You might also like
- Psychic Development ManualDocument52 pagesPsychic Development Manualmagickmerlin100% (19)
- The Self Compassion Skills Workbook PDFDocument166 pagesThe Self Compassion Skills Workbook PDFIsna Rizki Primayanti100% (5)
- Self HarmWorkbook Vol1ADocument26 pagesSelf HarmWorkbook Vol1AJennifer Caussade75% (4)
- The Everything Guide to Cognitive Behavioral Therapy: Learn Positive and Mindful Techniques to Change Negative BehaviorsFrom EverandThe Everything Guide to Cognitive Behavioral Therapy: Learn Positive and Mindful Techniques to Change Negative BehaviorsRating: 3.5 out of 5 stars3.5/5 (4)
- Befriend Your Brain: A Young Person's Guide to Dealing with Anxiety, Depression, Anger, Freak-Outs, and TriggersFrom EverandBefriend Your Brain: A Young Person's Guide to Dealing with Anxiety, Depression, Anger, Freak-Outs, and TriggersRating: 5 out of 5 stars5/5 (2)
- Applications of EMG in Clinical and Sports MedicineDocument412 pagesApplications of EMG in Clinical and Sports Medicineteju1996coolNo ratings yet
- Cognitive Behavioral Therapy by Olivia Telford PDFDocument114 pagesCognitive Behavioral Therapy by Olivia Telford PDFnonimugo100% (4)
- The OCD CureDocument85 pagesThe OCD CureAlexandra Patrascoiu100% (1)
- How To Eliminate Negative Thinking - Learn To Control Your Thoughts, Overthinking, Negativity Bias, HealDocument172 pagesHow To Eliminate Negative Thinking - Learn To Control Your Thoughts, Overthinking, Negativity Bias, HeallindyloulindenNo ratings yet
- Your Life Can Be Better, Using Strategies for Adult ADHD, Second EditionFrom EverandYour Life Can Be Better, Using Strategies for Adult ADHD, Second EditionRating: 5 out of 5 stars5/5 (1)
- Brain Based Therapy For OCD A Workbook For Clinicians and Clients (John Arden, PHD)Document190 pagesBrain Based Therapy For OCD A Workbook For Clinicians and Clients (John Arden, PHD)shylajaNo ratings yet
- Depression and Low Mood: An NHS Self Help GuideDocument29 pagesDepression and Low Mood: An NHS Self Help GuideKristine Apostol RecanaNo ratings yet
- Causes and Remedies of Obsessive-Compulsive Disorder: The Key to Escape from self-made Prison (Workbook for Overcoming OCD)From EverandCauses and Remedies of Obsessive-Compulsive Disorder: The Key to Escape from self-made Prison (Workbook for Overcoming OCD)No ratings yet
- How To Stop NegativeDocument136 pagesHow To Stop NegativeSaeed Alzahrani100% (1)
- Summary of The Sleep Fix: Practical, Proven, and Surprising Solutions for Insomnia, Snoring, Shift Work, and More by Diane Macedo: Book Tigers Health and Diet SummariesFrom EverandSummary of The Sleep Fix: Practical, Proven, and Surprising Solutions for Insomnia, Snoring, Shift Work, and More by Diane Macedo: Book Tigers Health and Diet SummariesNo ratings yet
- Ankle FractureDocument11 pagesAnkle FracturecorsaruNo ratings yet
- My Life of Checking, Hiding, and Faking: How I Conquered the Hidden Torment of OCDFrom EverandMy Life of Checking, Hiding, and Faking: How I Conquered the Hidden Torment of OCDNo ratings yet
- The Everything Health Guide to OCD: Professional advice on handling anxiety, understanding treatment options, and finding the support you needFrom EverandThe Everything Health Guide to OCD: Professional advice on handling anxiety, understanding treatment options, and finding the support you needRating: 5 out of 5 stars5/5 (1)
- Our Self-Harm Workbook: Kati MortonDocument26 pagesOur Self-Harm Workbook: Kati Mortonaliahaniff100% (4)
- Compulsive Stereotypic and Displacement DisordersDocument5 pagesCompulsive Stereotypic and Displacement DisordersBrook Farm Veterinary CenterNo ratings yet
- Depression and Low MoodDocument40 pagesDepression and Low Moodfau fauNo ratings yet
- Pasta TripleDocument7 pagesPasta TripleLincoln GarciaNo ratings yet
- Rewire Your Brain: A Beginner's Guide to Cognitive Behavioral Therapy CBT - Change Your Thoughts, Change Your LifeFrom EverandRewire Your Brain: A Beginner's Guide to Cognitive Behavioral Therapy CBT - Change Your Thoughts, Change Your LifeNo ratings yet
