You might also like
- Puppets of Political Propaganda--Time to Pull Our Own StringsFrom EverandPuppets of Political Propaganda--Time to Pull Our Own StringsNo ratings yet
- Case Study The Stanford University SchoolDocument6 pagesCase Study The Stanford University Schoolaxv136100% (1)
- Bioweapon AttackDocument3 pagesBioweapon Attackta84288No ratings yet
- Leadership in Healthcare: Essential Values and Skills, Fourth EditionFrom EverandLeadership in Healthcare: Essential Values and Skills, Fourth EditionNo ratings yet
- The Affordable Care ActDocument7 pagesThe Affordable Care ActalexNo ratings yet
- Nurs FPX 4050 Assessment 1 Preliminary Care Coordination PlanDocument4 pagesNurs FPX 4050 Assessment 1 Preliminary Care Coordination PlanEmma Watson100% (1)
- Briefing Memo House Vaccine Hesitancy Hearing 2021.05.26Document7 pagesBriefing Memo House Vaccine Hesitancy Hearing 2021.05.26Stephen LoiaconiNo ratings yet
- Zero Harm in Health Care - Catalyst PDFDocument23 pagesZero Harm in Health Care - Catalyst PDFRicardo Espinoza LipaNo ratings yet
- Slide 1: Disaster Recovery Plan For Vila Health: Berke, Et Al., 2014)Document7 pagesSlide 1: Disaster Recovery Plan For Vila Health: Berke, Et Al., 2014)Ravi KumawatNo ratings yet
- Covid Operational Plan TemplateDocument6 pagesCovid Operational Plan TemplateEdwardNo ratings yet
- Main ethical issues in human subjects researchDocument4 pagesMain ethical issues in human subjects researchMarkLawrenceLanderoValdezNo ratings yet
- A ADN or BSN What Is The Difference (A)Document5 pagesA ADN or BSN What Is The Difference (A)adrianazeleNo ratings yet
- Stephen L. DeFelice On The Future of NutraceuticalsDocument9 pagesStephen L. DeFelice On The Future of NutraceuticalsDecrapitationNo ratings yet
- Charles Stack - Public Health Challenges of EpilepsyDocument1 pageCharles Stack - Public Health Challenges of Epilepsycstack3No ratings yet
- Healthcare Fraud Paper 1Document9 pagesHealthcare Fraud Paper 1api-609705358No ratings yet
- COVID-19 Vaccine Snapshot: Clark County, NevadaDocument4 pagesCOVID-19 Vaccine Snapshot: Clark County, NevadaKSNV News3LVNo ratings yet
- Brief Summary of Eric Shirt Vs Saddle Lake Cree Nation T-978-16Document2 pagesBrief Summary of Eric Shirt Vs Saddle Lake Cree Nation T-978-16Shannon M HouleNo ratings yet
- EHT For Athletes For Brain HealthDocument2 pagesEHT For Athletes For Brain HealthTracey Jorg RollisonNo ratings yet
- HASTING CENTER The Privacy Rule That's NotDocument11 pagesHASTING CENTER The Privacy Rule That's NotIon Arrieta ValeroNo ratings yet
- ASRM COVID-19 Vaccine GuidanceDocument4 pagesASRM COVID-19 Vaccine GuidancePatricia FernándezNo ratings yet
- Chapter 4Document21 pagesChapter 4Ahmad KhooryNo ratings yet
- Open Letter To Congress From Health Care Policy ExpertsDocument25 pagesOpen Letter To Congress From Health Care Policy ExpertsKFFHealthNewsNo ratings yet
- IDFI in ChinaDocument17 pagesIDFI in ChinaSuoh MikotoNo ratings yet
- Heart Disease Research Paper Final DraftDocument13 pagesHeart Disease Research Paper Final Draftapi-301442453No ratings yet
- Health Impact Framework Paper DraftDocument14 pagesHealth Impact Framework Paper Draftapi-449021066No ratings yet
