You might also like
- Principles and Applications of Clinical Mass Spectrometry: Small Molecules, Peptides, and PathogensFrom EverandPrinciples and Applications of Clinical Mass Spectrometry: Small Molecules, Peptides, and PathogensNader RifaiNo ratings yet
- Clinical Gait Assessment in The Neurologically ImpairedDocument6 pagesClinical Gait Assessment in The Neurologically Impairedvamat63No ratings yet
- Current Concepts in Dupuytren's DiseaseDocument10 pagesCurrent Concepts in Dupuytren's DiseaseandrehrNo ratings yet
- Metaanalysis Distal End Radius Volar Plate Vs Conservative2058 5241 EOR 22 0022Document9 pagesMetaanalysis Distal End Radius Volar Plate Vs Conservative2058 5241 EOR 22 0022Mohan DesaiNo ratings yet
- Holt by 2004Document6 pagesHolt by 2004saviraNo ratings yet
- Activity and Basic Mobility Short Forms Validity of The AM-PAC ''6-Clicks'' Inpatient DailyDocument36 pagesActivity and Basic Mobility Short Forms Validity of The AM-PAC ''6-Clicks'' Inpatient Dailyapi-241031382No ratings yet
- 2 Different Methods of Goniometric Measurement For Forearm Pronation and SupinationDocument9 pages2 Different Methods of Goniometric Measurement For Forearm Pronation and SupinationSachin SethiNo ratings yet
- Reliability of Gait Performance Tests in Men and Women With Hemiparesis After StrokeDocument8 pagesReliability of Gait Performance Tests in Men and Women With Hemiparesis After StrokeKaniNo ratings yet
- 10 1016@j JHT 2017 02 001 PDFDocument10 pages10 1016@j JHT 2017 02 001 PDFGusti Ayu KrisnayantiNo ratings yet
- Paper Section 3 Draft1Document11 pagesPaper Section 3 Draft1api-568855135No ratings yet
- Measuring The Whole or The Parts?Document15 pagesMeasuring The Whole or The Parts?Janaiana UchoaNo ratings yet
- Inter ReliabilityDocument3 pagesInter ReliabilityDeepi GurungNo ratings yet
- Early Detection of Parkinson's Disease Through Patient Questionnaire and Predictive ModellingDocument42 pagesEarly Detection of Parkinson's Disease Through Patient Questionnaire and Predictive ModellingKanagaraj SubramaniNo ratings yet
- 1106 FullDocument14 pages1106 Fullnanthini kanasanNo ratings yet
- Guideline On Anterior Cruciate Ligament InjuryDocument9 pagesGuideline On Anterior Cruciate Ligament Injuryanggraini wahyuNo ratings yet
- 1106 FullDocument14 pages1106 Fullmarcos viniciusNo ratings yet
- Yjmt 30 1992090Document13 pagesYjmt 30 1992090Luis Sebastian Arango OspinaNo ratings yet
- Physical Function of RA Patients Tapering TreatmenDocument7 pagesPhysical Function of RA Patients Tapering Treatmenuyenminhdl88No ratings yet
- Franciosi-13 RS Variables Clinicas HDDocument8 pagesFranciosi-13 RS Variables Clinicas HDMARIA MONTSERRAT SOMOZA MONCADANo ratings yet
- Tveter 2014Document8 pagesTveter 2014Thays VotaçõesNo ratings yet
- Robot-Assisted Therapy For Long-Term Upper-Limb Impairment After StrokeDocument8 pagesRobot-Assisted Therapy For Long-Term Upper-Limb Impairment After StrokerimarahmadiptaNo ratings yet
- s12984 019 0568 yDocument11 pagess12984 019 0568 yTONY HII CHANG SOONNo ratings yet
- Rotator Cuff Shoulder Pain DiagnosticDocument14 pagesRotator Cuff Shoulder Pain DiagnosticTomBramboNo ratings yet
- Management of Plantar Heel Pain: A Best Practice Guide Informed by A Systematic Review, Expert Clinical Reasoning and Patient ValuesDocument14 pagesManagement of Plantar Heel Pain: A Best Practice Guide Informed by A Systematic Review, Expert Clinical Reasoning and Patient ValuesDavid SoaresNo ratings yet
