You might also like
- Comprehensive Glossary of Legal Terms, Law Essentials: Essential Legal Terms Defined and AnnotatedFrom EverandComprehensive Glossary of Legal Terms, Law Essentials: Essential Legal Terms Defined and AnnotatedNo ratings yet
- The Van Conversion Bible - The Ultimate Guide To Converting A CampervanDocument170 pagesThe Van Conversion Bible - The Ultimate Guide To Converting A CampervanPil100% (3)
- Cross-Training: The Medical Assistant WorkbookFrom EverandCross-Training: The Medical Assistant WorkbookNo ratings yet
- Grammar WorksheetsDocument161 pagesGrammar WorksheetsKhánhNo ratings yet
- Records ReleaseDocument1 pageRecords ReleasechelseaNo ratings yet
- Supervising Claim Examiner: Passbooks Study GuideFrom EverandSupervising Claim Examiner: Passbooks Study GuideNo ratings yet
- Revamping An Integrated Hydrocracker and Lube Base Oil UnitDocument5 pagesRevamping An Integrated Hydrocracker and Lube Base Oil UnitVyacheslavNo ratings yet
- AngularJS Cheat SheetDocument3 pagesAngularJS Cheat SheetZulqarnain Hashmi100% (1)
- Philippine Multimodal Transportation and Logistics Industry Roadmap - Key Recommendations - 2016.04.14Document89 pagesPhilippine Multimodal Transportation and Logistics Industry Roadmap - Key Recommendations - 2016.04.14PortCalls50% (4)
- SC Health and Welfare FormDocument4 pagesSC Health and Welfare FormLeandro Tamayo14% (7)
- Lesson For SpreadsheetsDocument69 pagesLesson For SpreadsheetsCrisna Rivera PundanoNo ratings yet
- PWD Certificate FormatDocument1 pagePWD Certificate FormatSourav Panda100% (1)
- Liberian Medical Form PDFDocument2 pagesLiberian Medical Form PDFArpit Roy100% (2)
- NATIONAL VETERINARY BOARDS (NBE) (NVB) PART III - Physical Diagnosis, Medicine, Surgery: Passbooks Study GuideFrom EverandNATIONAL VETERINARY BOARDS (NBE) (NVB) PART III - Physical Diagnosis, Medicine, Surgery: Passbooks Study GuideNo ratings yet
- Annex C Doh Peme LB Rev0 5212013Document3 pagesAnnex C Doh Peme LB Rev0 5212013Leo II RomagosNo ratings yet
- Goat Farm ProjectDocument44 pagesGoat Farm ProjectVipin Kushwaha83% (6)
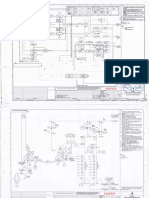
- Attachment 05 - BFD, ELD and P&I Diagrams-PearlDocument77 pagesAttachment 05 - BFD, ELD and P&I Diagrams-Pearlum er100% (1)
- Navi Mumbai C.A. ListDocument48 pagesNavi Mumbai C.A. ListManish Shetty67% (9)
- BSNL Project MBA NitishDocument92 pagesBSNL Project MBA NitishAnkitSingh0% (2)
- DTMF CoreDocument6 pagesDTMF Corevara prasadNo ratings yet
- Notice DR Aww Bkpu CDocument8 pagesNotice DR Aww Bkpu Cduttabishal712No ratings yet
- PWD Medical Certificate & Format For ScribeDocument2 pagesPWD Medical Certificate & Format For Scribehemantaduttaghy1No ratings yet
- App IIDocument1 pageApp IIPunjabi ListenNo ratings yet
- Scribe Declaration Form (Specified Disabilities)Document2 pagesScribe Declaration Form (Specified Disabilities)itishkakaralcNo ratings yet
- Medical CertificateDocument2 pagesMedical CertificateBhem Fernandez RomeroNo ratings yet
- Appendix A Certificate For Physical Limitation For PWBD Candidate INI CET PG July 2021Document1 pageAppendix A Certificate For Physical Limitation For PWBD Candidate INI CET PG July 2021suryadev s24No ratings yet
- Pre AuthorizationForPertrochantericFractureDocument2 pagesPre AuthorizationForPertrochantericFracturepatrickarilloNo ratings yet
- Data Privacy Consent:: General Evaluation FormDocument2 pagesData Privacy Consent:: General Evaluation FormIreish Mae RutaNo ratings yet
- FINAL CAT-III ADVT (2022) Final - 43-EndDocument4 pagesFINAL CAT-III ADVT (2022) Final - 43-EndjackNo ratings yet
- ENCLOSURESDocument13 pagesENCLOSURESnidhi sharmaNo ratings yet
- Acfrogbo ZR Yavmao RZ No1aftdazyjfq 7lqb Pnhtkqb6m5dp1xcygg2b38 Ifk8cvklo40xcq2j5uqxtb5jwzvgrwzssliqzlyuxdwzplaglu597wcdop8igqqDocument3 pagesAcfrogbo ZR Yavmao RZ No1aftdazyjfq 7lqb Pnhtkqb6m5dp1xcygg2b38 Ifk8cvklo40xcq2j5uqxtb5jwzvgrwzssliqzlyuxdwzplaglu597wcdop8igqqKhay Gillesania MasulaNo ratings yet
- Instruction For PWD PWBDDocument4 pagesInstruction For PWD PWBDselvaraj sNo ratings yet
