre KalimantanNo ratings yet
- Committee On Trauma Presents: Therma L InjuriesDocument35 pagesCommittee On Trauma Presents: Therma L InjuriesJavar SodicNo ratings yet
- Cupping TherapyDocument20 pagesCupping TherapyMohamed AttiaNo ratings yet
- FundamentalsDocument34 pagesFundamentalsColleen CalditoNo ratings yet
- WoundsDocument40 pagesWoundsDr Sania SardarNo ratings yet
- Administering Cold Therapy CanvaDocument25 pagesAdministering Cold Therapy CanvaAlex OppusNo ratings yet
- Pediatric ConceptDocument19 pagesPediatric ConceptAntonio Intia IVNo ratings yet
- Committee On Trauma Presents: Thermal InjuriesDocument35 pagesCommittee On Trauma Presents: Thermal InjuriesAlfina Aulia RizkiNo ratings yet
- Perilite ExposureDocument15 pagesPerilite ExposureBella Cy Lopez67% (3)
- Nursing Management of BurnDocument40 pagesNursing Management of BurnSalinKaur0% (1)
- Case Audit Mixed Degree Burns: DR Hareesh Kumar R Dept of General SurgeryDocument23 pagesCase Audit Mixed Degree Burns: DR Hareesh Kumar R Dept of General SurgeryRazor GGNo ratings yet
- Burn Lecture NotesDocument7 pagesBurn Lecture NotesMarcus, RN100% (3)
- Rehabilitation Post StrokeDocument27 pagesRehabilitation Post StrokeNorNashiraMohdIbrahimNo ratings yet
- BAD Cryotherapy Update March 2018 - Lay Review March 2018Document4 pagesBAD Cryotherapy Update March 2018 - Lay Review March 2018Kaka ShunkNo ratings yet
- Hot and Cold Application - PPTX RevisedDocument61 pagesHot and Cold Application - PPTX RevisedMicah HuanNo ratings yet
- First Aid - CPR ProjectDocument13 pagesFirst Aid - CPR ProjectJade MorrisNo ratings yet
- Burns & Burn Management, Asphyxiation, and Head InjuriesDocument77 pagesBurns & Burn Management, Asphyxiation, and Head InjuriesGabz GabbyNo ratings yet
- Medical Surgical NursingDocument76 pagesMedical Surgical NursingARIANE DOLINONo ratings yet
- 11 BurnDocument31 pages11 Burnjitendra magarNo ratings yet
- Accident & EmergencyDocument7 pagesAccident & EmergencyAdeel HaiderNo ratings yet
- Must KnowsDocument8 pagesMust KnowsVincent Lawrence D. MarcosNo ratings yet
- LC 02 Primary Care & Emergency ProceduresDocument21 pagesLC 02 Primary Care & Emergency ProceduresPayalNo ratings yet
- BurnDocument11 pagesBurnsofea zamriNo ratings yet
- Heat and Cold Application: Wella Grace A. Go, RN, RMDocument24 pagesHeat and Cold Application: Wella Grace A. Go, RN, RMPaulineNo ratings yet
- Bleeding, Burns, and Shock: Bio Medicine - Emergency Medicine #2 Dr. Spencer ShimabukuroDocument37 pagesBleeding, Burns, and Shock: Bio Medicine - Emergency Medicine #2 Dr. Spencer ShimabukurochaiyoonNo ratings yet
- Integumentary NotesDocument5 pagesIntegumentary NotesRiyue KreoNo ratings yet
- Transes Tra - Peri-OpDocument11 pagesTranses Tra - Peri-OpJoshua DelantarNo ratings yet
- BurnsDocument9 pagesBurnsVincentus BinNo ratings yet
- Combutio 2019Document52 pagesCombutio 2019Dannish Alii0% (1)
- Surgical Aspects of Diabetes MellitusDocument27 pagesSurgical Aspects of Diabetes MellitusSushmi RajanNo ratings yet
- Burn - Emergency ManagementDocument28 pagesBurn - Emergency ManagementHira Ashraf100% (1)
- Burns - Types, Symptoms & Treatment Nursing ManagementDocument15 pagesBurns - Types, Symptoms & Treatment Nursing ManagementJubitta JobyNo ratings yet
- Pediatric DERMATOLOGYDocument12 pagesPediatric DERMATOLOGYalex ocasioNo ratings yet
- Physiotherapy Management of Secondary Impairments in Patients With StrokeDocument18 pagesPhysiotherapy Management of Secondary Impairments in Patients With StrokeBryan ChiamNo ratings yet
- General Principles of Skin Graft and FlapsDocument61 pagesGeneral Principles of Skin Graft and FlapsamalNo ratings yet
- 1soft Tissue TraumaDocument60 pages1soft Tissue TraumaZosima Caniga GabuleNo ratings yet
- Hydrotherapy: 20 Minutes or Less for Health and BeautyFrom EverandHydrotherapy: 20 Minutes or Less for Health and BeautyNo ratings yet