- Management of Plantar Heel Pain: A Best Practice Guide Informed by A Systematic Review, Expert Clinical Reasoning and Patient ValuesDocument14 pagesManagement of Plantar Heel Pain: A Best Practice Guide Informed by A Systematic Review, Expert Clinical Reasoning and Patient ValuesMaximiliano LabraNo ratings yet
- 2021 03 30 21254578 FullDocument21 pages2021 03 30 21254578 Fullestefy140399No ratings yet
- Two Casting Methods Compared in Patients With Colles' Fracture: A Pragmatic, Randomized Controlled TrialDocument12 pagesTwo Casting Methods Compared in Patients With Colles' Fracture: A Pragmatic, Randomized Controlled TrialTeja Laksana NukanaNo ratings yet
- A Systematic Review of Satisfaction With TeledermatologyDocument8 pagesA Systematic Review of Satisfaction With Teledermatologysri karuniaNo ratings yet
- Articlereport 1Document5 pagesArticlereport 1api-704750924No ratings yet
- Poster PapersDocument262 pagesPoster PapersLeonardo RodríguezNo ratings yet
- Management of Plantar Heel Pain. A Best Practice Guide Informed by A Systematic Review, Expert Clinical Reasoning and Patient ValuesDocument14 pagesManagement of Plantar Heel Pain. A Best Practice Guide Informed by A Systematic Review, Expert Clinical Reasoning and Patient ValuesJesusNavarrete97No ratings yet
- Rotator Cuff Repair vs. Nonoperative Treatment - 2021 (Tema 3)Document12 pagesRotator Cuff Repair vs. Nonoperative Treatment - 2021 (Tema 3)Carlos NoronaNo ratings yet
- Cmar 10 2439Document9 pagesCmar 10 2439andrei vladNo ratings yet
- Time and Travel Burden Associated With Hexapod Assisted Correction of Lower Extremity DeformityDocument6 pagesTime and Travel Burden Associated With Hexapod Assisted Correction of Lower Extremity DeformityAthenaeum Scientific PublishersNo ratings yet
- Evaluation Hand in Trigger FingerDocument8 pagesEvaluation Hand in Trigger FingerJorge RamirezNo ratings yet
- Evaluation of An Interdisciplinary Screening Program For People With Parkinson Disease and Movement DisordersDocument10 pagesEvaluation of An Interdisciplinary Screening Program For People With Parkinson Disease and Movement DisordersAbu Faris Al-MandariNo ratings yet
- Clinimetric Analyses of The Modified Parkinson Activity Scale PDFDocument7 pagesClinimetric Analyses of The Modified Parkinson Activity Scale PDFdanielNo ratings yet
- AmputeeDocument7 pagesAmputeeneurodivertoNo ratings yet
- Elemento Termico Pra Establecer RiesgoDocument18 pagesElemento Termico Pra Establecer RiesgoMAURICIO MELONo ratings yet
- Perilunate Dislocations: Cme Information and DisclosuresDocument5 pagesPerilunate Dislocations: Cme Information and DisclosuresClaudio LimaNo ratings yet
- How To Use Article Diagnostic Test PDFDocument3 pagesHow To Use Article Diagnostic Test PDFzahrara90No ratings yet
- Fractura Radio Distal ReviewDocument5 pagesFractura Radio Distal ReviewUn SerNo ratings yet
- Heel-Rise Test in The Assessment of Individuals With Peripheral Arterial Occlusive DiseaseDocument7 pagesHeel-Rise Test in The Assessment of Individuals With Peripheral Arterial Occlusive Diseaseputra batosaiNo ratings yet
- Goetz CG, Et Al - The Unified Parkinson's Disease Rating Scale (UPDRS) Status and RecommendationsDocument13 pagesGoetz CG, Et Al - The Unified Parkinson's Disease Rating Scale (UPDRS) Status and Recommendationsursula_ursulaNo ratings yet