- DOJ/Pence Reply To GohmertDocument14 pagesDOJ/Pence Reply To GohmertRebecca Harrington100% (1)
- Nnaples - Heart Disease Final Term PaperDocument11 pagesNnaples - Heart Disease Final Term Paperapi-523878990100% (1)
- HealthcareDocument9 pagesHealthcareapi-272097622No ratings yet
- Couden - Final Chikungunya Health Impact Framework PaperDocument15 pagesCouden - Final Chikungunya Health Impact Framework Paperapi-449016836100% (1)
- City of Gainesville Response in Opposition To PetitionDocument14 pagesCity of Gainesville Response in Opposition To Petitionryan turbevilleNo ratings yet
- Capstone Paper Summative FINAL VERSIONDocument10 pagesCapstone Paper Summative FINAL VERSIONoliviajuolaNo ratings yet
- Nurse Interview Leadership SkillsDocument8 pagesNurse Interview Leadership SkillsMaina PeterNo ratings yet
- 2018 Physician Compensation ReportDocument23 pages2018 Physician Compensation ReportPNo ratings yet
- Nevada Covid 19 Vaccine Playbook v3 Brief 011121Document11 pagesNevada Covid 19 Vaccine Playbook v3 Brief 011121Tony GarciaNo ratings yet
- Health Care USA Chapter 6Document46 pagesHealth Care USA Chapter 6David TurnerNo ratings yet
- Wellcome TrustDocument5 pagesWellcome TrustAuromic BeheraNo ratings yet
- Avandia - The Intimidation of Dr. John BuseDocument12 pagesAvandia - The Intimidation of Dr. John BuseVaccineInformation100% (1)
- Resume of Jens H. Kuhn, M.D./PH.D., PH.D., M.S., Lead VirologistDocument37 pagesResume of Jens H. Kuhn, M.D./PH.D., PH.D., M.S., Lead VirologistHarry the GreekNo ratings yet
- FDA 9 Letter Letter To President Obama 4-2-09 FINAL RedactedDocument6 pagesFDA 9 Letter Letter To President Obama 4-2-09 FINAL Redactedniagarasquare100% (1)
- The Nuremberg Code and Its Impact On Clinical ResearchDocument2 pagesThe Nuremberg Code and Its Impact On Clinical ResearchAmrita SinghNo ratings yet
- 4546 PaperDocument7 pages4546 Paperapi-437840576No ratings yet
- Declaration in Defense of Science and SecularismDocument7 pagesDeclaration in Defense of Science and SecularismSybok100% (1)
- Urschel - How To AnalyzeDocument4 pagesUrschel - How To Analyzek1988No ratings yet
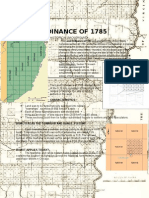
- Aphg Land Ordinance of 1785Document1 pageAphg Land Ordinance of 1785Anna Rojek100% (1)
- History of US HealthcareDocument12 pagesHistory of US HealthcareAntonio Abreu Jr.100% (1)
- Draft COVID-19 Vaccination Policy 2021Document3 pagesDraft COVID-19 Vaccination Policy 2021Jason Rantz100% (1)
- Health Care Disparities - Stereotyping and Unconscious BiasDocument39 pagesHealth Care Disparities - Stereotyping and Unconscious BiasCherica Oñate100% (1)
- Letter To CMSDocument7 pagesLetter To CMSWill SmithNo ratings yet
- Evidence Based RUADocument12 pagesEvidence Based RUAAsma AliNo ratings yet
- Organizational Behavior Case Part IIDocument5 pagesOrganizational Behavior Case Part IIAnubhav AgarwalNo ratings yet
- Bill Gates SummaryDocument10 pagesBill Gates SummaryArslanNo ratings yet
- HHS OIG Institutional Conflicts of Interes at NIH GranteesDocument32 pagesHHS OIG Institutional Conflicts of Interes at NIH GranteesBeverly TranNo ratings yet
- 13 Case Management Clinical PathwayDocument33 pages13 Case Management Clinical PathwayVenska TrianaNo ratings yet