- Edexcel As Biology Unit 1 Exam Revision NotesDocument19 pagesEdexcel As Biology Unit 1 Exam Revision Notesfockoffu100% (1)
- NLP Communication & conscious leadership: train your brain to top performanceFrom EverandNLP Communication & conscious leadership: train your brain to top performanceRating: 5 out of 5 stars5/5 (1)
- Breaking Free From OCD (Book, Salkovskis & Others, 2011)Document220 pagesBreaking Free From OCD (Book, Salkovskis & Others, 2011)Luisa fernanda Avila UrueñaNo ratings yet
- Journaling for Non-Journalers: Your expert guide to creating a journaling practice that works for youFrom EverandJournaling for Non-Journalers: Your expert guide to creating a journaling practice that works for youNo ratings yet
- The Blackmailer in Your Head: What To Do About Obsessive Compulsive DisorderFrom EverandThe Blackmailer in Your Head: What To Do About Obsessive Compulsive DisorderRating: 4 out of 5 stars4/5 (4)
- Expert Secrets - Cognitive Behavioral Therapy (CBT): The Ultimate Guide Made Simple to Overcome Anger Management, Anxiety, Depression, Insomnia, Negative Thinking, Panic, Phobias, Stress, and Worry!From EverandExpert Secrets - Cognitive Behavioral Therapy (CBT): The Ultimate Guide Made Simple to Overcome Anger Management, Anxiety, Depression, Insomnia, Negative Thinking, Panic, Phobias, Stress, and Worry!No ratings yet
- Kati Morton Self Harm Workbook Vol1 PDFDocument26 pagesKati Morton Self Harm Workbook Vol1 PDFFábioPedroso100% (1)
- Beating The BluesDocument4 pagesBeating The BlueshotaussieguyNo ratings yet
- Meditation Mind Tricks: Mindfulness Made EasyFrom EverandMeditation Mind Tricks: Mindfulness Made EasyRating: 3.5 out of 5 stars3.5/5 (2)
- 7 Thoughts to Live Your Life By: A Guide to the Happy, Peaceful, & Meaningful Life: Master Your Mind, Revolutionize Your Life, #10From Everand7 Thoughts to Live Your Life By: A Guide to the Happy, Peaceful, & Meaningful Life: Master Your Mind, Revolutionize Your Life, #10Rating: 5 out of 5 stars5/5 (1)
- NCP PsychosisDocument3 pagesNCP PsychosisKristian Karl Bautista Kiw-is100% (1)
- Self Care: Love Yourself: How to Embrace Self-Compassion, Body Love & Self Love for Life-Changing Wellness & Self-EsteemFrom EverandSelf Care: Love Yourself: How to Embrace Self-Compassion, Body Love & Self Love for Life-Changing Wellness & Self-EsteemNo ratings yet
- Steve Flowers, Mindful Path Through Shyness Workbook PDFDocument77 pagesSteve Flowers, Mindful Path Through Shyness Workbook PDFjhonpreston100% (1)
- List of Licenced PharmaciesDocument11 pagesList of Licenced PharmaciesMalvika TomarNo ratings yet
- My Recovery Work Journal: Recovering from a Mental Health CrisisFrom EverandMy Recovery Work Journal: Recovering from a Mental Health CrisisNo ratings yet
- Cognitive Behavioral Therapy Olivia TelfordDocument114 pagesCognitive Behavioral Therapy Olivia TelfordmikesoupNo ratings yet
- DR - Karach Oil Pulling TherapyDocument2 pagesDR - Karach Oil Pulling TherapyHritcu AndreiNo ratings yet
- Chicken Soup for the Soul: Think, Act, & Be Happy: How to Use Chicken Soup for the Soul Stories to Train Your Brain to Be Your Own TherapistFrom EverandChicken Soup for the Soul: Think, Act, & Be Happy: How to Use Chicken Soup for the Soul Stories to Train Your Brain to Be Your Own TherapistRating: 4 out of 5 stars4/5 (1)
- Commentary Biowaiver Monographs For Immediate Release Solid Oral Dosage Forms: PrednisoloneDocument20 pagesCommentary Biowaiver Monographs For Immediate Release Solid Oral Dosage Forms: PrednisolonePrisca WicitaNo ratings yet
- Inside Yourself: Tips and Tricks to restore and improve your mental healthFrom EverandInside Yourself: Tips and Tricks to restore and improve your mental healthNo ratings yet
- Your Personal Guidance System: Unlock the Door to the Universe and Experience the MagicFrom EverandYour Personal Guidance System: Unlock the Door to the Universe and Experience the MagicNo ratings yet
