You might also like
- ZF 6HP21 ZF 6HP21X 6 SPEED RWD (Full Electronic Control) : BMW Code 1071 030 XXX BMW Code 1071 050 XXXDocument6 pagesZF 6HP21 ZF 6HP21X 6 SPEED RWD (Full Electronic Control) : BMW Code 1071 030 XXX BMW Code 1071 050 XXXToks Vilmantas100% (1)
- 10 Professional Practices - Prepare BCM CertificationDocument60 pages10 Professional Practices - Prepare BCM CertificationAdneya AudhiNo ratings yet
- GTX 3XX Part 23: AML STC Installation ManualDocument367 pagesGTX 3XX Part 23: AML STC Installation ManuallocoboeingNo ratings yet
- PapelDocument8 pagesPapelignacio galindoNo ratings yet
- Midface Clinical Anatomy and Regional Approaches.31Document17 pagesMidface Clinical Anatomy and Regional Approaches.31Andreas Chandra100% (3)
- Equipco FleetMgtDocument25 pagesEquipco FleetMgtrajadas777No ratings yet
- Variations and Claims Procedure: Practical Issues: A Paper Given at The SCL (Gulf) Conference in Dubai On 20th March 2011Document14 pagesVariations and Claims Procedure: Practical Issues: A Paper Given at The SCL (Gulf) Conference in Dubai On 20th March 2011Mohamed El AbanyNo ratings yet
- 3D Printing in MedicalDocument4 pages3D Printing in MedicalAadil KakarNo ratings yet
- Issues in Economics TodayDocument559 pagesIssues in Economics TodayNikhil Singhal71% (7)
- Bok:978 3 030 96874 8Document533 pagesBok:978 3 030 96874 8CarlosBaculimaNo ratings yet
- ASME B31.8 Riser CalcDocument23 pagesASME B31.8 Riser Calcisrar khan100% (2)
- Ethics Case Digest CompleteDocument56 pagesEthics Case Digest Completeevealyn.gloria.wat20100% (3)
- Common Complications in Endodontics Prevention and Management by Priyanka Jain (Eds.)Document294 pagesCommon Complications in Endodontics Prevention and Management by Priyanka Jain (Eds.)ruacondungmanhNo ratings yet
- Field Density TestDocument12 pagesField Density TestRoyNo ratings yet
- Trim Labiaplasty.8Document2 pagesTrim Labiaplasty.8Afif MansorNo ratings yet
- Railway Ticketing DocumentationDocument243 pagesRailway Ticketing Documentationsakthipet1100% (1)
- AWS Operational Excellence Pillar PDFDocument23 pagesAWS Operational Excellence Pillar PDFCharley RajNo ratings yet
- RTN 950 Configuration GuideDocument1,722 pagesRTN 950 Configuration GuideWilliam Fernandes100% (2)
- Cast and Splint Immobilization - Complications PDFDocument11 pagesCast and Splint Immobilization - Complications PDFcronoss21No ratings yet
- Ues Final Published Urology PDFDocument29 pagesUes Final Published Urology PDFKamran MovassaghiNo ratings yet
- Effect of Negative Pressure Wound Therapy On Wound Healing: Current Problems in SurgeryDocument31 pagesEffect of Negative Pressure Wound Therapy On Wound Healing: Current Problems in SurgeryriniNo ratings yet
- Evidence-Based Strategies To Reduce Postoperative Complications in Plastic SurgeryDocument10 pagesEvidence-Based Strategies To Reduce Postoperative Complications in Plastic SurgeryAmanda HodelNo ratings yet
- Management Thumb Tip Injuries - Germann - JHS 2015Document9 pagesManagement Thumb Tip Injuries - Germann - JHS 2015Professeur Christian DumontierNo ratings yet
- Adhesive and Sealant Interfaces For General Surgery ApplicationsDocument14 pagesAdhesive and Sealant Interfaces For General Surgery ApplicationsDiana Petrea100% (1)