- Different in the therapy of pressure negtotheeva single-useFrom EverandDifferent in the therapy of pressure negtotheeva single-useNo ratings yet
- Soak It In: Hydrotherapy Treatments In 20 Minutes or Less for Health and BeautyFrom EverandSoak It In: Hydrotherapy Treatments In 20 Minutes or Less for Health and BeautyNo ratings yet
- Emergency Nclex QuestionsDocument19 pagesEmergency Nclex QuestionsAlsalman Anam100% (8)
- 4.3 LP 5 Hypovolemic Shock - PPSXDocument40 pages4.3 LP 5 Hypovolemic Shock - PPSXCamelia A. ParuschiNo ratings yet
- Hypovolemic Shock TEXTDocument5 pagesHypovolemic Shock TEXTrhen1991No ratings yet
- Shock - StatPearls - NCBI BookshelfDocument5 pagesShock - StatPearls - NCBI BookshelfSYAFIRA LAILA NURULITANo ratings yet
- Shock - Critical Care Medicine - MSD Manual Professional EditionDocument11 pagesShock - Critical Care Medicine - MSD Manual Professional Editionazaria zhafirahNo ratings yet
- Signs and Symptoms of Shock in Children and Infant1Document2 pagesSigns and Symptoms of Shock in Children and Infant1Alfiani Mar'atussalehahNo ratings yet
- Nursing Care Plan On Platelet DisordersDocument8 pagesNursing Care Plan On Platelet DisordersbhavanaNo ratings yet
- Emergency Room Medicine Notes ATFDocument192 pagesEmergency Room Medicine Notes ATFGiovanna Moller100% (3)
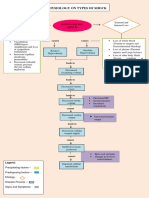
- Pathophysiology On Types of ShockDocument4 pagesPathophysiology On Types of ShockJessa Mae Alforque AsentistaNo ratings yet
- Fluid Management in The Critically Ill: Jean-Louis VincentDocument6 pagesFluid Management in The Critically Ill: Jean-Louis VincentLucas MontanhaNo ratings yet
- Shock Cheat Sheet PDFDocument2 pagesShock Cheat Sheet PDFRupert AsesorNo ratings yet
- Fluid Therapy For Critically Ill Dogs and Cats - WSAVA2005 - VINDocument14 pagesFluid Therapy For Critically Ill Dogs and Cats - WSAVA2005 - VINHament KumarNo ratings yet
- Dr. Az Rifki, Span - Kic Departemen Anestesiologi Dan Reanimasi Rsi Siti Rahmah/Fk-Fkg Universitas Baiturrahmah PadangDocument62 pagesDr. Az Rifki, Span - Kic Departemen Anestesiologi Dan Reanimasi Rsi Siti Rahmah/Fk-Fkg Universitas Baiturrahmah PadangKamelia MarcshendaNo ratings yet
- Fluid Management in Acute Kidney InjuryDocument8 pagesFluid Management in Acute Kidney InjuryHGZ 83 MoreliaNo ratings yet
- Fluids and ElectrolytesDocument142 pagesFluids and ElectrolytesAndradaLavricNo ratings yet
- 3 Tactical Field CareDocument164 pages3 Tactical Field CareINSTRUCTOR INTERNACIONAL ANTONIO RAMIREZNo ratings yet
- Stages of ShockDocument13 pagesStages of ShockA. P.No ratings yet
- Burn Case Study - Saisankalp Shankar - 3A PathophysiologyDocument3 pagesBurn Case Study - Saisankalp Shankar - 3A PathophysiologysaimarvelousNo ratings yet
- Shock and HemorrhageDocument29 pagesShock and HemorrhageDr djNo ratings yet
- Report About Dengue: Introduction: Dengue Fever Is A Viral Illness Transmitted ToDocument11 pagesReport About Dengue: Introduction: Dengue Fever Is A Viral Illness Transmitted ToMike Faustino SolangonNo ratings yet
- Risk For DehydrationDocument2 pagesRisk For DehydrationJahne CM80% (5)
- Intestinal Failure AdultsDocument12 pagesIntestinal Failure Adultssilvio da costa guerreiroNo ratings yet
- Multiple TraumaDocument5 pagesMultiple TraumaChristabel EdithNo ratings yet
- Cardiovascular Management of Septic ShockDocument10 pagesCardiovascular Management of Septic ShockErwin RachmadNo ratings yet
- Shock PresentationDocument20 pagesShock Presentationrosalyn sugayNo ratings yet
- Refelctive Journal Development 346Document2 pagesRefelctive Journal Development 346Jennifer Goodlet100% (1)
- MODULE 5 - DISASTER AWARENESS AND MANAGEMENT - PPT EditedDocument43 pagesMODULE 5 - DISASTER AWARENESS AND MANAGEMENT - PPT Edited(MG)PEDAWGNo ratings yet
- Vasoactive MedicationsDocument1 pageVasoactive Medicationsapi-635152754No ratings yet