- Navigating Sleeplessness: How to Sleep Deeper and Better for LongerFrom EverandNavigating Sleeplessness: How to Sleep Deeper and Better for LongerNo ratings yet
- The OCD (OBSESSIVE-COMPULSIVE DISORDER) Workbook Skills, Techniques, and Exercises To Manage Anxiety, Compulsions And... (Beatrice W. Hanlon PHD (Hanlon PHD Etc.Document287 pagesThe OCD (OBSESSIVE-COMPULSIVE DISORDER) Workbook Skills, Techniques, and Exercises To Manage Anxiety, Compulsions And... (Beatrice W. Hanlon PHD (Hanlon PHD Etc.Nour Abou ZakiNo ratings yet
- Are You Happy: Everyday Happiness a Guide to Finding You: Are You HappyFrom EverandAre You Happy: Everyday Happiness a Guide to Finding You: Are You HappyNo ratings yet
- A Guide For Young Children: Come and MeetDocument12 pagesA Guide For Young Children: Come and MeetDoottyNo ratings yet
- 0 - Free From Ocd - Timothy SisemoreDocument96 pages0 - Free From Ocd - Timothy Sisemoremeeting.biomedicalNo ratings yet
- Alzheimer's Days Gone By: For Those Caring for Their Loved OnesFrom EverandAlzheimer's Days Gone By: For Those Caring for Their Loved OnesNo ratings yet
- What Isa Habit?Document3 pagesWhat Isa Habit?mekkawi99No ratings yet
- Easy Read Guide AnxietyDocument20 pagesEasy Read Guide AnxietysagonNo ratings yet
- 23-05-2018 011346916 - Intervention Modalities - Chapter 16Document26 pages23-05-2018 011346916 - Intervention Modalities - Chapter 16Bisan RatuishNo ratings yet
- Accumulation of Nitrate in Vegetables and Its Possible Implications To Human HealthDocument10 pagesAccumulation of Nitrate in Vegetables and Its Possible Implications To Human HealthJesus David Calderon GomezNo ratings yet
- Radiotherapy Physics and Principles of Radiotherapy: Q.P. Code: 801908Document12 pagesRadiotherapy Physics and Principles of Radiotherapy: Q.P. Code: 801908Sandhiya KNo ratings yet
- Understanding Insomnia - Felson, SDocument4 pagesUnderstanding Insomnia - Felson, SRoxan PacsayNo ratings yet
- Sexually Transmitted Diseases Treatment Guidelines, 2010 PDFDocument110 pagesSexually Transmitted Diseases Treatment Guidelines, 2010 PDFAzam GundalNo ratings yet
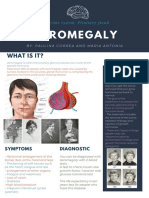
- Acromegaly: What Is It?Document1 pageAcromegaly: What Is It?Paulina CorreaaNo ratings yet
- Glaucoma & CataractDocument53 pagesGlaucoma & CataractBenita100% (1)
- Cotofana FrenteDocument10 pagesCotofana FrenteLorenzoNo ratings yet
- Chest Pain Low RiskDocument2 pagesChest Pain Low RiskWills Consulting LLCNo ratings yet
- Puerperal Psychosis: A Carer's Survival GuideDocument64 pagesPuerperal Psychosis: A Carer's Survival GuideGrace LNo ratings yet
- What Is Typhoid FeverDocument5 pagesWhat Is Typhoid FeverKameh Dani Adrian Wadzon'sNo ratings yet
- Cms High Risk MedicationsDocument8 pagesCms High Risk MedicationsMihai VladescuNo ratings yet
- Sarcomas Glandula MamariaDocument6 pagesSarcomas Glandula MamariaNelly ChacónNo ratings yet
- HKSIEM.2017.Peroxisomal Diseases WorkshopDocument42 pagesHKSIEM.2017.Peroxisomal Diseases WorkshopCalvin Yeow-kuan ChongNo ratings yet
- Inhibidores de La ECADocument16 pagesInhibidores de La ECAFarmaFMNo ratings yet
- Effectiveness of Myofunctional Therapy in Ankyloglossia: A Systematic ReviewDocument18 pagesEffectiveness of Myofunctional Therapy in Ankyloglossia: A Systematic Reviewmistic0No ratings yet
- 261 Final EvaluationDocument9 pages261 Final Evaluationapi-283888852No ratings yet
- Trigger Finger Injection PDFDocument2 pagesTrigger Finger Injection PDFGS NidhiNo ratings yet
- Fourth Stage of Labor1Document5 pagesFourth Stage of Labor1So FarNo ratings yet
- The Prevention and Cure Effects of Aspirin Eugenol Ester On Hyperlipidemia and Its MetabonomicsDocument108 pagesThe Prevention and Cure Effects of Aspirin Eugenol Ester On Hyperlipidemia and Its MetabonomicsKavisa GhoshNo ratings yet
- Antibiotik Profilaksis DR Eko Setijanto 06032020 EditDocument40 pagesAntibiotik Profilaksis DR Eko Setijanto 06032020 EditFitria AgustianiNo ratings yet