You might also like
- Surgery Rotation NotesDocument18 pagesSurgery Rotation NotesNadiim Rajabalee100% (2)
- Crohn's Disease: Natural Healing Forever, Without MedicationFrom EverandCrohn's Disease: Natural Healing Forever, Without MedicationNo ratings yet
- Acute Cholecystitits, Choledocholithiasis and Acute CholangitisDocument16 pagesAcute Cholecystitits, Choledocholithiasis and Acute CholangitisKath de L'EnferNo ratings yet
- Etiology, Pathophysiology, and Clinical Manifestations of CholecystitisDocument3 pagesEtiology, Pathophysiology, and Clinical Manifestations of CholecystitisGerriNo ratings yet
- Gall StoneDocument38 pagesGall Stoneumay83% (6)
- Cholangitis and Cholecystitis (DR - Dr. Hery Djagat Purnomo, SpPD-KGEH)Document47 pagesCholangitis and Cholecystitis (DR - Dr. Hery Djagat Purnomo, SpPD-KGEH)Aditya SahidNo ratings yet
- Cholangitis: Reported By: R. DongaranDocument18 pagesCholangitis: Reported By: R. DongaranVishnu Karunakaran100% (1)
- Gallstone Disease and Acute Cholecystitis MADDocument21 pagesGallstone Disease and Acute Cholecystitis MADMuhammad AbdurrahmanNo ratings yet
- Tokyo Guideline 2018 - Cholecystitis (Small Size)Document69 pagesTokyo Guideline 2018 - Cholecystitis (Small Size)Muhammad RezaNo ratings yet
- Gallbladder - Gallstones and SurgeryDocument4 pagesGallbladder - Gallstones and SurgeryVinod MeenaNo ratings yet
- Cholangitis:: Presented By: S.Vishnu Priya (BSC Nursing) Tutor Bishop College of Nursing DharapuramDocument25 pagesCholangitis:: Presented By: S.Vishnu Priya (BSC Nursing) Tutor Bishop College of Nursing DharapuramVishnu PriyaNo ratings yet
- Chronic Liver Diseases & PLCCDocument56 pagesChronic Liver Diseases & PLCCibnbasheer100% (5)
- Acute Calculous CholecystitisDocument25 pagesAcute Calculous CholecystitisShankar LamichhaneNo ratings yet
- Biliary Tract DiseasesDocument35 pagesBiliary Tract DiseasesSoumya Ranjan PandaNo ratings yet
- CholedocholithiasisDocument3 pagesCholedocholithiasisAbdullah AlkharsNo ratings yet
- CholelithiasisDocument3 pagesCholelithiasisAbdullah AlkharsNo ratings yet
- CholecystitisDocument3 pagesCholecystitisAbdullah AlkharsNo ratings yet
- Understanding Disseminated Intravascular Coagulation (DIC)Document40 pagesUnderstanding Disseminated Intravascular Coagulation (DIC)Denise135No ratings yet
- Day 10. Choledocholitiasis, CholangitisDocument26 pagesDay 10. Choledocholitiasis, Cholangitisهنادي رازمNo ratings yet
- Sepsis: Nawaf AlruwailiDocument10 pagesSepsis: Nawaf AlruwailiNawaf AlrwuiliNo ratings yet
- Clinical Examination Obstructive Jaundice PrabedasDocument47 pagesClinical Examination Obstructive Jaundice PrabedasThompson CatNo ratings yet
- A Man With Diarrhea ColitisDocument5 pagesA Man With Diarrhea ColitisAriel MojanaNo ratings yet
- CholangitisDocument19 pagesCholangitisJohn mvulaNo ratings yet
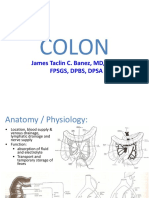
- Colon Dr. BanezDocument89 pagesColon Dr. BanezMiguel C. DolotNo ratings yet
- 1st Month AssessmentDocument43 pages1st Month AssessmentJonathan DavidNo ratings yet
- Acute CholangitisDocument9 pagesAcute CholangitisMike GNo ratings yet
- GB Lec SamiDocument43 pagesGB Lec SamiSajad Kadhim M DNo ratings yet
- SurgeryDocument146 pagesSurgeryNaren ShanNo ratings yet
- Acute PancreatitisDocument14 pagesAcute Pancreatitisعمار عارفNo ratings yet
- Diverticuloza DuodenalaDocument4 pagesDiverticuloza Duodenalaraluca77No ratings yet
- Acute Mesenteric Ischemia in COVID19 Patient - NAT FixedDocument10 pagesAcute Mesenteric Ischemia in COVID19 Patient - NAT FixedAde Tan RezaNo ratings yet