- Reply Secondary Neck Lift and The Importance Of.57Document2 pagesReply Secondary Neck Lift and The Importance Of.57MikeunoeNo ratings yet
- Ijmse 2015 Vol 2 Issue 4 Page 154-166Document13 pagesIjmse 2015 Vol 2 Issue 4 Page 154-166Sarra TekayaNo ratings yet
- Filler Rhinoplasty: Evidence, Outcomes, and ComplicationsDocument3 pagesFiller Rhinoplasty: Evidence, Outcomes, and ComplicationsАндрей ПетровNo ratings yet
- HHS Public Access: Cutaneous Imaging Technologies in Acute Burn and Chronic Wound CareDocument20 pagesHHS Public Access: Cutaneous Imaging Technologies in Acute Burn and Chronic Wound CareandreeaNo ratings yet
- Updates in Aesthetic Surgery II 1112 Article.1Document2 pagesUpdates in Aesthetic Surgery II 1112 Article.1Hải Dương MinhNo ratings yet
- Interstitial High-Dose-Rate Gynecologic Brachytherapy: Clinical Workflow Experience From Three Academic InstitutionsDocument10 pagesInterstitial High-Dose-Rate Gynecologic Brachytherapy: Clinical Workflow Experience From Three Academic Institutions980Denis FernandezNo ratings yet
- Clinical Application of Instant 3D Printed Cast Versus Polymer Orthosis in The Treatment of Colles Fracture: A Randomized Controlled TrialDocument9 pagesClinical Application of Instant 3D Printed Cast Versus Polymer Orthosis in The Treatment of Colles Fracture: A Randomized Controlled Trialkanni.40976No ratings yet
- Advances in Periodontal Surgery: A Clinical Guide to Techniques and Interdisciplinary ApproachesFrom EverandAdvances in Periodontal Surgery: A Clinical Guide to Techniques and Interdisciplinary ApproachesSalvador NaresNo ratings yet
- Interventional Treatment of Wounds: A Modern Approach for Better OutcomesFrom EverandInterventional Treatment of Wounds: A Modern Approach for Better OutcomesDennis P. OrgillNo ratings yet
- Penetrating Duodenal Trauma: A 19-Year Experience: AAST Continuing Medical Education ArticleDocument5 pagesPenetrating Duodenal Trauma: A 19-Year Experience: AAST Continuing Medical Education ArticleLaiz DecampsNo ratings yet
- Preoperative Planning in Primary Total Knee ArthroplastyDocument12 pagesPreoperative Planning in Primary Total Knee ArthroplastytripodegrandeNo ratings yet
- Thesis Topics in General Surgery DownloadDocument4 pagesThesis Topics in General Surgery Downloadjqcoplhld100% (1)
- Article 5Document5 pagesArticle 5bestin athappillyNo ratings yet
- Can You Tell The Difference Round Vs Anatomical Implants A Real Time Global BallotDocument2 pagesCan You Tell The Difference Round Vs Anatomical Implants A Real Time Global BallotMinh Thư DươngNo ratings yet
- Quality of Life Assessment of Patients Utilizing Orbital Implant Supported ProsthesesDocument6 pagesQuality of Life Assessment of Patients Utilizing Orbital Implant Supported ProsthesesBagis Emre GulNo ratings yet
- Hickson 2018Document12 pagesHickson 2018Luigi Paolo Zapata DelgadoNo ratings yet
- Evolution in Tissue Expander Design For Breast Reconstruction: Technological Innovation To Optimize Patient OutcomesDocument10 pagesEvolution in Tissue Expander Design For Breast Reconstruction: Technological Innovation To Optimize Patient OutcomesFauzi Novia Isnaening TyasNo ratings yet
- Journal Pre-Proof: Journal of Plastic, Reconstructive & Aesthetic SurgeryDocument10 pagesJournal Pre-Proof: Journal of Plastic, Reconstructive & Aesthetic SurgeryMaitham IsmailNo ratings yet