- Hydrocortisone, Vitamin C, and Thiamine For The Treatment of Severe Sepsis and Septic ShockDocument10 pagesHydrocortisone, Vitamin C, and Thiamine For The Treatment of Severe Sepsis and Septic Shockmmmaw mmNo ratings yet
- Apa - Final Edition - The Ethical Dilemma of Healthcare in AmericaDocument9 pagesApa - Final Edition - The Ethical Dilemma of Healthcare in AmericaChristina Morales100% (1)
- CLONING TECHNOLOGYDocument25 pagesCLONING TECHNOLOGYMark Christian M. GonzagaNo ratings yet
- Report of The National Commission of Audit Phase 1.Document345 pagesReport of The National Commission of Audit Phase 1.SBS_NewsNo ratings yet
- 2022 MEDICATION ERROR Without ReferenceDocument133 pages2022 MEDICATION ERROR Without ReferenceSuhaime UEMNo ratings yet
- Letter From Doctors To APSDocument2 pagesLetter From Doctors To APSJustin HinkleyNo ratings yet
- SingDocument15 pagesSingkennedy othoroNo ratings yet
- 6429e9c7f03bf Informatics and Nursing Sensitive Quality Indicators - EditedDocument7 pages6429e9c7f03bf Informatics and Nursing Sensitive Quality Indicators - Editedkennedy othoroNo ratings yet
- 627e6e96954b6 Scope of Changes in Medical Education - EditedDocument6 pages627e6e96954b6 Scope of Changes in Medical Education - Editedkennedy othoroNo ratings yet
- Global Lightings Inc NotesDocument2 pagesGlobal Lightings Inc Noteskennedy othoroNo ratings yet
- Global Lightings Inc NotesDocument2 pagesGlobal Lightings Inc Noteskennedy othoroNo ratings yet
- Economic Analysis of A CurrentDocument7 pagesEconomic Analysis of A Currentkennedy othoroNo ratings yet
- 63afe140741ed Assessment 4 Instructions Informatics and Nursing Sensitive Quality IndicatorsDocument5 pages63afe140741ed Assessment 4 Instructions Informatics and Nursing Sensitive Quality Indicatorskennedy othoroNo ratings yet
- Literature Review DRAFTDocument9 pagesLiterature Review DRAFTkennedy othoroNo ratings yet
- 627a9e8637feb Financial Strategy Policy Bond Stock Questions and AnswersDocument9 pages627a9e8637feb Financial Strategy Policy Bond Stock Questions and Answerskennedy othoroNo ratings yet
- RubishDocument9 pagesRubishkennedy othoroNo ratings yet
- Qualys Gateway Service User GuideDocument39 pagesQualys Gateway Service User Guideshiv kumarNo ratings yet
- Que Bank PFMDocument5 pagesQue Bank PFMAmit KesharwaniNo ratings yet
- 2012 2013 Selection List For Government Sponsored StudentsDocument50 pages2012 2013 Selection List For Government Sponsored StudentsJohn Richard KasalikaNo ratings yet
- Memorandum of Agreement Between PartiesDocument3 pagesMemorandum of Agreement Between PartiesIsaac CursoNo ratings yet
- Animal Farm WebquestDocument8 pagesAnimal Farm Webquestapi-388806678No ratings yet
- CA FINAL First Priority Topics and Questions for MAY-22 ExamsDocument3 pagesCA FINAL First Priority Topics and Questions for MAY-22 ExamsasdNo ratings yet
- The 2015 IMD World Competitiveness ScoreboardDocument1 pageThe 2015 IMD World Competitiveness ScoreboardCarlos G.No ratings yet
- Population: Lebanon State of The Environment Report Ministry of Environment/LEDODocument7 pagesPopulation: Lebanon State of The Environment Report Ministry of Environment/LEDO420No ratings yet
