You might also like
- MigraineDocument6 pagesMigraineNatália CândidoNo ratings yet
- TX EstadomigrañosoDocument14 pagesTX EstadomigrañosoGerardoLiraMendozaNo ratings yet
- A14 2002febGallagherS58 73 2Document16 pagesA14 2002febGallagherS58 73 2Zahra Ahmed AlzaherNo ratings yet
- Migraine and The Scope of HomeopathyDocument6 pagesMigraine and The Scope of HomeopathyDiego RodriguezNo ratings yet
- Pharmacological MigraineDocument5 pagesPharmacological MigraineSofia RomeroNo ratings yet
- Prophylaxis of Migraine Headache: The CaseDocument8 pagesProphylaxis of Migraine Headache: The CaseRo KohnNo ratings yet
- Intravenous Treatment of Migraine: Sait Ashina, Russell K. PortenoyDocument5 pagesIntravenous Treatment of Migraine: Sait Ashina, Russell K. PortenoyJess MelMedNo ratings yet
- Prolonged Abuse of Vasograin Tablets: 10.5005/jp-Journals-10067-0014Document2 pagesProlonged Abuse of Vasograin Tablets: 10.5005/jp-Journals-10067-0014Pratipal SinghNo ratings yet
- Dor de Cabeça IIDocument11 pagesDor de Cabeça IIElisaLadagaNo ratings yet
- Jurnal Migrain Asam ValproatDocument5 pagesJurnal Migrain Asam ValproatcynthiaramaNo ratings yet
- Manejo de La Migraña en Adultos. Tratamiento FarmacologicoDocument19 pagesManejo de La Migraña en Adultos. Tratamiento FarmacologicoGabriel Josué Alaña UrdanetaNo ratings yet
- 2017 Article 592Document17 pages2017 Article 592Shivam BhadauriaNo ratings yet
- Migraine: By: B K PandaDocument19 pagesMigraine: By: B K PandapandabijoyNo ratings yet
- Chronic Daily HeadacheDocument1 pageChronic Daily HeadacheGriggrogGingerNo ratings yet
- Contents 2019 Neurologic-ClinicsDocument4 pagesContents 2019 Neurologic-ClinicsAghie vlogNo ratings yet
- New England Journal of Medicine Volume 383 Issue 19 2020 (Doi 10.1056 - NEJMra1915327) Ropper, Allan H. Ashina, Messoud - MigraineDocument11 pagesNew England Journal of Medicine Volume 383 Issue 19 2020 (Doi 10.1056 - NEJMra1915327) Ropper, Allan H. Ashina, Messoud - MigraineMarija Sekretarjova100% (1)
- Maju Jurnal MigrainDocument7 pagesMaju Jurnal MigrainRosyid PrasetyoNo ratings yet
- 10.1177 1941874412439583 PDFDocument9 pages10.1177 1941874412439583 PDFindahNo ratings yet
- 0907 MigraineheadachesDocument2 pages0907 Migraineheadachesrena_psNo ratings yet
- Management of Migraine Headaches in A Chronic Pain Patient: A Case ReportDocument5 pagesManagement of Migraine Headaches in A Chronic Pain Patient: A Case Reporthenandwitafadilla28No ratings yet
- ANSWERS Vol 24.4 - Headache.2018 PDFDocument40 pagesANSWERS Vol 24.4 - Headache.2018 PDFmonica ortizNo ratings yet
- Nejmra 1915327Document11 pagesNejmra 1915327lakshminivas PingaliNo ratings yet
- AFP MigrañaDocument9 pagesAFP MigrañaJuaan AvilaNo ratings yet
- Emerging Drugs For Migraine Treatment: An UpdateDocument19 pagesEmerging Drugs For Migraine Treatment: An UpdateShivam BhadauriaNo ratings yet
- Headache: Migraine and Tension-Type HeadacheDocument12 pagesHeadache: Migraine and Tension-Type HeadacheLoren SangalangNo ratings yet
- Jurnal RadaDocument3 pagesJurnal RadaMuh Ridho AkbarNo ratings yet
- Nej MR A 1915327Document11 pagesNej MR A 1915327Noel Saúl Argüello SánchezNo ratings yet
- Management of Migraine Headache: An Overview of Current PracticeDocument7 pagesManagement of Migraine Headache: An Overview of Current Practicelili yatiNo ratings yet
- Practice: A 32-Year-Old Woman With HeadacheDocument2 pagesPractice: A 32-Year-Old Woman With HeadacheFeliNo ratings yet
- Ukdi Preparation I:: Neurogenic Pain Syndromes Peripheral Nerve DisordersDocument65 pagesUkdi Preparation I:: Neurogenic Pain Syndromes Peripheral Nerve DisordersFelicia SutarliNo ratings yet
- Menstrual Migrain Razutis 2015Document4 pagesMenstrual Migrain Razutis 2015Fifi RohmatinNo ratings yet