- Disablity Certificate FormatDocument2 pagesDisablity Certificate FormatSudeshana JainNo ratings yet
- Liberia Ok Physical Examination ReportcertDocument2 pagesLiberia Ok Physical Examination ReportcertRicardo AquinoNo ratings yet
- Certificates and FormatsDocument12 pagesCertificates and FormatsAnimesh PriyadarshiNo ratings yet
- Federal Staff Relief Fund FormDocument1 pageFederal Staff Relief Fund Formkazmi_jeNo ratings yet
- Hsslive RPWD Annexure 5Document1 pageHsslive RPWD Annexure 5abhaianil24No ratings yet
- PWD Format1Document2 pagesPWD Format1Divakar Maurya100% (1)
- AbndgjdksvdkkdjDocument4 pagesAbndgjdksvdkkdjEn KayNo ratings yet
- IMA FormDocument3 pagesIMA FormSandeep OdelaNo ratings yet
- Cost of Application Form As Given in Notification (Non-Refundable.)Document5 pagesCost of Application Form As Given in Notification (Non-Refundable.)srikanthk_wilshireNo ratings yet
- Claim Form Lcpsea2018Document3 pagesClaim Form Lcpsea2018Rince RioNo ratings yet
- Senior Residents & Senior Demonstrators - Annexure 1 & IIDocument3 pagesSenior Residents & Senior Demonstrators - Annexure 1 & IIsarath6872No ratings yet
- Persons With Disabilities (PWD) Using The Services of A ScribeDocument3 pagesPersons With Disabilities (PWD) Using The Services of A Scribevedant patil. div ANo ratings yet
- Proforma For PH CertificateDocument2 pagesProforma For PH CertificateDivakar MauryaNo ratings yet
- GMCH Faculty App Nov12Document1 pageGMCH Faculty App Nov12nareshjangra397No ratings yet
- MYRO HR Checklist & Disclosure Statement Ver 1.7 JUN19Document2 pagesMYRO HR Checklist & Disclosure Statement Ver 1.7 JUN19soheilfozhanNo ratings yet
- MAP Application Form (Rev20230719)Document3 pagesMAP Application Form (Rev20230719)Jen EugenioNo ratings yet
- Instructions For MBBS Admissions For 2014-2015Document17 pagesInstructions For MBBS Admissions For 2014-2015Avinash GowdaNo ratings yet
- Appendix-I Application Form Officers Training Academy, Gaya (Bihar) - 823005Document4 pagesAppendix-I Application Form Officers Training Academy, Gaya (Bihar) - 823005SaiiNo ratings yet
- MQ 2nd Phase Principal Letter 2023Document5 pagesMQ 2nd Phase Principal Letter 2023RAMESH BABUNo ratings yet
- Notification Kolkata Port Trust Assistant Manager PostsDocument11 pagesNotification Kolkata Port Trust Assistant Manager PostsNeha SharmaNo ratings yet
- Indian Provisional Permanent RegistrationDocument8 pagesIndian Provisional Permanent RegistrationUdhayashankar DhayalanNo ratings yet
- PH CertificateDocument1 pagePH Certificatethenmozhi thenmozhiNo ratings yet
- Scribe Notice 23112022Document4 pagesScribe Notice 23112022rajNo ratings yet
- Application Form: Professional Regulation CommissionDocument1 pageApplication Form: Professional Regulation CommissionAnonymous wYyVjWTVibNo ratings yet
- Annex A - Informed ConsentNov2020Document3 pagesAnnex A - Informed ConsentNov2020Raul Jr. BlasabasNo ratings yet
- Application For The para Medical Recruitment in The Esi Hospital Sanathnagar Hyderabad - 500038Document4 pagesApplication For The para Medical Recruitment in The Esi Hospital Sanathnagar Hyderabad - 500038Mudavath RajuNo ratings yet
- InterviewDocument4 pagesInterviewas9345667No ratings yet
- Contract Basis 2023 AugDocument4 pagesContract Basis 2023 AugHimanshu DhimanNo ratings yet
- Certificate No - 1: (By OC Unit/Army Personnel Branch/DSS & A Board/Record .Office)Document5 pagesCertificate No - 1: (By OC Unit/Army Personnel Branch/DSS & A Board/Record .Office)Sushim KumarNo ratings yet
- Jose Rizal University: ODC Form 1BDocument3 pagesJose Rizal University: ODC Form 1BJonieP84No ratings yet
- F 006 Admission Form 2023Document2 pagesF 006 Admission Form 2023EJ “EJ” RoseteNo ratings yet
- Scribe Instruction MtsDocument3 pagesScribe Instruction MtsBhargav VekariaNo ratings yet
- Jose Rizal University: ODC Form 1CDocument3 pagesJose Rizal University: ODC Form 1CJonieP84No ratings yet
- Annexures: Annexure - IDocument35 pagesAnnexures: Annexure - IAarav DhingraNo ratings yet