- 10 1016@j Jamcollsurg 2020 02 031Document34 pages10 1016@j Jamcollsurg 2020 02 031Residentes Cirugia Udea 2016No ratings yet
- 3D CD - Three Days Complete Denture Technique For Compromised Geriatric PatientsDocument5 pages3D CD - Three Days Complete Denture Technique For Compromised Geriatric PatientsMaulida Dara HarjantiNo ratings yet
- CX Preprotesica OOODocument4 pagesCX Preprotesica OOOMich ReynosoNo ratings yet
- Canula+versos+agulha+em+cada Ver+2Document16 pagesCanula+versos+agulha+em+cada Ver+2raquelhxNo ratings yet
- Incluir en Justificación El Rapido Crecimiento Del Uso de Las Herramientas de Marketing DigitalDocument2 pagesIncluir en Justificación El Rapido Crecimiento Del Uso de Las Herramientas de Marketing DigitalMaestria en Administración 2021No ratings yet
- Literature Review Open FractureDocument8 pagesLiterature Review Open Fractureea3h1c1p100% (1)
- Minimal Invasiveness in Soft Tissue Augmentation at Dental Implants A Systematic Review and Meta-Analysis of Patient-Reported OutcomeDocument17 pagesMinimal Invasiveness in Soft Tissue Augmentation at Dental Implants A Systematic Review and Meta-Analysis of Patient-Reported Outcomemahesh kumarNo ratings yet
- The Subcutaneous Inverted Looped Horizontal Mattress Stitch A Novel and EDocument3 pagesThe Subcutaneous Inverted Looped Horizontal Mattress Stitch A Novel and Elriveros540No ratings yet
- Rhomboid Flap For Pilonidal Sinus - Our ExperienceDocument5 pagesRhomboid Flap For Pilonidal Sinus - Our ExperienceKhalidHussainNo ratings yet
- Ams 7 245Document5 pagesAms 7 245dayanaNo ratings yet
- Laser Management of ScarsFrom EverandLaser Management of ScarsKayvan ShokrollahiNo ratings yet
- PRP An Mandibular FractureDocument6 pagesPRP An Mandibular Fracture6hd6mnrzw2No ratings yet
- MainDocument5 pagesMaindark_PinchoNo ratings yet
- A-Plasty Scar Revision TechniqueDocument2 pagesA-Plasty Scar Revision TechniqueAlpagan YıldırımNo ratings yet
- Maxillary Protraction With Rapid Maxillary Expansion and Facemask Versus Skeletal Anchorage With Mini-Implants in Class III Patients A Non-Randomized Clinical TrialDocument11 pagesMaxillary Protraction With Rapid Maxillary Expansion and Facemask Versus Skeletal Anchorage With Mini-Implants in Class III Patients A Non-Randomized Clinical TrialMariana SantosNo ratings yet
- Thesis Bone RegenerationDocument8 pagesThesis Bone RegenerationPaperWritingServicesForCollegeStudentsOverlandPark100% (2)
- Clin Adv Periodontics - 2022 - Kashani - Incision Free Coronally Advanced Flap With Subepithelial Connective Tissue GraftDocument10 pagesClin Adv Periodontics - 2022 - Kashani - Incision Free Coronally Advanced Flap With Subepithelial Connective Tissue GraftAlzahraa AhmedNo ratings yet
- Advanced Smile Diagnostics Using CAD. CAM Mock Ups. Irina. Leido PDFDocument19 pagesAdvanced Smile Diagnostics Using CAD. CAM Mock Ups. Irina. Leido PDFsolangeNo ratings yet
- 00014Document5 pages00014Dauz ArashNo ratings yet
- Comparison of Two Incision Designs For Surgical ReDocument5 pagesComparison of Two Incision Designs For Surgical ReSooraj SNo ratings yet
- Borgia Gonzalo, Ravecca Tabaré, Fumero Miriam, Pebé PabloDocument13 pagesBorgia Gonzalo, Ravecca Tabaré, Fumero Miriam, Pebé PabloJaime Angel Ortiz DiazNo ratings yet
- Bed Sore 2Document4 pagesBed Sore 2Zymmer100% (1)