- Migrain Guidelines by MedscapeDocument18 pagesMigrain Guidelines by MedscapeAlfionita HardaniNo ratings yet
- Charles 2017Document9 pagesCharles 2017Aldebaran LadoNo ratings yet
- Headache - Seminars in NeurologyDocument7 pagesHeadache - Seminars in NeurologyandreaNo ratings yet
- Management of Migraine by DR GaneshDocument46 pagesManagement of Migraine by DR GaneshDr Ganeshgouda MajigoudraNo ratings yet
- Migraine: Diagnosis and Management: PathophysiologyDocument6 pagesMigraine: Diagnosis and Management: Pathophysiologykillingeyes177No ratings yet
- Preventive Therapy of Migraine: Pembimbing: Dr. Anyeliria Sutanto, SP.SDocument39 pagesPreventive Therapy of Migraine: Pembimbing: Dr. Anyeliria Sutanto, SP.SClaudia TariNo ratings yet
- Headache - Approach To The Adult PatientDocument28 pagesHeadache - Approach To The Adult PatientasasakopNo ratings yet
- Treatment of Migraine Attacks and Prevention of MiDocument40 pagesTreatment of Migraine Attacks and Prevention of MiHemi Amalia AmirullahNo ratings yet
- Ashkenazi 2007Document10 pagesAshkenazi 2007Ecaterina PozdircăNo ratings yet
- Lipton 2015Document14 pagesLipton 2015Javier Nicolas Pena DazaNo ratings yet
- BMC Neurology: Acute Treatment of Migraine. Breaking The Paradigm of MonotherapyDocument5 pagesBMC Neurology: Acute Treatment of Migraine. Breaking The Paradigm of MonotherapyFaradiba MaricarNo ratings yet
- Preventive Migraine TreatmentDocument20 pagesPreventive Migraine TreatmentNatalia BahamonNo ratings yet
- Migraine DiagnosisDocument7 pagesMigraine DiagnosisMariaAmeliaGoldieNo ratings yet
- Migraine Headache Prophylaxis - American Family PhysicianDocument16 pagesMigraine Headache Prophylaxis - American Family Physiciando leeNo ratings yet
- Migraine Headaches in A Nutshell: S Afr Fam Pract ReviewDocument3 pagesMigraine Headaches in A Nutshell: S Afr Fam Pract ReviewmaryNo ratings yet
- Efficacy of Adding Midazolam To Paracetamol in PaiDocument6 pagesEfficacy of Adding Midazolam To Paracetamol in PaiI Made AryanaNo ratings yet
- Weli 1 PDFDocument4 pagesWeli 1 PDFfahrihamzahNo ratings yet
- Randomized Study of Metoclopramide PlusDocument10 pagesRandomized Study of Metoclopramide PlusNovitNo ratings yet
- Patient Case PresentationDocument26 pagesPatient Case PresentationKathleen B BaldadoNo ratings yet
- Medication Overuse Headache: An Entrenched Idea in Need of ScrutinyDocument10 pagesMedication Overuse Headache: An Entrenched Idea in Need of ScrutinyLidio NetoNo ratings yet
- FavotriptanDocument12 pagesFavotriptansandyriaaaNo ratings yet
- Chronic Daily Headache - Challenges in TreatmentDocument4 pagesChronic Daily Headache - Challenges in TreatmenttutiNo ratings yet
- HeadacheDocument24 pagesHeadacheshayma khanNo ratings yet
- 2013 Pharmacology of Balance and DizzinessDocument14 pages2013 Pharmacology of Balance and Dizzinessfono.jcbertolaNo ratings yet
- Migraine EbmDocument10 pagesMigraine EbmAfni Panggar BesiNo ratings yet
- Diskusi Topik (Sakit Kepala) - Nafisa Zulpa Elhapidi-406202067Document34 pagesDiskusi Topik (Sakit Kepala) - Nafisa Zulpa Elhapidi-406202067nafisa zulfaelNo ratings yet
- Management of Intracranial Pain: Aliah Shivaan I Sara Anne William Sailo Aisyah Jayson Yuen Alice Hafizah Archan ADocument63 pagesManagement of Intracranial Pain: Aliah Shivaan I Sara Anne William Sailo Aisyah Jayson Yuen Alice Hafizah Archan AWilliam OngNo ratings yet
- Role of Triptans in The Management of Acute Migraine: A ReviewDocument7 pagesRole of Triptans in The Management of Acute Migraine: A ReviewAndreas NatanNo ratings yet
- Migraine: The Definitive Guide to Understanding and Managing Severe HeadachesFrom EverandMigraine: The Definitive Guide to Understanding and Managing Severe HeadachesNo ratings yet