- MKT 460 CH 1 Seh Defining Marketing For The 21st CenturyDocument56 pagesMKT 460 CH 1 Seh Defining Marketing For The 21st CenturyRifat ChowdhuryNo ratings yet
- Shell Drops Singapore Biofuels Project, Splits Renewables Energy IntelligenceDocument3 pagesShell Drops Singapore Biofuels Project, Splits Renewables Energy IntelligenceDjy DuhamyNo ratings yet
- Individual and Group Dynamics: Managing Diversity at Cityside Financial ServicesDocument7 pagesIndividual and Group Dynamics: Managing Diversity at Cityside Financial ServicesxxxNo ratings yet
- Peer Coaching Reflections and InsightsDocument8 pagesPeer Coaching Reflections and Insightsapi-269187486No ratings yet
- Maximizing Well-Being: Understanding UtilitarianismDocument15 pagesMaximizing Well-Being: Understanding UtilitarianismpalukNo ratings yet
- Annauniversity 2017 Mba Syllabus PDFDocument86 pagesAnnauniversity 2017 Mba Syllabus PDFSHAHULNo ratings yet
- Lesson Plan Post Modern ProtraitsDocument4 pagesLesson Plan Post Modern Protraitsapi-373758397No ratings yet
- 25 Posts (Open Merit) Provincial Management Service (PMS) Bs-17Document3 pages25 Posts (Open Merit) Provincial Management Service (PMS) Bs-17Raheel MunawarNo ratings yet
- BE01 Autobiography of Bhai Sahib Randhir Singh PDFDocument364 pagesBE01 Autobiography of Bhai Sahib Randhir Singh PDFGagan Singh PurewalNo ratings yet
- Abnormal Psychology Homework #4: Factors in Anxiety Disorders and Their TreatmentsDocument6 pagesAbnormal Psychology Homework #4: Factors in Anxiety Disorders and Their TreatmentsBrian ochiengNo ratings yet
- 07.01 Discussion EssayDocument3 pages07.01 Discussion EssayNguyễn Phương NgọcNo ratings yet
- DHAN BANK Final Approved COMPANY ListDocument84 pagesDHAN BANK Final Approved COMPANY Listcnu11082No ratings yet
- My Chemical RomanceDocument14 pagesMy Chemical RomanceCaruiza-chan Ragos100% (1)
- ACF-Dog - Cat Adoption ApplicationDocument5 pagesACF-Dog - Cat Adoption ApplicationBrittneyNo ratings yet
- Excerpts From The Book 'The Lawless State (The Crimes of The U.S. Intelligence Agencies) ' by Morton H. Halperin, Jerry Berman, Robert Borosage, Christine Marwick (1976)Document50 pagesExcerpts From The Book 'The Lawless State (The Crimes of The U.S. Intelligence Agencies) ' by Morton H. Halperin, Jerry Berman, Robert Borosage, Christine Marwick (1976)Anonymous yu09qxYCM100% (1)
- Clinicas de Derecho Ambiental Solicitan Negar Permiso de Construccion GasoductoDocument52 pagesClinicas de Derecho Ambiental Solicitan Negar Permiso de Construccion GasoductoDiálogoNo ratings yet
- Plato Girls PDFDocument30 pagesPlato Girls PDFJohn Reigh CatipayNo ratings yet
- Air Arabia 2017 Financial StatementsDocument62 pagesAir Arabia 2017 Financial StatementsRatika AroraNo ratings yet
- 5 Explanation of Pratikramana Sutra Uvasaggaharam StotraDocument83 pages5 Explanation of Pratikramana Sutra Uvasaggaharam Stotrajinavachan67% (3)
- Department of Education: Republic of The PhilippinesDocument2 pagesDepartment of Education: Republic of The PhilippinesKhalil Mae Labuyo100% (1)
- Viva Presentation: Ruchi Vinay ChavanDocument54 pagesViva Presentation: Ruchi Vinay ChavanPravin SarafNo ratings yet
- Hybrid Electric Vehicle: Ashley BuchananDocument9 pagesHybrid Electric Vehicle: Ashley BuchananSai Charan Sri HarshaNo ratings yet