- Cholecystitis: Causes and PathologyDocument12 pagesCholecystitis: Causes and PathologySher KhanNo ratings yet
- CholelithiasisDocument8 pagesCholelithiasissaranya amuNo ratings yet
- Tg13: Updated Tokyo Guidelinesfor Acute CholecystitisDocument59 pagesTg13: Updated Tokyo Guidelinesfor Acute CholecystitisDeoValendraNo ratings yet
- Biliary System and Pancreatic DisorderDocument59 pagesBiliary System and Pancreatic DisorderAlda AdeliaNo ratings yet
- Caroli Syndrome: Medical ImagesDocument1 pageCaroli Syndrome: Medical ImagesEsmeralda Victoria ZdNo ratings yet
- Gallstone DiseaseDocument104 pagesGallstone DiseaseTan DanNo ratings yet
- JaundiceDocument30 pagesJaundiceNorakmal Andika YusriNo ratings yet
- Emergency GI 5th Yr Med Student 2019 NP RVDocument58 pagesEmergency GI 5th Yr Med Student 2019 NP RVPanda AhahaNo ratings yet
- Mesenteric Venous Thrombosis As A Rare Complication of Decompression SicknessDocument5 pagesMesenteric Venous Thrombosis As A Rare Complication of Decompression SicknessVan Cuong TranNo ratings yet
- Gallstone DiseaseDocument104 pagesGallstone DiseaseEma RadulescuNo ratings yet
- In The Name of God: Renal PathologyDocument56 pagesIn The Name of God: Renal PathologyIrsyad IzakiNo ratings yet
- General Surgery: (Gallbladder Disease)Document1 pageGeneral Surgery: (Gallbladder Disease)Matt100% (1)
- Surgery Class Biliary System SurgeryDocument69 pagesSurgery Class Biliary System SurgeryKashif BurkiNo ratings yet
- Id QuestionDocument67 pagesId QuestionRahul PradeepNo ratings yet
- Surgery CBL Module 4Document22 pagesSurgery CBL Module 4A SNo ratings yet
- Pages From Pages From STS-2Document42 pagesPages From Pages From STS-2mostaw safNo ratings yet
- Pages From STS-2 - 1Document43 pagesPages From STS-2 - 1mostaw safNo ratings yet
- 1 s2.0 S2210261221009731 MainDocument4 pages1 s2.0 S2210261221009731 Maintarmohamed.muradNo ratings yet
- Posttraumatic Hematuria With Pseudorenal Failure: A Diagnostic Lead For Diagnosing Intraperitoneal Bladder Rupture.Document4 pagesPosttraumatic Hematuria With Pseudorenal Failure: A Diagnostic Lead For Diagnosing Intraperitoneal Bladder Rupture.Ketan VagholkarNo ratings yet
- 1706509515565-Intestinal Diseases Congenital and Inflammatory LesionsDocument18 pages1706509515565-Intestinal Diseases Congenital and Inflammatory LesionsmyarjddbzNo ratings yet
- Acute CholecystitisDocument3 pagesAcute CholecystitisHardik JeenaNo ratings yet
- English ThemeDocument4 pagesEnglish ThemeJu BuNo ratings yet
- The Gallbladder Diseases Bile Duct StoneDocument69 pagesThe Gallbladder Diseases Bile Duct Stoneحميد حيدرNo ratings yet
- Biliary Cast Syndrome in Portal Hypertensive Biliopathy: Direct Cholangioscopic Findings and Endoscopic Therapy With Metal StentDocument3 pagesBiliary Cast Syndrome in Portal Hypertensive Biliopathy: Direct Cholangioscopic Findings and Endoscopic Therapy With Metal StentMarcelo CalossoNo ratings yet
- Curtis Peery MD: Sanford Health Surgical Associates Sioux Falls SD 605-328-3840Document26 pagesCurtis Peery MD: Sanford Health Surgical Associates Sioux Falls SD 605-328-3840Haruna BzakiNo ratings yet
- 1 s2.0 S0929644112000057 MainDocument4 pages1 s2.0 S0929644112000057 MainAisahNo ratings yet
- Untitled Notebook PDFDocument24 pagesUntitled Notebook PDFyoune6No ratings yet
- Clinical Guideline For Management of Acute Cholecystitis in AdultsDocument9 pagesClinical Guideline For Management of Acute Cholecystitis in AdultsGaby D'LuneNo ratings yet
- Clinical Guideline For Management of Acute Cholecystitis in AdultsDocument9 pagesClinical Guideline For Management of Acute Cholecystitis in AdultsPutria Rezki ArgathyaNo ratings yet