- Development of The ATAQ-IPf 2010Document9 pagesDevelopment of The ATAQ-IPf 2010Julio HuapayaNo ratings yet
- Reliability and Validity of Dual-Task Mobility Assessments in People With Chronic Stroke - PMCDocument29 pagesReliability and Validity of Dual-Task Mobility Assessments in People With Chronic Stroke - PMCSavannah GreyNo ratings yet
- Exercise Therapy in The Non-Operative Treatment of Full-Thickness Rotator Cuff Tears: A Systematic ReviewDocument44 pagesExercise Therapy in The Non-Operative Treatment of Full-Thickness Rotator Cuff Tears: A Systematic ReviewJavier Alonso Jara CánovasNo ratings yet
- Valor Pronostico Del Llenado CapilarDocument13 pagesValor Pronostico Del Llenado Capilarwilington26No ratings yet
- Heel-Rise Test in The Assessment of Individuals With Peripheral Arterial Occlusive DiseaseDocument11 pagesHeel-Rise Test in The Assessment of Individuals With Peripheral Arterial Occlusive Diseaseputra batosaiNo ratings yet
- BMJ g1687 FullDocument12 pagesBMJ g1687 FullJaumeNo ratings yet
- Guidelines For Perioperative Care in Bariatric SurgeryDocument23 pagesGuidelines For Perioperative Care in Bariatric Surgerymilagros12300No ratings yet
- TIDie RDocument12 pagesTIDie RBruno SantinonNo ratings yet
- Bo Hannon 2016Document5 pagesBo Hannon 2016rafaelorcyNo ratings yet
- (2009) LAVIGNE - The Functional Outcome of Hip Resurfacing and Large-Head THA Is The SameDocument12 pages(2009) LAVIGNE - The Functional Outcome of Hip Resurfacing and Large-Head THA Is The SameSandro Luiz Machado CarvalhoNo ratings yet
- TIDieR InglésDocument12 pagesTIDieR InglésPG TavoNo ratings yet
- Validity and Reliability of The Novel Thyroid-Specific Quality of Life Questionnaire, ThyproDocument7 pagesValidity and Reliability of The Novel Thyroid-Specific Quality of Life Questionnaire, ThyproPriyanaka NaraniyaNo ratings yet
- Esicm 2020Document612 pagesEsicm 2020FERNANDODEJESUS LOPEZ RUEDANo ratings yet
- Guidelines For The Treatment of Venous UlcersDocument14 pagesGuidelines For The Treatment of Venous UlcerssorinmoroNo ratings yet
- Diagnosis and Treatment of Worker-Related Musculoskeletal Disorders of The Upper Extremity OmbroDocument705 pagesDiagnosis and Treatment of Worker-Related Musculoskeletal Disorders of The Upper Extremity OmbroDouglas GarciaNo ratings yet
- Tailored Communication For Older Patients With Cancer Using ClusterDocument7 pagesTailored Communication For Older Patients With Cancer Using ClusterDiego andisNo ratings yet
- 2019 Article 448Document8 pages2019 Article 448Diego andisNo ratings yet
- Coping Styles in PacientesDocument11 pagesCoping Styles in PacientesDiego andisNo ratings yet
- Association Between Different Coping Styles and Healt - RelatedDocument10 pagesAssociation Between Different Coping Styles and Healt - RelatedDiego andisNo ratings yet
- Pathfinder Template FormDocument7 pagesPathfinder Template FormWan Ahmad Fadir100% (1)
- Root Cause AnalysisDocument2 pagesRoot Cause Analysisjjjj000No ratings yet
- Benchmark Reflection of Professional Development SessionDocument5 pagesBenchmark Reflection of Professional Development Sessionapi-475628377No ratings yet
- FIOP II ASSIGNMENT (Bareera-2100)Document15 pagesFIOP II ASSIGNMENT (Bareera-2100)Yashika Jain -63No ratings yet