- Novel Microneedle BandedgeDocument15 pagesNovel Microneedle BandedgePratik WANKHEDENo ratings yet
- OPD JOURNAL REACTION Sutures Vs StaplesDocument4 pagesOPD JOURNAL REACTION Sutures Vs StaplesSoniaMarieBalanayNo ratings yet
- Informatics Quality Change Final Draft ZellerDocument7 pagesInformatics Quality Change Final Draft Zellerapi-536681273No ratings yet
- Plastic Surgery Research Paper TopicsDocument5 pagesPlastic Surgery Research Paper Topicsxwrcmecnd100% (1)
- Scherer 2008Document12 pagesScherer 2008Jorge Luis Corcho AcostaNo ratings yet
- A Retained Surgical Item Is Any Instrument Used Then Unintentionally Left Inside The Patient After Completion of A Surgical ProcedureDocument8 pagesA Retained Surgical Item Is Any Instrument Used Then Unintentionally Left Inside The Patient After Completion of A Surgical ProcedureRoy MutahiNo ratings yet
- Treatment of Nipple Hypertrophy by A Simplified Reduction TechniqueDocument7 pagesTreatment of Nipple Hypertrophy by A Simplified Reduction TechniqueАндрей ПетровNo ratings yet
- 1 s2.0 S2214541920300213 MainDocument4 pages1 s2.0 S2214541920300213 MainWinda KhosasiNo ratings yet
- Post Insertion Complaints of Removable Dental Prostheses: October 2018Document5 pagesPost Insertion Complaints of Removable Dental Prostheses: October 2018Javaria IftekharNo ratings yet
- Protego 2020 - 21Document429 pagesProtego 2020 - 21jleonclau1No ratings yet
- Defect Analysis and Prevention For Software Process Quality ImprovementDocument6 pagesDefect Analysis and Prevention For Software Process Quality ImprovementSrinivas Rg KNo ratings yet
- Profile SRC Projects PDFDocument52 pagesProfile SRC Projects PDFrengarajan82No ratings yet
- ICDL Module 1 FinalDocument131 pagesICDL Module 1 Finalyousef100% (1)
- Challenges of International BusinessDocument4 pagesChallenges of International BusinessRikesh SapkotaNo ratings yet
- MSDS-Manganese DioxideDocument7 pagesMSDS-Manganese DioxideMuhammad BahauddinNo ratings yet
- USBee Air-Gap Covert-Channel Via Electromagnetic Emission From USBDocument5 pagesUSBee Air-Gap Covert-Channel Via Electromagnetic Emission From USBRanim JaafarNo ratings yet
- Mpo - Compressor MotorDocument2 pagesMpo - Compressor MotorroelNo ratings yet
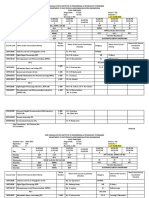
- III B.Tech TT 2021-22Document5 pagesIII B.Tech TT 2021-22ravikumar rayalaNo ratings yet
- Multimedia Project Team RolesDocument16 pagesMultimedia Project Team RolesrinaNo ratings yet
- Toyo - Soal Dasar Akuntansi UTS - Gasal 2122Document2 pagesToyo - Soal Dasar Akuntansi UTS - Gasal 2122Dita nNo ratings yet
- BtwinlogDocument6 pagesBtwinlogBhavdeep SharmaNo ratings yet
- GEL 4100 PIDE CompactLogixDocument16 pagesGEL 4100 PIDE CompactLogixAndreina Sofía Nuñez VargasNo ratings yet
- Cylinder: Data Sheet No. 2.29.001E-1Document10 pagesCylinder: Data Sheet No. 2.29.001E-1sancsa_74No ratings yet
- Module 2 - Intrinsic ValuationDocument11 pagesModule 2 - Intrinsic ValuationLara Camille CelestialNo ratings yet
- Marsha Mellow Doesn T Care Whether She Consumes in Period 1Document1 pageMarsha Mellow Doesn T Care Whether She Consumes in Period 1trilocksp SinghNo ratings yet
- ERP Implementation: Assignment No 1 By: Syed Hasan Ali Shah 02-111162-213 Bba 8Document5 pagesERP Implementation: Assignment No 1 By: Syed Hasan Ali Shah 02-111162-213 Bba 8Abdur-Rehman QureshiNo ratings yet