- Dwnload Full Psychology of Criminal Behaviour A Canadian Perspective Canadian 2nd Edition Brown Test Bank PDFDocument36 pagesDwnload Full Psychology of Criminal Behaviour A Canadian Perspective Canadian 2nd Edition Brown Test Bank PDFslipknotdartoid0wdc100% (9)
- Cocaine and Other Sympathomimetics PDFDocument11 pagesCocaine and Other Sympathomimetics PDFLizeth GirónNo ratings yet
- Psychopathology NotesDocument16 pagesPsychopathology NotesAtiaNo ratings yet
- Fun Facts About BrainDocument3 pagesFun Facts About BrainBulcastoked TandagNo ratings yet
- Amphetamine, Anorexogenics and AnalepticsDocument20 pagesAmphetamine, Anorexogenics and AnalepticsShing Ming TangNo ratings yet
- Mood Disorders Short EssayDocument4 pagesMood Disorders Short EssayscholifyNo ratings yet
- Acupuncture Modern MedicineDocument400 pagesAcupuncture Modern MedicineRoberto Biglia100% (5)
- Fight The Obesity EpidemicDocument102 pagesFight The Obesity EpidemicJorianditha RamadhanNo ratings yet
- Contoh Reading Card Bahasa InggrisDocument8 pagesContoh Reading Card Bahasa InggrisWahyu BudimanNo ratings yet
- FAA Newcomer's Packet Online VersionDocument48 pagesFAA Newcomer's Packet Online VersionPeyton Brooke100% (4)
- Journal Pre-Proof: European Journal of PharmacologyDocument46 pagesJournal Pre-Proof: European Journal of PharmacologyMike RohrichNo ratings yet
- Albizzia The Tree of HappinessDocument4 pagesAlbizzia The Tree of HappinessslowhaNo ratings yet
- Autacoids: AntagonistsDocument37 pagesAutacoids: AntagonistsJayaNo ratings yet
- APPETITE: Physiological and Neurobiological AspectsDocument8 pagesAPPETITE: Physiological and Neurobiological AspectsTamara Souza RossiNo ratings yet
- Relert Tablets: 1. Qualitative and Quantitative CompositionDocument9 pagesRelert Tablets: 1. Qualitative and Quantitative Compositionddandan_2No ratings yet
- Presented By:-11081506 (Ridhi) 11081524 (Khushboo) 11081560 (Shiny) 11081542 (Sakshi)Document17 pagesPresented By:-11081506 (Ridhi) 11081524 (Khushboo) 11081560 (Shiny) 11081542 (Sakshi)Akanksha KapoorNo ratings yet
- Epidemiol Rev 2008 Nock 133 54Document22 pagesEpidemiol Rev 2008 Nock 133 54Maria Magdalena DumitruNo ratings yet
- Chronic Pain 1: SeriesDocument16 pagesChronic Pain 1: Seriesginamilena90No ratings yet
- Neurotoxicity of Ecstasy (MDMA) : An OverviewDocument10 pagesNeurotoxicity of Ecstasy (MDMA) : An OverviewArian JafariNo ratings yet
- Anatomy of An EpidemicDocument13 pagesAnatomy of An EpidemicCris RodriguesNo ratings yet
- B2B Psychopharmacology 2015Document128 pagesB2B Psychopharmacology 2015Soleil DaddouNo ratings yet
- Foods That Look Like Body Parts They're Good ForDocument7 pagesFoods That Look Like Body Parts They're Good Forkaravi schinias100% (1)
- Psychopathology AQA Psychology Alevel PowerpointDocument38 pagesPsychopathology AQA Psychology Alevel PowerpointBarbara GladyszNo ratings yet
- Off-Label Trazodone Prescription-Evidence, Benefits and RisksDocument9 pagesOff-Label Trazodone Prescription-Evidence, Benefits and RisksomarapesNo ratings yet
- Review: in The Search For Selective Ligands of 5-Ht, 5-HT and 5-Ht Serotonin ReceptorsDocument15 pagesReview: in The Search For Selective Ligands of 5-Ht, 5-HT and 5-Ht Serotonin ReceptorsAlegría LeeNo ratings yet
- Adrenergic Nervous SystemDocument71 pagesAdrenergic Nervous SystemsmbawasainiNo ratings yet
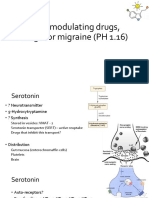
- 5-HT Modulating Drugs, Drugs For Migraine (PH 1.16)Document13 pages5-HT Modulating Drugs, Drugs For Migraine (PH 1.16)shruti sangwanNo ratings yet
- Lista BibliográficaDocument17 pagesLista BibliográficafernandaNo ratings yet
- IJOPP MalariaDocument62 pagesIJOPP MalariaSantanu MallikNo ratings yet
- 1-Dr. Samir El BadawyDocument83 pages1-Dr. Samir El BadawytarikeopsNo ratings yet