- Robert DavidsonDocument32 pagesRobert DavidsonRazaNo ratings yet
- Lesson Plan: The Threats of Unsustainable Consumption and ProductionDocument3 pagesLesson Plan: The Threats of Unsustainable Consumption and Productionapi-346534803No ratings yet
- NLC Lesson PlanDocument2 pagesNLC Lesson PlanMalou Sojon100% (1)
- Campaña Covid en ArgentinaDocument9 pagesCampaña Covid en ArgentinaSMIBA MedicinaNo ratings yet
- The Impact of Female Empowerment in Advertising (Femvertising)Document7 pagesThe Impact of Female Empowerment in Advertising (Femvertising)1569 BidishaNo ratings yet
- Outsourcing in Operations ManagementDocument10 pagesOutsourcing in Operations ManagementInaraMirza-zadeNo ratings yet
- Revision Sheet (Statistics & Probability) : MarkschemeDocument18 pagesRevision Sheet (Statistics & Probability) : MarkschemeDev SethiNo ratings yet
- Challenges and Difficulties Encountered by Teachers in The Conduct of Educational Research: Basis For Teachers' Enhancement ProgramDocument11 pagesChallenges and Difficulties Encountered by Teachers in The Conduct of Educational Research: Basis For Teachers' Enhancement Programtin del rosarioNo ratings yet
- Holy Angel University Bachelor of Science in Accountancy (Bsa)Document2 pagesHoly Angel University Bachelor of Science in Accountancy (Bsa)Louis Even MacaspacNo ratings yet
- Medical Software Business PlanDocument48 pagesMedical Software Business PlancssdNo ratings yet
- Syllabus - VTU - MBA - Research Methodology and Strategic Management PDFDocument2 pagesSyllabus - VTU - MBA - Research Methodology and Strategic Management PDFPreethi Gopalan100% (1)
- Autosar Pro ConsDocument8 pagesAutosar Pro ConsYaseen YaseenNo ratings yet
- Background of The ProblemDocument48 pagesBackground of The ProblemEmmanuel Geronimo100% (2)
- Chapter 4 Market and Demand AnalysisDocument36 pagesChapter 4 Market and Demand Analysismubasheralijamro54% (13)
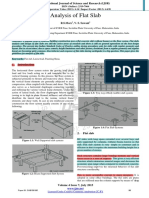
- Analysis of Flat Slab - CompleteDocument4 pagesAnalysis of Flat Slab - Completemariyam khanNo ratings yet
- Summer Training ReportDocument116 pagesSummer Training ReportSonam SinghNo ratings yet
- Banana WiltDocument29 pagesBanana WiltMarshtoNo ratings yet
- Dual Processes in Reasoning? : University College LondonDocument14 pagesDual Processes in Reasoning? : University College LondonAnna Carolina Velozo NaderNo ratings yet
- 2201 Engagement PlanningDocument7 pages2201 Engagement PlanningdeeptimanneyNo ratings yet
- Chapter Four Research ProposalDocument26 pagesChapter Four Research Proposaldawit demeNo ratings yet
- PhaneendraDocument1 pagePhaneendraPrateek NagariaNo ratings yet
- Which One of The Following Is True About CensusDocument4 pagesWhich One of The Following Is True About CensusgenanewNo ratings yet
- Research Paper On Mental HealthDocument63 pagesResearch Paper On Mental HealthDivyajeet SinghNo ratings yet
- The New Concept in Civil FieldDocument15 pagesThe New Concept in Civil FieldNaveen Kumar KaddsNo ratings yet
- The Advantages & Disadvantages of Employee Empowerment: Involved EmployeesDocument7 pagesThe Advantages & Disadvantages of Employee Empowerment: Involved EmployeesThimme Gowda RGNo ratings yet
- Development and Validation of A Brand Trust ScaleDocument59 pagesDevelopment and Validation of A Brand Trust ScalewardakhanNo ratings yet