- Consent For Mental Health Records Search: List Prior Addresses For Past 10 YearsDocument1 pageConsent For Mental Health Records Search: List Prior Addresses For Past 10 YearsJOSEPH MONTESNo ratings yet
- Oil and Natural Gas Corporation Limited Western Onshore Basin: Vadodara Walk in Interview For Medics and Paramedics On Contractual BasisDocument3 pagesOil and Natural Gas Corporation Limited Western Onshore Basin: Vadodara Walk in Interview For Medics and Paramedics On Contractual BasisAbhinav KumarNo ratings yet
- Application Form RBI Bank Medical Consultant PostsDocument2 pagesApplication Form RBI Bank Medical Consultant PostsNeha SharmaNo ratings yet
- California Notary Public Study Guide with 7 Practice Exams: 280 Practice Questions and 100+ Bonus Questions IncludedFrom EverandCalifornia Notary Public Study Guide with 7 Practice Exams: 280 Practice Questions and 100+ Bonus Questions IncludedNo ratings yet
- Orthopedics Instruments - 1Document21 pagesOrthopedics Instruments - 1Chetanya aggarwalNo ratings yet
- Surgery Short CasesDocument25 pagesSurgery Short CasesChetanya aggarwalNo ratings yet
- Aiats Topic Wise Schedule Class 10Document1 pageAiats Topic Wise Schedule Class 10Chetanya aggarwalNo ratings yet
- Solutions AIATS Foundation-2018 Test-1B Class-09 (23!07!2017)Document7 pagesSolutions AIATS Foundation-2018 Test-1B Class-09 (23!07!2017)Chetanya aggarwalNo ratings yet
- The Comparison and Evaluation of Carrying Angle of Elbow With Anthropometric Measurements in Both SexesDocument5 pagesThe Comparison and Evaluation of Carrying Angle of Elbow With Anthropometric Measurements in Both SexesChetanya aggarwalNo ratings yet
- Statement of Facts:: State of Adawa Vs Republic of RasasaDocument10 pagesStatement of Facts:: State of Adawa Vs Republic of RasasaChristine Gel MadrilejoNo ratings yet
- Aditya Birla Sun Life Insurance Secureplus Plan: Dear MR Kunjal Uin - 109N102V02Document7 pagesAditya Birla Sun Life Insurance Secureplus Plan: Dear MR Kunjal Uin - 109N102V02kunjal mistryNo ratings yet
- National Geographic - April 2020 PDFDocument160 pagesNational Geographic - April 2020 PDFIbn ZubairNo ratings yet
- Di MCB DB Pricelist01!07!2018Document1 pageDi MCB DB Pricelist01!07!2018saurabhjerps231221No ratings yet
- Ultra Wideband TechnologyDocument21 pagesUltra Wideband TechnologyAzazelNo ratings yet
- Pivacare Preventive-ServiceDocument1 pagePivacare Preventive-ServiceSadeq NeiroukhNo ratings yet
- LESSON - STEM-based Research ProblemsDocument49 pagesLESSON - STEM-based Research ProblemsLee JenoNo ratings yet
- Global Review of Enhances Geothermal SystemDocument20 pagesGlobal Review of Enhances Geothermal SystemKatherine RojasNo ratings yet
- Financial Analysis of OGDCLDocument16 pagesFinancial Analysis of OGDCLsehrish_sadaqat7873100% (1)
- Guidelines For New Students - 2022Document14 pagesGuidelines For New Students - 2022Ria Faye PaderangaNo ratings yet
- Geometric Entities: Basic Gear TerminologyDocument5 pagesGeometric Entities: Basic Gear TerminologyMatija RepincNo ratings yet
- COST v. MMWD Complaint 8.20.19Document64 pagesCOST v. MMWD Complaint 8.20.19Will HoustonNo ratings yet
- Pepsico IncDocument26 pagesPepsico IncYKJ VLOGSNo ratings yet
- Print Design Business Model CanvasDocument3 pagesPrint Design Business Model CanvasMusic Da LifeNo ratings yet
- Transport StrikeDocument9 pagesTransport StrikeYsrael Von ArcillaNo ratings yet
- How To Configure VFD - General - Guides & How-Tos - CoreELEC ForumsDocument13 pagesHow To Configure VFD - General - Guides & How-Tos - CoreELEC ForumsJemerald MagtanongNo ratings yet
- Nelson/Salmo Pennywise March 15, 2016Document48 pagesNelson/Salmo Pennywise March 15, 2016Pennywise PublishingNo ratings yet
- Juniper M5 M10 DatasheetDocument6 pagesJuniper M5 M10 DatasheetMohammed Ali ZainNo ratings yet
- Sampling PowerpointDocument21 pagesSampling PowerpointMuhammad Furqan Aslam AwanNo ratings yet
- UT Dallas Syllabus For cs4341.001.09s Taught by (Moldovan)Document4 pagesUT Dallas Syllabus For cs4341.001.09s Taught by (Moldovan)UT Dallas Provost's Technology GroupNo ratings yet