- Interpretation of Urine Testing ResultsDocument1 pageInterpretation of Urine Testing ResultsBigPharma HealtcareNo ratings yet
- Kegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungDocument47 pagesKegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungEfa FathurohmiNo ratings yet
- K-9 Infeksi Saluran KemihDocument45 pagesK-9 Infeksi Saluran KemihSyarifah FauziahNo ratings yet
- Biliary Atresia Digestive IVDocument13 pagesBiliary Atresia Digestive IVherdigunantaNo ratings yet
- Chole CystDocument12 pagesChole CystMoch NizamNo ratings yet
- Surgical JaundiceDocument19 pagesSurgical JaundiceNur InsyirahNo ratings yet
- Dannangxue (M-Le-23) : Gallbladder PointDocument1 pageDannangxue (M-Le-23) : Gallbladder Pointray72roNo ratings yet
- HIstology Lec - 13 GI Accessory GlandsDocument6 pagesHIstology Lec - 13 GI Accessory GlandsKevin C. AguilarNo ratings yet
- Surgery Class Biliary System SurgeryDocument69 pagesSurgery Class Biliary System SurgeryKashif BurkiNo ratings yet
- @ (White Paper - Cut-Off) RS85 - S-Shearwave Imaging LiverDocument10 pages@ (White Paper - Cut-Off) RS85 - S-Shearwave Imaging LiverHajjab AnasNo ratings yet
- Organ Function Test: Assessment of Functions of The OrgansDocument39 pagesOrgan Function Test: Assessment of Functions of The OrgansSri Abinash MishraNo ratings yet
- PancreasDocument6 pagesPancreasSimran Radhika JasujaNo ratings yet
- Acute Pancreatitis Hepatitis Infection: A. C. Rodriguez de Lope, G. San Miguel andDocument2 pagesAcute Pancreatitis Hepatitis Infection: A. C. Rodriguez de Lope, G. San Miguel andrezam6No ratings yet
- Attachment 181014031633Document35 pagesAttachment 181014031633lalalalalililililiNo ratings yet
- Liver Transplant in PuneDocument9 pagesLiver Transplant in PuneDr. Ninad DeshmukhNo ratings yet
- Surgical Anatomy of The Biliary TractDocument5 pagesSurgical Anatomy of The Biliary TracthoangducnamNo ratings yet
- Caroli Disease and CholangiocarcinomaDocument10 pagesCaroli Disease and CholangiocarcinomaDanielle Foster100% (1)
- Pathophysiology On Liver CirrhosisDocument39 pagesPathophysiology On Liver CirrhosisswaraNo ratings yet
- What Are Gallstones?: Lemuel Jay A. Segovia Grade 8-Peace Science Q4M1Document4 pagesWhat Are Gallstones?: Lemuel Jay A. Segovia Grade 8-Peace Science Q4M1Zarah Joyce SegoviaNo ratings yet
- Liver & Its Function.Document2 pagesLiver & Its Function.Niraj NiketNo ratings yet
- Pathophysiology: Adobe Stock, Licensed To Teachmeseries LTDDocument6 pagesPathophysiology: Adobe Stock, Licensed To Teachmeseries LTDNestaNo ratings yet
- Biliary Enteric BypassDocument25 pagesBiliary Enteric BypassAlexandru Ferdohleb100% (1)
- Poster-SessionsDocument105 pagesPoster-SessionsjishnuNo ratings yet
- Conceptual Study of Kamala (Jaundice)Document4 pagesConceptual Study of Kamala (Jaundice)Amit patelNo ratings yet
- V63N1A08Document7 pagesV63N1A08Carolina JozamiNo ratings yet
- Sirosis HatiDocument17 pagesSirosis HatiAndrianto WongkarNo ratings yet
- Acute Hepatitis ADocument1 pageAcute Hepatitis ACJMALNo ratings yet
- Path Pancreas McqsDocument4 pagesPath Pancreas McqsUu UuNo ratings yet
- Liver Function Tests (LFTS) : Git Block 1 Lecture Dr. Usman GhaniDocument26 pagesLiver Function Tests (LFTS) : Git Block 1 Lecture Dr. Usman Ghaniraanja2100% (1)
- Case - Based Pathophysiology of Type 1 Hyperlipidemia - Familial HyperchylomicronemiaDocument1 pageCase - Based Pathophysiology of Type 1 Hyperlipidemia - Familial HyperchylomicronemiaMae Rose Charlene MendozaNo ratings yet